
Abstract
Background:
A better understanding of movement biomechanics after anterior cruciate ligament reconstruction (ACLR) could inform injury prevention, knee injury rehabilitation, and osteoarthritis prevention strategies.
Purpose:
To investigate differences in vertical drop jump (VDJ) biomechanics between patients with a 3- to 10-year history of youth sport–related ACLR and uninjured peers of a similar age, sex, and sport.
Study Design:
Cross-sectional study. Level of evidence III.
Methods:
Lower limb kinematics and bilateral ground-reaction forces (GRFs) were recorded for participants performing 10 VDJs. Joint angles and GRF data were analyzed, and statistical analysis was performed using 2 multivariate models. Dependent variables included sagittal (ankle, knee, and hip) and coronal (knee and hip) angles at initial contact and maximum knee flexion, the rate of change of coronal knee angles (35%-90% of the support phase; ie, slopes of linear regression lines), and vertical and mediolateral GRFs (normalized to body weight [BW]). Fixed effects included group, sex, and time since injury. Participant clusters, defined by sex and sport, were considered as random effects.
Results:
Participants included 48 patients with a history of ACLR and 48 uninjured age-, sex-, and sport-matched controls (median age, 22 years [range, 18-26 years]; 67% female). Patients with ACLR demonstrated steeper negative coronal knee angle slopes (β = –0.04 deg/% [95% CI, –0.07 to –0.00 deg/%]; P = .025). A longer time since injury was associated with reduced knee flexion (β = –0.2° [95% CI, –0.3° to –0.0°]; P = .014) and hip flexion (β = –0.1° [95% CI, –0.2° to –0.0°]; P = .018). Regardless of ACLR history, women displayed greater knee valgus at initial contact (β = 2.1° [95% CI, 0.4° to 3.8°]; P = .017), greater coronal knee angle slopes (β = 0.05 deg/% [95% CI, 0.02 to 0.09 deg/%]; P = .004), and larger vertical GRFs (landing: β = –0.34 BW [95% CI, –0.61 to –0.07 BW]; P = .014) (pushoff: β = –0.20 BW [95% CI, –0.32 to –0.08 BW]; P = .001).
Conclusion:
Women and patients with a 3- to 10-year history of ACLR demonstrated VDJ biomechanics that may be associated with knee motion control challenges.
Clinical Relevance:
It is important to consider knee motion control during activities such as VDJs when developing injury prevention and rehabilitation interventions aimed at improving joint health after youth sport–related ACLR.
The knee is the most commonly injured joint in youth sports. 14,18,32,53 Knee joint injuries, particularly anterior cruciate ligament (ACL) tears, meniscal tears, and intra-articular fractures, are associated with a 6-fold increased risk of future knee osteoarthritis (OA) in the first 11 years. 54 The risk of ACL tears in sports varies by sport and sex, 19 and the overall prevalence of ACL tears in children and adolescents in the United States has increased by approximately 2.3% annually over the past 20 years. 4 ACL tears are associated with a substantial recovery time, 36 time lost from sport, 25 and a high recurrence rate and subsequent contralateral ACL tears. 49,50 Specifically, Schilaty et al 50 reported that 13.8% of patients diagnosed with an ACL tear experienced a second ACL tear. Second ACL tears occurred, on average, 3.7 to 4.7 years after the initial injury and were either caused by graft failure (46.1%) or a tear of the contralateral ACL (53.9%, including contralateral graft tears).
Previous research has determined a number of possible intrinsic factors for ACL tears during sport including age, sex, and previous injuries 12 ; strength 48 ; and joint biomechanics. 3,15,21,35 Biomechanical factors that have been associated with an increased likelihood of ACL injuries in female youth athletes include a stiff landing strategy, 10,29,30 characterized by less total hip and knee flexion as well as valgus knee alignment 39 and medial knee displacement. 27 However, studies assessing movement biomechanics and sport-related ACL tears have not resulted in consistent observations. Hewett et al 22 identified greater knee valgus angles at initial contact and greater vertical ground-reaction forces (GRFs) during a vertical drop jump (VDJ) in women who went on to have an ACL tear. Other studies have reported associations of a lower extremity injury and ACL tear with medial knee displacement during jumping 27,38 and squatting tasks 44 as well as greater knee extension and higher peak vertical GRFs during a jumping task. 30 Importantly, a systematic review by Chia et al 5 indicated that there is currently only limited evidence of strength deficits and movement biomechanics as potential risk factors for an athletic knee injury.
