
Abstract
Background:
Vitamin D is believed to play a role in influencing fracture risk and athletic performance. Insufficiency of vitamin D affects an estimated three-quarters of the United States population. Hypovitaminosis D has also been demonstrated to be quite common among professional basketball players in the National Basketball Association (NBA).
Purpose:
To determine whether a relationship exists between vitamin D levels and fracture risk and athletic performance (as measured by NBA draft status) among elite basketball players.
Study Design:
Descriptive epidemiology study.
Methods:
Data were obtained from the NBA regarding combine participants from 2009 through 2013. This information included vitamin D level, demographic information, fracture history, and NBA draft status. The data were analyzed to determine associations between vitamin D level and fracture risk and NBA draft status.
Results:
Vitamin D levels were measured for 279 players at the NBA Combine from 2009 through 2013. Vitamin D deficiency (<20 ng/mL) was seen in 32.3% of athletes, vitamin D insufficiency (20-30 ng/mL) was seen in 41.2%, and sufficient levels of vitamin D (>30 ng/mL) were present in only 26.5%. A total of 118 players had a history of at least 1 fracture. Vitamin D level was not predictive of fracture risk. Contrary to our hypothesis, players with a history of stress fracture had a significantly greater mean vitamin D level than those without such history (30.7 vs 25.1 ng/mL; P = .04). A majority (79.6%) of participants were selected in the NBA draft. Players with deficient vitamin D levels had a significantly lower rate of being drafted into the NBA (P = .027). The NBA draft rate was found to increase with increasing levels of vitamin D (P = .007).
Conclusion:
Hypovitaminosis D is quite common among NBA Combine participants, affecting 73.5%. While no significant relationship was found between vitamin D level and fracture history, patients with a history of stress fracture had significantly greater mean vitamin D levels. Additionally, participants with greater vitamin D levels were more likely to be drafted into the NBA. This information supports the potential role of vitamin D in influencing athletic performance.
Vitamin D is a steroid hormone found in the diet and synthesized in the skin in the presence of ultraviolet radiation. 17 The full extent of the physiological effects of vitamin D has yet to be completely elucidated. Vitamin D has proposed roles in bone health, the inflammatory response, immunity, neuromuscular function, carcinoma risk, and overall mortality risk. 1
The role of vitamin D in bone health has been studied extensively, and deficiency may predispose athletes to stress fractures. 8,15 Lappe and colleagues 8 performed a prospective randomized trial evaluating the efficacy of calcium and vitamin D supplementation on stress fracture incidence. Female United States (US) Navy recruits were randomized to receive either calcium and vitamin D supplements or placebo. There were 309 stress fractures over the course of the study, and the recruits who received calcium and vitamin D supplementation had a 20% decreased incidence of stress fracture. 8 Stress fractures occur with some frequency among basketball athletes, most commonly affecting the tibia and metatarsals. 6 McCarthy and others 10 found that a self-reported history of stress fracture was present in 7.3% of athletes participating in the Women’s National Basketball Association (WNBA) Combine.
In addition to mediating bone health and inflammation, vitamin D may also influence neuromuscular function and athletic performance. 1 Vitamin D is believed to directly affect skeletal muscle through a specific vitamin D receptor. Vitamin D has been shown to influence calcium storage in the sarcoplasmic reticulum, phosphate homeostasis, protein synthesis, and the morphologic features of type II muscle fibers. 2,12 Sorensen and colleagues 16 demonstrated an increased percentage and area of type II muscle fibers on muscle biopsies of patients receiving calcium and vitamin D supplementation. Myon and colleagues 11 assessed the influence of vitamin D supplementation on the athletic performance of elite ballet dancers. The authors found an 18.7% increase in isometric quadriceps strength, a 7.1% increase in vertical jump, and a decreased overall incidence of injury in the dancers receiving supplementation.
Insufficiency of vitamin D is surprisingly common, affecting up to 1 billion people worldwide and up to 77% of the US population. 1,12 Certain demographic factors have been associated with vitamin D insufficiency, including dark skin pigmentation, female sex, increasing age, malabsorption syndromes, latitude greater than 35° N, winter season, indoor sports, and the use of sunscreen. 3,13,14,18 Fishman and others 4 recently investigated the epidemic of vitamin D insufficiency among professional basketball players. These authors found that hypovitaminosis D was present in 79.3% of combine participants, with 32.3% having deficient levels.
The clinical significance of hypovitaminosis D in professional basketball players is unknown and requires investigation. It is possible that low levels of vitamin D may be associated with an increased risk of musculoskeletal injury and stress fracture. Insufficient levels of vitamin D may also affect athletic performance on a neuromuscular level. The purpose of this study was to determine the relationship between vitamin D levels and fracture risk and athletic performance (as measured by National Basketball Association [NBA] draft status) among professional basketball players. We hypothesized that players with hypovitaminosis D would have a greater risk of stress fracture and a lower incidence of being drafted into the NBA.
