
Abstract
Background:
The presence of bone marrow edema (BME) on magnetic resonance imaging (MRI) has been used to evaluate for bone stress injuries in athletes.
Purpose:
To examine the prevalence of MRI findings, including BME, in a single male collegiate basketball team before and after a single season and to assess its association with clinically symptomatic metatarsal bone stress injuries.
Study Design:
Cohort Study; Level of evidence, 3.
Methods:
A total of 16 men on a single collegiate basketball team (mean age, 20.0 ± 1.8 years) underwent 1.5-T MRI focused on both midfeet during the preseason, and 13 underwent repeat MRI during the postseason. MRI findings included the presence of BME and the radiographic classification of the bone stress injury (grades 1-4). Injury surveillance performed by athletic trainers was used to identify metatarsal bone stress injuries over the course of the season.
Results:
Preseason MRI demonstrated metatarsal BME in 5 of the 16 participants, and postseason MRI demonstrated metatarsal BME in 4 of the 13 participants. All 4 of the participants with postseason BME had MRI findings of BME in the same metatarsals. Compared to those without BME, participants with metatarsal BME had a shorter history of basketball exposure (preseason: 10.4 ± 4.1 vs 14.2 ± 1.9 years, respectively [P = .023]; postseason: 9.6 ± 4.1 vs 14.0 ± 2.1 years, respectively [P = .024]), and those with postseason BME had started playing at an older age (9.8 ± 4.3 vs 6.2 ± 1.6 years, respectively; P = .050). The preseason MRI classification for metatarsals included grade 1 (n = 3), followed by grades 2 and 3 (n = 2 each). In the 4 participants with postseason MRI findings, the grade increased from 1 to 4 in 1 participant and was stable in the other 3. No participants were diagnosed clinically with a metatarsal bone stress injury during the season. BME of the sesamoids was identified in 6 participants, who trended toward being older (21.0 ± 2.2 vs 19.4 ± 1.3 years, respectively; P < .10), with the abnormalities persisting on postseason MRI in all players.
Conclusion:
Collegiate male basketball players may have a high prevalence of BME, often without associated symptoms. The absence of foot pain or a corresponding diagnosis of a metatarsal bone stress injury in this study suggests that MRI findings of BME in asymptomatic athletes should be interpreted with caution.
A bone stress injury is a common form of an overuse injury in athletes, including basketball players. The mechanism of a bone stress injury has been proposed as the accumulation of microtrauma that can coalesce to develop a fracture line, commonly referred to as a stress fracture. 19 Studies 5,6 on the incidence of stress fractures across sports have identified basketball as having a high rate of injuries starting at younger ages. Across 25 collegiate sports, men’s basketball had the second highest rate of bone stress injuries by athletic exposure. 17 In that investigation, the metatarsal was the most common anatomic site of bone stress injuries, comprising 59.6% of total bone stress injuries sustained. 17 A separate investigation of the National Basketball Association (NBA) identified 76 bone stress injuries sustained by 75 athletes over the 2005 to 2015 seasons. 13 The majority of bone stress injuries (n = 42; 55%) were localized to the foot, with 14 injuries sustained at the fifth metatarsal. All fifth metatarsal stress fractures were managed with surgery; however, a large proportion of players (6/14) were subsequently unable to return to sport.
Magnetic resonance imaging (MRI) is increasingly used for evaluating the presence and severity of a bone stress injury. The higher sensitivity of marrow and soft tissue abnormalities compared to radiography and the lack of ionizing radiation have made MRI the method of choice in evaluating bone stress injuries in athletes. 8 Additionally, criteria have been proposed to determine the severity of a bone stress injury using MRI, and a higher grade of injury may be prognostic for a longer time to return to play. 12 The original MRI grading scale was proposed by Fredericson et al 8 to evaluate tibial bone stress injuries. Subsequent studies have expanded this system to grade bone stress injuries in other anatomic locations, including the metatarsals. 16 A common feature of these grading systems is examining the presence of bone marrow edema (BME). The presence of BME on fluid-sensitive MRI sequences localized to the site of pain is used to identify bone stress injuries. However, BME has been shown to reflect bone turnover, changes that may represent either adaptive remodeling or the presence of an injury. 18
Findings of BME on MRI have been described in studies of active populations at risk for bone stress injuries including the military and runners. 4,9,14 However, while MRI is very sensitive, the presence of BME may not correspond with pain to confirm a clinical injury. While basketball is a popular sport with a high rate of bone stress injuries, no studies to date have evaluated the presence of BME in collegiate players over the course of their season, and no prior study has determined whether MRI findings of BME during the preseason may identify those who sustain subsequent bone stress injuries.