In addition to the apparent uncertainty regarding the contributions of biomechanical factors to an athletic knee injury, there continues to be a knowledge gap on the biomechanical consequences of youth sport–related ACL tears. Systematic reviews by Johnston et al 24 and Pairot-de-Fontenay et al 41 indicated that ACL reconstruction (ACLR) may be associated with greater knee extension during jump-landing and running activities. The authors argue that such differences in knee joint biomechanics may have implications on the risk of future injuries as well as the risk of OA development. However, most of the research evidence on ACLR relates to patients who underwent ACLR as adults, with data typically collected within 2 years after surgery. It is unclear if similar biomechanical alterations may be observed after longer time intervals since surgery. Further, it is unclear if patients who underwent ACLR in their youth display equivalent biomechanical alterations, as youths may differ from adults in their capacity to gain strength. 20,45 Consequently, it is suggested that postoperative rehabilitation for youths should emphasize neuromuscular training, 58 which may affect subsequent biomechanical responses. Therefore, there is a need to quantify the medium-term biomechanical consequences of youth sport–related ACLR to inform rehabilitation and injury/OA prevention strategies targeted at improving knee joint health.
The objective of this research was to examine the differences in VDJ biomechanics between patients with a 3- to 10-year history of youth sport–related ACLR compared with uninjured participants of a similar age, sex, and sport. The specific focus of this study was on the support phase of the VDJ and biomechanical differences at the hip, knee, and ankle joints. In addition to traditional biomechanical variables associated with a risk of sustaining a knee injury, the rate of change of knee varus/valgus alignment was explored as a surrogate measure of dynamic knee motion control.
Methods
Study Design
This is a cross-sectional study of data from the first follow-up of the Alberta Youth Prevention of Early Osteoarthritis (PrE-OA) study, which examined the biomechanical, structural, clinical, physiological, behavioral, and functional consequences of sport-related intra-articular knee joint injuries in youth sports. 56 Approval for this study was provided by the local ethics board, and written informed consent was provided by all participants.
Participants
The PrE-OA cohort consisted of a convenience sample of patients who sustained a knee injury related to youth sports (aged ≤18 years) 3 to 10 years previously and uninjured controls matched on age (within 12 months), sex, and sport at the time of injury. Information on cohort recruitment, including injury diagnoses and exclusion criteria, has been reported previously. 56 Briefly, patients sustained a youth sport–related knee injury (clinical diagnosis of a ligament, meniscal, or other intra-articular tibiofemoral or patellofemoral injury) that required medical attention (eg, by a physician or physical therapist) and disrupted sport participation 3 to 10 years previously. Uninjured controls reported no previous knee injury resulting in time lost from sport. Participants were excluded if they were pregnant, received nonsteroidal anti-inflammatory drugs or cortisone injections within 3 months before testing, had a musculoskeletal injury within 3 months before testing that resulted in time loss (ie, at work, school, or sport), had a diagnosis of other arthritides, or had any current medical problems that prevented participation in functional tests. The current study is a subsample of patients with a history of complete ACL tears and ACLR and uninjured matched controls with available VDJ biomechanical data.