Methods
Approval was gained from our institutional review board as well as the NBA to conduct this study. Vitamin D levels of 279 athletes participating in the 2009-2013 NBA Combine were retrospectively reviewed. Vitamin D levels were collected as part of the general medical evaluation during the NBA Combine. No players were excluded.
All player data were provided to the research team in a deidentified format. Player demographic information was recorded, including age (fractional years), height (inches), weight (pounds), and body mass index. Vitamin D levels (ng/mL) were recorded as well. For our analysis, we used the Endocrine Society’s 2011 guidelines to categorize vitamin D levels. These guidelines define deficient levels of vitamin D as <20 ng/mL and sufficient levels as >30 ng/mL. 5
A retrospective chart review was performed by league representatives to elucidate data regarding fracture history and NBA draft status. The location of fracture was recorded. Additionally, whether or not the fracture was classified as a stress fracture was recorded. In terms of NBA draft status, players were listed as a first-round selection, a second-round selection, or an undrafted player.
Statistical Analysis
Data were analyzed by use of SAS version 9.2 software (SAS Institute). For categorical variables, the Fisher exact test was used to assess group differences. For numerical variables, the paired t test or Wilcoxon rank tests were used. Regression analysis was used to assess predictors of deficiency.
Results
There were 279 players with recorded vitamin D levels who participated in the NBA Combine from 2009 to 2013. The mean player age was 21.5 years. The mean height and weight were 77.7 inches and 216.4 pounds, respectively, and the mean body mass index was 25.2. None of these demographic parameters demonstrated a significant relationship with vitamin D levels.
Using the 2011 Endocrine Society recommended cutoff values, 5 we found that hypovitaminosis D was present in 73.5% of players. Deficient vitamin D levels were present in 32.3% of players, and insufficient vitamin D levels were present in 41.2% of players. Only 26.5% of players had sufficient levels of vitamin D.
Of the 279 players, 118 (42.3%) had a history of fracture. A total of 140 fractures were noted. The most common locations of fracture were hand (n = 33), wrist (n = 31), and metatarsal (n = 19). When assessing for a relationship between vitamin D level and fracture history, we found that the rate of fracture was similar across groups (Fisher exact test, P = .84). History of fracture was present in 40% of players with deficient levels of vitamin D, 42.6% of players with insufficient levels, and 45.6% of players with sufficient levels. No evidence was found of a trend toward decreasing fracture rate with increasing vitamin D level (Cochran-Armitage trend test, P = .55). Regression analysis demonstrated that vitamin D level was not predictive of fracture risk.
A history of multiple fractures was present in 18 patients (6.5%); 8.9% of players with deficient levels of vitamin D, 4.3% of players with insufficient levels, and 6.8% of players with sufficient levels had a history of multiple fractures. The mean vitamin D level was not significantly different in patients with and without a history of multiple fractures (Wilcoxon rank sum test, P = .55). There was no evidence that the rate of multiple fractures differed across vitamin D levels (Fisher exact test, P = .39).
Stress fractures accounted for 23 of the 118 total fractures (19.5%). The most common locations for stress fracture were the tibia (n = 6), foot (n = 5), and ankle (n = 4). The mean vitamin D level in patients with a history of stress fracture was 30.7 ng/mL. This value was higher than the mean level for patients with no history of fracture (25.3 ng/mL) and a history of a non–stress-type fracture (24.9 ng/mL). Graphic representation of this finding is portrayed in Figure 1. The cohort of patients with a history of stress fracture had a significantly greater vitamin D level than those without a history of stress fracture (analysis of variance, P = .04).

Percentage of players with a history of fracture at each vitamin D level.
Of the 279 players in this study, 222 were drafted in either the first or second round (79.6%); 45.5% of players were first-round selections, 34.1% of players were second-round selections, and only 20.4% were undrafted. When assessing the relationship between NBA draft status and vitamin D levels, we found a lower rate of NBA draft occurrence in players with deficient vitamin D levels (Fisher exact test, P = .027). Results showed that 70% of players with deficient vitamin D levels, 83.5% of players with insufficient vitamin D levels, and 85.1% of players with sufficient vitamin D levels were drafted in the first or second round. Graphic representation of this is portrayed in Figure 2. Cochran-Armitage trend testing demonstrated an increasing rate of NBA draft occurrence with increasing vitamin D levels (P = .007).