The purpose of this study was to examine the prevalence of MRI findings used in determining the grade of a bone stress injury during the preseason and postseason in a single male collegiate basketball team and to assess its association with clinically symptomatic metatarsal bone stress injuries. We hypothesized that a proportion of basketball players would have BME of the metatarsal bones and that not all players with BME or findings meeting imaging criteria for grading a metatarsal bone stress injury would have clinical correlates of a bone stress injury.
Methods
Study Design and Participants
The study protocol was approved by the Partners Institutional Review Board. Members of a single National Collegiate Athletic Association Division III male collegiate basketball team were recruited to participate. Study personnel visited the school and presented details on study participation. Written informed consent was obtained from each athlete before participation. There were 18 members of the basketball team initially enrolled in the study. Of these, 16 participants underwent preseason MRI of both feet, and 13 underwent postseason MRI of both feet. The CONSORT flowchart in Figure 1 depicts the observational, prospective cohort design of this study.

CONSORT diagram of participant inclusion.
Surveys
Each participant completed a series of online surveys hosted by Research Electronic Data Capture (REDCap). REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture, (2) audit trails for tracking data manipulation and export procedures, (3) automated export procedures for seamless data downloads to common statistical packages, and (4) procedures for data integration and interoperability with external sources. 10,11 We recorded participant age at enrollment, the age at which each began to play basketball, and the level of participation in basketball as well as in other sports.
The surveys included whether each participant had a prior diagnosis of a bone stress injury based on reports of stress reactions or stress fractures of the lower extremity. The surveys also included the anatomic location, the number of injuries, who made the diagnosis (eg, physician, other medical personnel), and if any imaging was performed to confirm the diagnosis. To account for other factors that may influence bone health, including diet and sleep, each participant was queried regarding whether he was a vegetarian and whether he had any prior diagnoses of an eating disorder or disordered eating. The average number of calcium-containing foods consumed daily as well as the use and dose of calcium and vitamin D supplementation were recorded. Finally, each participant completed the 16-item Athlete Sleep Screening Questionnaire 3 to identify average hours of sleep per night, and 5 of its items were used to generate the Sleep Difficulty Score. 3
Magnetic Resonance Imaging
Each participant underwent preseason MRI between October 13, 2019, and October 17, 2019. A second MRI examination was performed during the postseason between March 1, 2020, and March 11, 2020, representing imaging conducted, on average, 2 weeks after the last game of the season. MRI of bilateral feet, focused on the metatarsals, was performed on a 1.5-T MRI system (Espree; Siemens) with a dedicated ankle coil using sagittal short tau inversion recovery (STIR) (repetition time/echo time: 3180/36 ms; flip angle: 180°) and axial long-axis T1-weighted sequences (repetition time/echo time: 450-534/100 milliseconds; 3-mm thickness; 0.5-mm interslice gap; field of view: 110-150 mm2; bandwidth: 150 Hz).
MRI scans were analyzed by a board-certified, fellowship-trained musculoskeletal radiologist (M.A.B.). The presence of BME was identified, and imaging findings in a given metatarsal were classified using a modified version of the MRI grading scale described by Fredericson et al
8
and Arendt et al,
1,2
as follows (Figure 2): Grade 1: mild marrow edema on STIR images (but not T1-weighted images) or mild periosteal edema. Grade 2: moderate marrow edema on STIR images (but not T1-weighted images) or moderate periosteal edema. Grade 3: severe marrow edema or severe periosteal edema on both STIR and T1-weighted images (in the same location) but without a discrete fracture line. Grade 4: severe marrow edema or severe periosteal edema with a fracture line on either T1-weighted or STIR images.