Vertical Drop Jump
Participants performed a series of 10 VDJs in the laboratory in which a larger number of trials, compared with previous studies, 22,27 was chosen to provide a precise estimate of VDJ biomechanics. The VDJ is a dynamic task that resembles sport-specific movements 17,40 and enables insights into the mechanisms of the lower limb and differences due to knee joint injuries. 7,11,40 VDJ biomechanics including knee abduction angle, knee abduction moment, and GRF has been shown to be associated with ACL injuries (r 2 = 0.88) and has a high test-retest reliability (intraclass correlation coefficient >0.94). 22,37 Bilateral joint kinematics and GRFs were recorded using an 8-camera optical marker system (240 Hz; Motion Analysis) and 2 force plates (2400 Hz; Type 9287 [Kistler]). A total of 38 reflective spherical markers (3 noncollinear markers per segment, 4 pelvis markers, and medial/lateral ankle and knee joint marker pairs) were attached to the lower limbs, pelvis, and torso of participants following recommendations by the International Society of Biomechanics. 57
After a standing neutral trial, participants performed the VDJs barefoot from a 31 cm–high box. Participants started with their feet at shoulder width apart and then stepped off the bench, landed with one foot on each force plate, and immediately moved into a maximal countermovement jump. Trials were repeated if participants jumped off the bench instead of stepping off and if both feet did not land on the force plates on either the first support phase or second support phase after the countermovement jump. Participants performed the VDJs barefoot to limit the potential influence of different footwear on joint angle estimates.
Data Processing
Bilateral lower limb kinematics was processed using Cortex (Motion Analysis), and 3-dimensional hip, knee, and ankle joint angles were computed using Visual3D (C-Motion). Cardan angles were computed using an x-y-z order of axis rotation (ie, flexion/extension, adduction/abduction, and internal/external rotation). Right and left leg joint angles were expressed such that positive angles indicated ankle dorsiflexion, knee flexion, adduction (ie, knee varus), and internal rotation as well as hip flexion, adduction, and internal rotation. Joint angle time series were normalized to the first support phase of the VDJ (100 data points) by extracting foot contact events for the right and left feet. Foot contact events of the right and left feet were identified in MATLAB (v2016b; MathWorks) 28 using vertical GRF data for each force plate with a cutoff value of 5% of the maximum vertical GRF. The duration of the support phase of the VDJ was determined from the time either leg first contacted the ground (ie, initial contact) until the first time either leg first left the ground (ie, toe-off). The mean of the resultant normalized joint angle time series was calculated across trials for each participant and used as input for subsequent computation of kinematic variables.
Joint kinematic variables included ankle, knee, and hip sagittal-plane (ie, flexion/extension) range of motion (ROM) during the VDJ support phase (ie, initial contact to maximum joint excursion) as well as knee and hip coronal-plane angles (ie, adduction/abduction) at initial contact and maximum knee flexion. These variables are a subset of joint angles representing the initiation and ROM of the VDJ. Knee and hip coronal-plane data were extracted with respect to maximum knee flexion to determine knee and hip alignment differences at the end of the landing phase. Further, to obtain additional insight into the dynamic changes in varus/valgus knee motion, the rate of change of coronal knee angles was explored. Here, the slopes of the linear regression fits, using 35% to 90% of the support phase of the mean coronal knee angles, were computed for each participant. The period of 35% to 90% of the support phase was chosen based on the shape of the mean waveforms of the coronal knee angles (Figure 1) in which data changed from a more adducted knee (ie, 35%) to greater knee abduction (ie, 90%). A linear regression approach was chosen because of the inherent variability of coronal knee joint angle trajectories between participants. The slope of the resultant regression fit (ie, coronal knee angle divided by percentage of the support phase) was then used to quantify whether the knee tended to move into varus (positive slope) or valgus (negative slope) during this period. Kinematic outcomes were analyzed with respect to the index leg, defined as the injured leg of the injured patients and the respective right or left leg of the uninjured controls.

Joint angle time series of the hip, knee, and ankle in the sagittal plane. Means and standard deviations for the support phase of the vertical drop jump (VDJ; initial contact [0%] to toe-off [100%]) are presented for the index leg of uninjured controls (CON; solid line and dark gray shading) and injured patients (INJ; dashed line and light gray shading). Positive angles represent ankle dorsiflexion, hip and knee flexion, and hip and knee adduction.
GRF data were expressed in newtons and filtered in MATLAB using a 200-Hz fourth-order Butterworth filter. Filtered GRF time series data were normalized to the duration of the first support phase of the VDJ. The mean of the resultant GRF time series was calculated across trials for each participant and used as input for subsequent computation of GRF variables. GRF variables included maximum vertical GRF and mediolateral GRF during landing (0%-40%) and pushoff (60%-100%) of the VDJ support phase (Figure 2). Values were normalized to body weight (BW) to obtain GRFs in which 1 BW is equivalent to the weight of the participant. Mediolateral force directions were standardized for both force plates such that positive forces correspond to a medial direction and negative forces correspond to a lateral direction with respect to the participant.