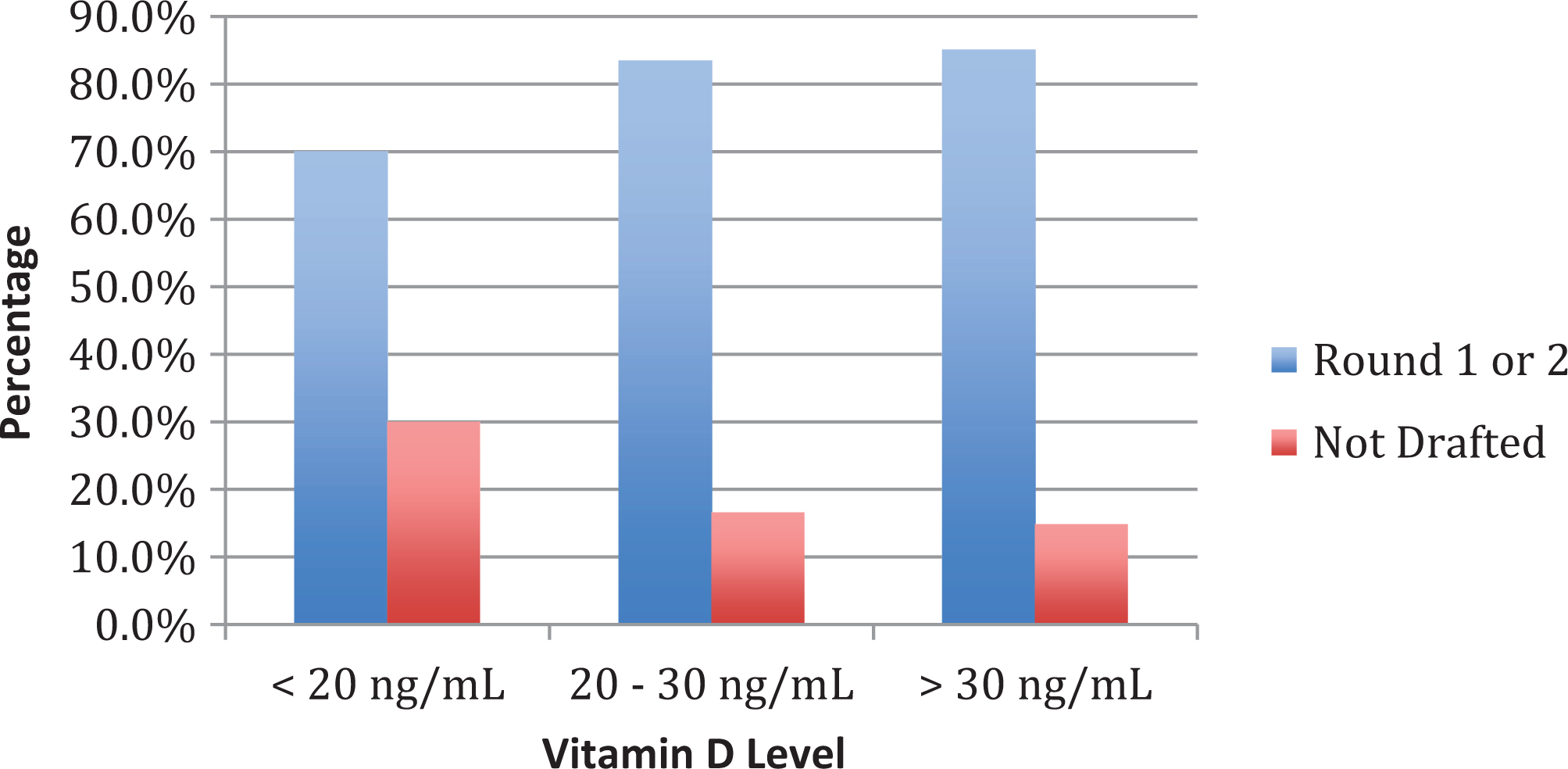
Percentage of players drafted into the NBA (first or second round) at each vitamin D level.
Discussion
Hypovitaminosis D is very common among professional basketball players at the NBA Combine, affecting 73.5% of players in this study. Nearly one-third of the players in our study were found to have deficient levels of vitamin D. Our results were in line with those of Maroon and colleagues, 9 who studied vitamin D insufficiency among professional athletes in the National Football League (NFL). In their cohort of NFL athletes, 68.8% of players had hypovitaminosis D and 26.3% were vitamin D deficient. 9 Those authors used a different scale to categorize vitamin D levels, with less than 20 ng/mL being considered deficient, 20 to 32 ng/mL considered insufficient, and greater than 32 ng/mL considered adequate. 9
Dark skin pigmentation is a known risk factor for vitamin D insufficiency. The increased melanin found in the skin of darkly pigmented individuals may increase the amount of time to synthesize vitamin D up to 10-fold. 3 In the NFL study by Maroon and colleagues, 9 black players had significantly lower mean vitamin D levels than white players. In fact, all players in that study with deficient vitamin D levels were black. 9 Dark skin pigmentation would be considered a significant risk factor among professional basketball players, as up to 76.7% of players in the NBA identify themselves as a person of color. 7
Contrary to our hypothesis, no significant correlation was found between hypovitaminosis D and a history of fracture in our cohort. This held true for individuals with a history of multiple fractures as well. This finding is not what we had expected based on our understanding of the effects of vitamin D on bone health. Maroon and colleagues 9 found in their cohort of NFL players that low vitamin D levels were a significant risk factor for fractures when controlling for the number of years played.