We assessed the 5 metatarsals as well as the hallux sesamoid bones. In addition, the BME cross-sectional area (mm2) was calculated for each metatarsal. To identify lesions, each sequence was segmented manually, and the largest cross-sectional area was reported (OsiriX Version 3.2.1; www.osirix-viewer.com/index.html).

Sagittal short tau inversion recovery (STIR) magnetic resonance imaging of the metatarsals showing metatarsal bone marrow edema (arrows) consistent with a (A) grade 1, (B) grade 2, and (C) grade 3 injury.
Outcomes of Interest
The primary outcome of interest was the detection of MRI findings used to classify a metatarsal bone stress injury, including the presence of BME and MRI grading criteria (grades 1-4), that corresponded to the development of a clinically diagnosed metatarsal bone stress injury. An athletic trainer, present at each game and practice, recorded any injuries that occurred, including bone stress injuries. For the purpose of this study, a metatarsal bone stress injury was defined as having pain in the metatarsal region, corresponding to MRI findings, and was diagnosed by a physician. Other outcomes included BME (cm2) on preseason and postseason MRI and anatomic locations, including both metatarsal bones and other bones captured within the MRI protocol.
Statistical Analysis
The data were evaluated using R software (Version 3.6.3; R Core Team). Continuous variables were reported as the mean and standard deviation, and categorical variables were reported as the number and percentage of the total cohort. Differences between groups were assessed using a 2-tailed Student t test or Fisher exact test, with the threshold of significance set at P ≤ .05 and a trend defined as P < .10.
Results
Participants
The mean age of the 16 participants was 20.0 ± 1.8 years, and the mean age at initial participation in basketball was 7.0 ± 2.9 years (Table 1). Overall, 2 participants reported a history of bone stress injuries before study enrollment: one localized to the fibula and the other in the third metatarsal.
Participant Characteristics (n = 16) a
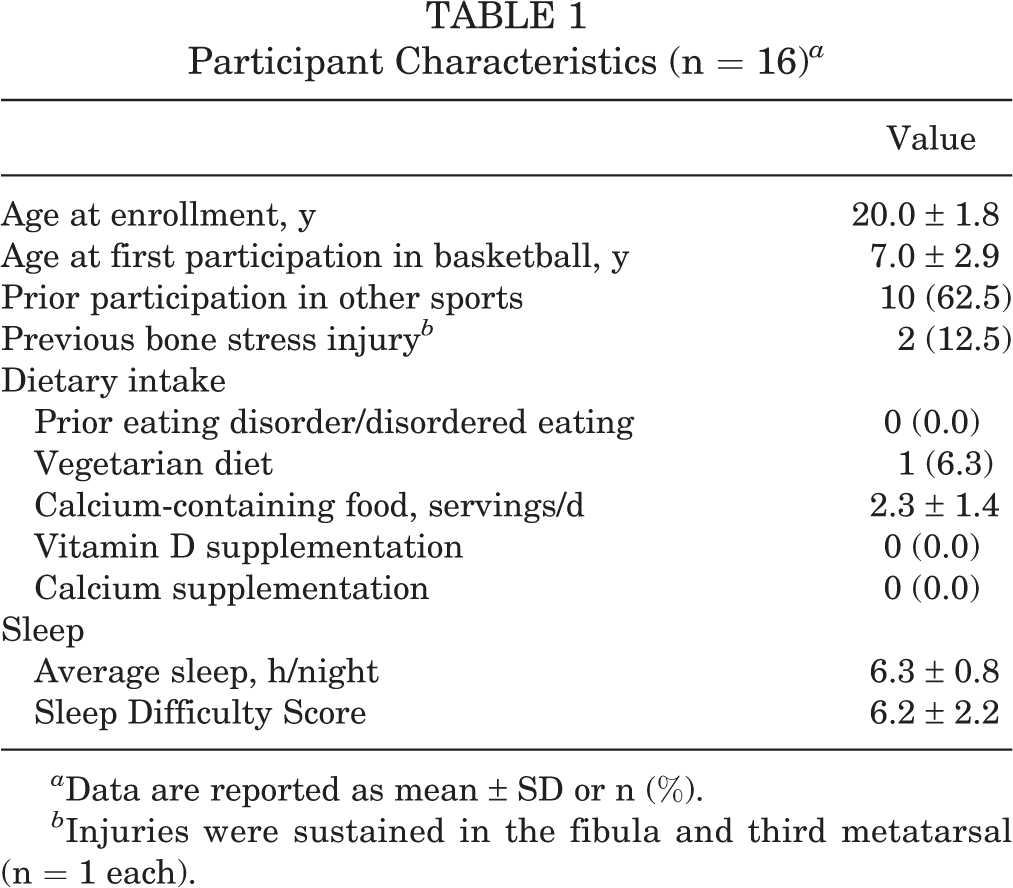
a Data are reported as mean ± SD or n (%).