Vertical and mediolateral (M/L) ground reaction forces (GRF) normalized to body weight (BW). Means and standard deviations for the support phase of the vertical drop jump (VDJ; initial contact [0%] to toe-off [100%]) are presented for the index leg of uninjured controls (CON; solid line and dark gray shading) and injured patients (INJ; dashed line and light gray shading). GRF data were extracted with respect to the maximum force values during the landing phase (0%-40%) and push-off phase (60%-100%).
Statistical Analysis
Participants’ characteristics were reported using medians and ranges, mean differences between matched pairs, standard deviations, and n values. Data analysis was conducted using MATLAB and R (v3.5.0; R Core Team) following previously reported approaches. 55 The effects of an ACL tear on kinematic and GRF variables were investigated using 2 separate multivariate models with random effects (ie, modelKIN and modelGRF, respectively) to account for clustering; analyses were conducted using the nlme package 42 in R. 34 A Bonferroni adjustment was applied to account for the false discovery rate associated with the use of 2 multivariate models (α = 0.025). With this approach, joint angle and GRF measurements for each participant were stacked on top of each other to create a single new DATA variable. The identity of each individual DATA value was retained using 0/1 dummy variables for each joint angle or GRF variable. Assumptions for the normality of residuals were visually assessed using Q-Q plots and plots of residuals against the fitted values.
In the multivariate models, injured and control data were considered as dependent multivariate samples. Participant matching was taken into account by clustering participants according to sex and sport. Resultant cluster allocations were then considered as random effects in the multivariate models. The effects of group (injured vs control) as well as the effects of potential confounders (time since injury and sex) were modeled as fixed effects. Time since injury for control participants was the same as for their respective matched case to reflect the equivalent injury-free time period. Multivariate models initially included fixed-effects interactions of group × time and group × sex (model 1). If the interactions were not significant, they were removed, and the analysis was repeated using the reduced multivariate model (model 2). The consequences of model simplification were assessed using likelihood ratio tests (α = 0.05). Multivariate model findings were reported using β coefficients and 95% CIs.
Results
Participant Characteristics
Of the 54 matched pairs in the PrE-OA study, 48 (n = 96 total) were included in these analyses. The participants were 67% female, with a median age of 22 years (range, 18-26 years; mean difference [MD] ± SD, 0.1 ± 0.7 years), median height of 1.70 m (range, 1.52-1.94 m; MD ± SD, 0.01 ± 0.09 m), and median weight of 69.8 kg (range, 51.0-105.5 kg; MD ± SD, 5.8 ± 13.5 kg) (Table 1). Overall, 6 matched pairs were removed from the analyses because of 1 patient with an ACL injury not participating in biomechanical testing, 1 patient with a new injury between recruitment and testing, or incomplete biomechanical data. All patients with an ACL tear underwent surgical reconstruction. ACL tears were sustained during soccer (40%), basketball (19%), ice hockey (10%), volleyball (6%), rugby (6%), track/running (6%), football (4%), and other (2%).