The incidence of stress fracture in the present study was in line with the results of the investigation of WNBA athletes by McCarthy and colleagues. 10 Stress fracture history was present in 8.2% of NBA Combine participants in our study compared with 7.3% of WNBA Combine participants in the McCarthy study. Although vitamin D levels did not correlate with fracture history, a significant relationship was found between vitamin D levels and stress fracture history. However, contrary to our expectations, we found a significant association between increased vitamin D levels and a history of stress fracture. The reason for this finding is uncertain, and the nature of our study limits our ability to control for all of the potential influencing variables. It is possible that athletes with a history of stress fracture received vitamin D supplementation after their injury. This intervention could potentially increase the vitamin D levels measured at the NBA Combine. Due to the blinded cross-sectional nature of this study, we were not privy to whether the players had received vitamin D supplementation. Another explanation of the increased vitamin D levels seen in players with a history of stress fracture relates to athletic exposure. Athletes with superior performance may be more likely to see increased playing time. Greater playing time could increase the exposure of an athlete to activities that may result in stress fracture. However, due to the blinded nature of this study, we did not have access to the amount of playing time seen by these athletes.
The effect of vitamin D on athletic performance has been a subject of research since the 1930s. Vitamin D is believed to enhance neuromuscular function at the skeletal muscle level. 1,2,12 Our study used NBA draft status as a surrogate measure of athletic performance for NBA Combine participants. A significant association was found between increasing levels of vitamin D and being drafted into the NBA. The combine participants drafted into the NBA would be expected to be superior in terms of their health and athleticism. Our findings support the notion of the importance of vitamin D in influencing athletic performance. However, we must emphasize that this is a statistical relationship and not a causal relationship.
This study has several limitations. The first is the retrospective nature of the investigation. We were limited to assessing for a history of fracture rather than prospectively assessing the incidence of fracture occurrence. The second limitation of this study is the inherent uncertainty regarding optimal testing of vitamin D levels and the definition of sufficient levels of vitamin D. For our study, we chose 30 ng/mL to represent a sufficient vitamin D level based on the Endocrine Society’s 2011 guidelines. 5 This threshold is likely conservative, given that vitamin D is not stored in muscle or fat until levels approach 40 to 50 ng/mL. 3 The measurements of vitamin D levels in this study took place at the NBA Combine, which occurs in May. Vitamin D levels have seasonal variation, so it would be interesting to see what the vitamin D levels are during the winter NBA season. A third limitation of this study is that we did not have access to information regarding prior vitamin D supplementation or the amount of playing time exposure. This information would be useful in trying to determine why vitamin D levels were higher in patients with a history of stress fracture.
In the future, it would be interesting to follow this cohort of players prospectively to assess the incidence of injury and athletic performance. Different metrics such as minutes played, scoring, rebounding, and player efficiency rating could be used as alternative measures of athletic performance. It would also be meaningful to assess the utility of vitamin D supplementation in this population given the high prevalence of hypovitaminosis D. Knowledge regarding the utility of vitamin D supplementation in injury prevention and athletic performance would truly highlight the importance of such intervention.
Conclusion
Hypovitaminosis D was very common among NBA Combine participants, with only 26.5% having sufficient levels of vitamin D. Contrary to what we had expected, the mean vitamin D level was significantly higher in patients with a history of stress fracture. The explanation of this finding is uncertain, but it could be attributable to supplementation after injury or increased athletic exposure associated with increased playing time. A significant relationship was found between increasing vitamin D levels and NBA draft occurrence. This highlights the potential role of vitamin D in influencing neuromuscular function and athletic performance. Knowledge of the implications of vitamin D insufficiency in professional basketball players is critically important and can underscore the importance of supplementation in this population of elite athletes.
Footnotes
Acknowledgment
The authors acknowledge James Mirocha, MS, senior statistician, Cedars-Sinai Medical Center.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was waived by Cedars-Sinai Office of Research Compliance and Quality Improvement.