b Injuries were sustained in the fibula and third metatarsal (n = 1 each).
BME of the Metatarsal on Preseason MRI
Of the 16 participants, 5 had BME of the metatarsal as shown on MRI (Table 2). During the preseason, the most common affected metatarsal was the first (n = 3), followed by the third (n = 2) and finally the second and fourth metatarsal bones (n = 1 each). Most metatarsal MRI findings were classified as grade 1 (n = 3), followed by grades 2 and 3 (n = 2 each) (Table 3).
Participant Characteristics by Season and Presence of BME a

a Data are reported as mean ± SD or n (%). Bolded P values indicate a statistically significant difference between groups (P ≤ .05). BME, bone marrow edema.
MRI Grades Metatarsal Bone Stress Injury at Preseason and Postseason a

a BME, bone marrow edema; MRI, magnetic resonance imaging; MT, metatarsal.
Table 3 shows the metatarsal locations and MRI grades assigned to abnormalities of the participants. Overall, 5 participants (of 16) showed BME on preseason MRI, and 4 participants (of 13) had changes on postseason MRI (grade improved in 1, worsened in 1, and was stable in 2 participants). Participant 5, with preseason BME of the third metatarsal, developed BME of the first metatarsal head of the other foot. Also, 2 participants without findings on preseason MRI developed BME on postseason MRI. No participant was clinically diagnosed with a metatarsal bone stress injury during the study.
Across variables of interest obtained from the surveys, BME of the metatarsal was more common in players with less exposure to the sport (10.4 ± 4.1 vs 14.2 ± 1.9 years, respectively, from age initiating sport to current age; P = .023). We did not observe differences in other measures including age, nutrition, sleep, or prior bone stress injuries (Table 2).
BME of the Metatarsal on Postseason MRI
All players who completed the season (n = 13) underwent postseason MRI. Overall, 6 participants had BME on postseason MRI, with a similar distribution by metatarsal location (first and third: n = 3; fourth: n = 2). Also, 4 participants with BME of the metatarsal on preseason MRI showed persistent BME on postseason MRI, localized to the first metatarsal and third metatarsal (n = 2 each), followed by the fourth metatarsal (n = 1) and new BME noted at the first metatarsal head of the contralateral foot in 1 participant. The maximum cross-sectional area of BME increased at 2 sites and decreased at 3 sites. The persistence of BME was associated with participants who were older at initial participation in basketball (9.8 ± 4.3 vs 6.2 ± 1.6 years, respectively; P = .050) and had less exposure to the sport (9.6 ± 4.1 vs 14.0 ± 2.1 years, respectively; P = .024) (Table 2).
In 4 participants with findings on postseason MRI, the grade increased in 1 participant (from grade 1 to grade 4) and was stable in the 3 other participants. Additionally, 2 participants without findings on preseason MRI developed grade 2 and 3 MRI findings on postseason MRI.
Metatarsal Bone Stress Injuries During Study Participation
The athletic trainer did not record foot pain of the metatarsals or other bones of the foot and ankle over the course of the study. No participant reported a medically diagnosed metatarsal bone stress injury or any foot injury that received medical attention.