Participant Characteristics a
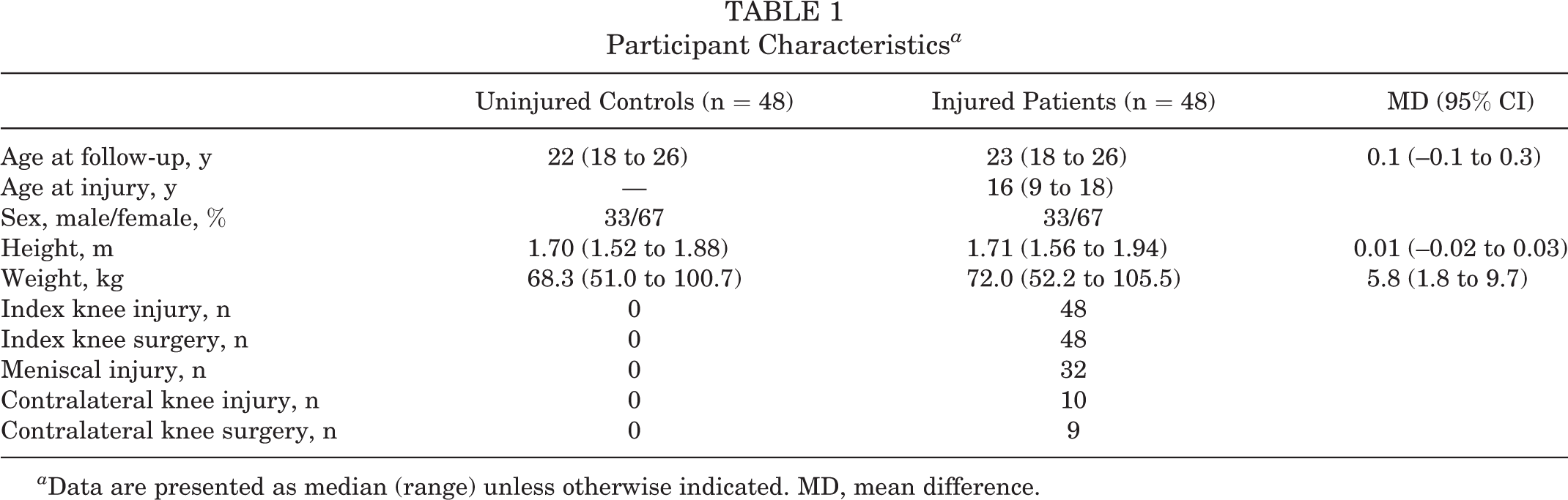
a Data are presented as median (range) unless otherwise indicated. MD, mean difference.
VDJ Biomechanics
Multivariate models including interaction terms (model 1) revealed no significant interactions of group × time and group × sex for joint angle or GRF variables. Therefore, interaction terms were removed from the models. Likelihood ratio tests of kinematic and GRF multivariate models with (ie, model 1KIN and model 1GRF) and without (ie, model 2KIN and model 2GRF) interaction terms indicated no significant effect of model simplification. Model 2KIN indicated a significant effect of group on the slope of knee adduction/abduction angles across 35% to 90% of the VDJ support phase (β = –0.04 deg/% [95% CI, –0.07 to –0.00 deg/%]; P = .025) (Tables 2 and 3 and Figure 1). Therefore, injured patients performed the support phase of the VDJ with a significantly greater change in knee alignment in the direction of knee abduction (ie, knee valgus) than uninjured controls. No significant differences were observed for the remaining ROM or joint angle variables of the hip, knee, and ankle at initial contact or maximum knee flexion (Table 3). Significant effects of sex were observed for knee adduction/abduction at initial contact (β = 2.1° [95% CI, 0.4° to 3.8°]; P = .017) and the slope of knee adduction/abduction (β = 0.05 deg/% [95% CI, 0.02 to 0.09 deg/%]; P = .004) (Table 3). These findings indicate that women performed the VDJ with a more abducted knee (ie, knee valgus) at initial contact and displayed a greater change toward knee valgus during the support phase of the VDJ than men. Significant effects of time since injury were observed for knee (β = –0.2° [95% CI, –0.3° to –0.0°]; P = .014) and hip (β = –0.1° [95% CI, –0.2° to –0.0°]; P = .018) flexion/extension ROM. Therefore, both control and injured participants performed the VDJ with a more extended knee and hip as the duration of time since injury increased. An assessment of the effect of data clusters (random effects) for model 2KIN did not indicate a substantial effect of clustering on the statistical findings.
Model 2GRF did not indicate an effect of group that met the criteria for significant differences (Table 4). However, maximum mediolateral GRF indicated trends for greater maximum medial GRFs by injured patients compared with uninjured controls during the landing phase (β = 0.04 BW [95% CI, 0.00 to 0.08 BW]; P = .043) and push-off phase (β = 0.03 BW [95% CI, 0.00 to 0.07 BW]; P = .049) (Tables 2 and 4 and Figure 2). Significant effects of sex were observed for maximum vertical GRFs during landing (β = –0.34 BW [95% CI, –0.61 to –0.07 BW]; P = .014) and pushoff (β = –0.20 BW [95% CI, –0.32 to –0.08 BW]; P = .001) (Table 4). These findings indicate that women experienced greater BW-normalized vertical forces during landing and pushoff of the VDJ support phase. No significant effects of time since injury were observed for either vertical or mediolateral GRFs. An assessment of the effect of data clusters (random effects) for model 2GRF did not indicate a substantial effect of clustering on the statistical findings.
Joint Angles and GRFs a

a Data are presented as mean ± SD unless otherwise indicated. AA, adduction/abduction; FE, flexion/extension; GRF, ground-reaction force; GRFML, mediolateral ground-reaction force; GRFV, vertical ground-reaction force; IC, initial contact; MD, mean difference; MKF, maximum knee flexion; PD, plantarflexion/dorsiflexion; ROM, range of motion.
b Normalized to body weight.
Multivariate Fixed-Effects Model Outcomes for Kinematic Variables a

a As no significant effects of interactions of group × TSI and group × sex were observed (model 1), the interaction terms were then removed (model 2). AA, adduction/abduction; FE, flexion/extension; IC, initial contact; MKF, maximum knee flexion; PD, plantarflexion/dorsiflexion; ROM, range of motion; TSI, time since injury.
b Statistically significant: P ≤ .025.
c Statistically significant: P < .05.
d Statistically significant: P < .01.
Multivariate Fixed-Effects Model Outcomes for GRF Variables a

a As no significant effects of interactions of group × TSI and group × sex were observed (model 1), the interaction terms were then removed (model 2). GRF, ground-reaction force; GRFML, mediolateral ground-reaction force; GRFV, vertical ground-reaction force; TSI, time since injury.
b Normalized to body weight.
c Statistically significant: P < .025.
d Statistically significant: P < .05.
e Statistically significant: P < .01.
Discussion
This study compared VDJ biomechanics between patients with a 3- to 10-year history of youth sport–related ACL injuries and uninjured peers of a similar age, sex, and sport. The findings of this study indicate that patients with a history of ACLR were more likely to display a larger rate of change of dynamic knee alignment in the direction of knee valgus during the support phase of the VDJ. Similarly, women, regardless of injury status, displayed significantly greater knee valgus at initial contact, a greater rate of change of coronal-plane knee alignment during the support phase, and greater vertical forces during the landing and push-off phases. Time since injury affected both knee and hip joint excursions regardless of injury status. The findings of this study support evidence of challenges in the dynamic control of knee motion during a sport-specific movement task in patients with a previous ACL tear, despite surgical reconstruction.
Cohort Characteristics
In line with previous research, 19 women represented the majority of patients with ACLR (67%). Gornitzky et al 19 demonstrated that female youth athletes experience a 1.6-fold greater rate of ACL tears per athletic exposure than male athletes. Further, injury type has been shown to vary by sport, with Emery 12 and Gornitzky et al 19 showing that the injury risk for female youth athletes is greatest in team sports including soccer and basketball. Similarly, sports associated with the greatest incidence of injuries in this study were soccer (40%), basketball (19%), and ice hockey (10%). Therefore, it appears that the cohort recruited in this study was broadly representative of those recruited in previous research on youth sport–related injuries. Also, ACL tears are commonly associated with a concomitant meniscal injury, 54 which was also evident for participants included in this subsample analysis, with 32 of 48 patients reporting a meniscal injury (Table 1). This observation is relevant in light of research evidence for an increased risk of developing radiographic signs of OA with combined ACL and meniscal injuries. 54
Effect of Injury History
Multivariate results indicated no group differences for sagittal-plane ankle, knee, and hip ROM data as well as coronal-plane knee and hip data at initial contact or maximum knee flexion (Table 3). This is in contrast to previous findings of a stiff landing strategy, characterized by reduced hip or knee flexion angles, 10 by patients either at risk of ACL injuries 30 or with previous ACL tears. 9,24 Further, there was no evidence for greater vertical GRFs (Table 4), which have been suggested as a risk factor for ACL injuries. 22 Injured patients also did not adopt greater hip flexion angles, as reported by Clarke et al, 6 which have been attributed to neuromuscular control deficits. Similarly, while greater knee valgus angles at initial contact have been reported by Delahunt et al 9 and Hewett et al, 22 no differences in coronal-plane knee angles were observed between injured and control participants for this cohort.