Other MRI Findings
The hallux sesamoids were included in all MRI scans. Preseason MRI identified BME of the sesamoid bones in 8 feet of 6 players; in all cases, the medial sesamoid was affected (Figure 3). A bipartite appearance was noted in 6 of 8 sesamoid bones with BME. Participants with abnormalities of the sesamoid bones trended toward being older (21.0 ± 2.2 vs 19.4 ± 1.3 years, respectively; P = .08). Sesamoid BME observed on preseason MRI persisted on postseason MRI in all cases.

Sagittal short tau inversion recovery (STIR) magnetic resonance imaging of the first metatarsal showing bone marrow edema of the sesamoids (arrow).
MRI findings within the field of view but outside of the area of interest were recorded. There were 2 participants who had abnormalities involving the calcaneus. These included an anterior process calcaneal fracture in one case and a calcaneal bone infarct in the other case. Persistent BME with imaging findings of a navicular stress fracture was observed on both preseason and postseason MRI (Figure 4). Finally, a cuboid fracture was observed on postseason MRI that was not present on preseason MRI. This athlete reported developing pain at the conclusion of the basketball season from landing awkwardly on the same foot, which he reported self-treating as a presumed ankle sprain.

(A) Sagittal short tau inversion recovery (STIR) and (B) long-axis T1-weighted magnetic resonance imaging show findings consistent with a stress fracture of the navicular bone with bone marrow edema on the STIR image and a fracture line on the T1-weighted image (arrows).
Discussion
The purpose of this study was to evaluate MRI findings meeting grading criteria for a metatarsal bone stress injury during the preseason and postseason to determine their association with the development of a metatarsal bone stress injury. A total of 5 participants during the preseason (31% of cohort) had evidence of BME of the metatarsal bones. The findings of BME in the metatarsals persisted in all 4 participants who underwent repeat MRI during the postseason. However, the measured cross-sectional areas of BME changed in size, including a reduction in 3 of 5 metatarsals and an increase in 2 of 5 metatarsals. The MRI classification for preseason metatarsal findings was most commonly grade 1 (n = 3), followed by grades 2 and 3 (n = 2 each). Additionally, 4 participants had persistent findings on postseason MRI: the grade increased in 1 participant (from grade 1 to grade 4) and was stable in the other 3 participants. There were new changes to the contralateral foot of the first metatarsal in 1 participant (grade 1). Despite observed BME during both the preseason and postseason, no participants over the course of a competitive collegiate basketball season were diagnosed with a metatarsal bone stress injury. Collectively, our results suggested a high prevalence of BME on MRI during both the preseason and postseason without associated reports of pain or an injury. This may suggest a limited ability of MRI to serve as a surveillance tool in male collegiate basketball players to identify those at a heightened risk for bone stress injuries during a collegiate season.
The high prevalence of asymptomatic MRI findings of metatarsal BME in our study is consistent with reports in other athlete populations. Lazzarini et al 14 were the first to describe MRI findings in the foot and ankle of runners and nonrunning athletes. Abnormalities including BME of the foot and ankle were detected in 16 of 20 runners and in a smaller number of nonrunners. Similar to our study, investigators found BME of the metatarsals along with changes in the calcaneus, cuboid, and navicular bones. None of the study participants reported associated pain with imaging findings. Bergman et al 4 reported BME in 43% of tibias evaluated across 21 asymptomatic distance runners followed up to 5 years, and no runners were observed to develop an injury localized to the site of the initial imaging abnormality. Our findings are similar to these reports in detecting a high prevalence of BME. While we cannot determine the etiology of these findings, it is important to note that no basketball player reported pain of the metatarsal bones. While some metatarsal BME may have represented an impending bone stress injury, it is also possible that a portion of those with BME may represent adaptive remodeling.
A strength of the current study was the serial acquisition of MRI scans both during the preseason and after the completion of a competitive basketball season. BME of the metatarsals persisted in all 4 athletes who underwent both preseason and postseason MRI. To our knowledge, only 1 other investigation has evaluated BME on serial MRI. Hadid et al 9 reported that among 26 military recruits with BME of the tibia at baseline, a resolution of BME was observed on MRI in 8 athletes at 4 months’ follow-up. Notably, 6 recruits developed a symptomatic bone stress injury of the tibia during military training. 9 There are multiple possible explanations for the absence of symptomatic metatarsal bone stress injuries in our cohort. The presence of BME on preseason MRI and persistent findings on postseason MRI of the metatarsals were observed in basketball players who had less exposure to the sport. It is possible that BME represents bone remodeling and adaptations to sports participation. 18 The duration of the basketball season (no extended play in tournaments after the conclusion of the regular season) for the team studied may also explain why metatarsal BME did not progress to a symptomatic bone stress injury. A study following 76 elite infantry recruits through 3 phases of military training over the course of 12 months 7 demonstrated stress fractures of the tibia and femoral shaft were observed most commonly in the early stages of military training. In contrast, metatarsal stress fractures represented 91% of total injuries sustained in the latter half of the observational period. Therefore, it is possible that they develop later in a training cycle for basketball players. It is also possible that these athletes did not report the pain they were experiencing to medical professionals. Regardless of the explanation for these findings, the presence of BME of the metatarsals should be interpreted with caution.
We observed that a large proportion of participants had abnormalities of the hallux sesamoid bones and in other bones including the navicular, cuboid, and calcaneus. Abnormal findings of the sesamoid bones were observed in 6 of 16 participants on preseason MRI and persisted in all participants who underwent MRI at both time points. These participants trended toward being older than those without changes of the sesamoid bones on MRI. These findings may suggest that sesamoid changes reflect cumulative trauma from the high demands of the forefoot sustained in basketball. The biomechanics of the hallux sesamoid bones is critical to foot function, as the sesamoid complex may transmit loads during push-off exceeding 3 times the body weight. 15 We postulate that the high number of MRI findings involving the sesamoid bones may be explained through the high demands of the forefoot from cumulative time participating in the sport of basketball. Understanding the clinical significance of BME and other imaging findings to the hallux sesamoid bones over a longer period of participation in basketball may clarify the clinical relevance of these findings.
While this is the first report to characterize MRI findings in basketball players over the course of a competitive season, there are study limitations. First is the small sample size and inclusion of participants from only 1 basketball team. Second, participants from the team studied were not competitive in their league and did not compete in the postseason, and this may have limited cumulative athletic exposure to progress to a metatarsal bone stress injury. These factors may limit generalizing findings to other basketball athletes of different ages over longer competitive seasons. Third, we did not perform a physical examination of players at the time of MRI to assess for symptoms of a bone stress injury or conduct surveillance examinations during the season, so we cannot exclude that some BME lesions or imaging findings may have corresponded to symptoms of pain and an injury. The use of an athletic trainer to perform injury surveillance over the course of the season may have reduced the likelihood of missing potential injuries. Fourth, our surveys characterized baseline risk factors for impaired bone health such as sleep and nutrition, and changes during the season in association with MRI findings were not measured. However, the limited number of investigations using serial MRI in athletes, particularly basketball players, provides value in reporting our findings and may serve as a basis for expanding this study design in larger cohorts of athletes over longer study periods to further understand how to best interpret MRI findings in athletes and substantiate the mechanisms of bone remodeling and injuries in metatarsal bones.
Conclusion
Our study showed that collegiate male basketball players had a high prevalence of BME, often without associated symptoms. The high prevalence of asymptomatic MRI findings in the feet of basketball players may be explained by the high biomechanical demands from the sport. However, given that MRI findings were not associated with clinical symptoms, they should be interpreted with caution. MRI remains an important clinical tool for the evaluation of foot pain and can be useful to detect findings corresponding with an injury. However, our results do not support using MRI as a screening or surveillance tool for injuries in collegiate basketball players, although findings could be further substantiated in larger cohorts and with different levels of competitive athletes.
Footnotes
Acknowledgment
The authors are grateful to the participants of the study as well as the coaches, athletic trainers, and others who made this study possible. Investigators are grateful for financial support from the National Basketball Association–General Electric grant.
Final revision submitted July 28, 2021; accepted September 10, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding to support this investigation was received from a National Basketball Association–General Electric grant. M.A.B. has received research support from Novartis Pharmaceuticals (contested by the author). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Massachusetts General Hospital (protocol No. 2017P002633).