Despite the apparent absence of biomechanical differences previously described for similar cohorts, ACLR was associated with a significantly more negative slope of knee adduction/abduction angles from 35% to 90% of the support phase of the VDJ (Tables 2 and 3). After initial contact (0% of the VDJ support phase), as the knee began to flex, the knees of injured and control participants typically moved from a varus to valgus alignment and returned again to a more varus alignment when the knee approached maximum flexion angles (∼35% of the support phase) (Figure 1). Thereafter, as the knee approached maximum knee flexion and began to extend again, the knee adopted a progressively more valgus alignment until approximately 90% of the support phase. Findings of a more negative slope between 35% and 90% of the support phase for injured patients, in turn, indicate a greater rate of change of knee alignment in the direction of knee valgus during the transition from the landing to push-off phases of the VDJ.
Findings of a greater rate of change of knee varus/valgus angles (Table 3) are analogous to previous observations of greater apparent knee valgus. 38,40,44 Specifically, Räisänen et al 44 reported an increased risk of injuries in young athletes with high frontal-plane projection angles of the knee during a single-leg squat. Similarly, Numata et al 38 observed significantly greater dynamic knee valgus for female youth athletes during a single-leg drop jump, who went on to develop an ACL tear, and Ortiz et al 40 observed potentially greater dynamic knee valgus during drop jumps in women with ACLR. In the current study, rather than landing with a more valgus alignment, patients with ACLR appeared to experience a greater rate of change of knee alignment during the transition from landing to pushoff. These findings may be an indication of greater difficulty for patients with ACLR to control coronal-plane knee motions, which has been related to diminished hip muscle strength and neuromuscular control. 43 However, no differences in strength between groups were reported in a previous analysis of participants with and without a knee injury. 56 Further, the adoption of a more valgus knee alignment may help to explain the observation of a tendency for elevated maximum medial GRFs by injured patients (Table 4). We are not aware of previous reports on differences in mediolateral GRFs. However, larger medial GRF trajectories may be a consequence of force application by a more medially positioned or valgus knee, resulting in a greater lateral force application of the foot to the ground. It should be acknowledged that patients with ACLR tended to be approximately 5.8 kg heavier than their uninjured counterparts (Table 1), which could have contributed to the observed differences.
From the perspective of the longitudinal consequences of ACLR, the findings of this study may provide additional insight into potential mechanical pathways for the development of posttraumatic OA. Changes in cartilage contact location and cartilage surface contact kinematics, 2 after ACL transection and ACLR, have been hypothesized to contribute to the pathogenesis of knee OA. Specifically, increased normal stress and plowing friction in ligament-transected animal models have been suggested to relate to greater gross morphological damage. 1,52 Further, greater tibiofemoral contact point excursions and velocities have been observed in patients with ACLR 23 and OA. 16 While an assessment of knee arthrokinematics is outside the scope of this study, a larger rate of change of coronal-plane knee alignment during the VDJ may indicate the presence of a similar mechanical mechanism that could contribute to the onset and progression of posttraumatic OA.
Effect of Sex and Time Since Injury
Similar to previous observations, sex had a significant effect on knee valgus angles in which women exhibited greater valgus angles at initial contact and steeper slopes of coronal-plane knee angles in the direction of increasing valgus (Tables 2 and 3). These findings are in agreement with those for national youth soccer players 33 in which female players had significantly greater knee valgus at multiple points of a drop jump. In alignment with the findings of Romanchuk et al, 47 hip adduction angles tended to be greater for women at maximum knee flexion (Table 3). However, in contrast to the findings of Decker et al, 8 no differences in sagittal-plane knee or ankle ROM between men and women were observed for this cohort. Interestingly, women exhibited significantly larger vertical GRFs relative to their BW than men (Table 4). Schmitz et al 51 reported similarly elevated vertical GRFs for female recreational athletes performing single-leg landings. However, female athletes in the study by Schmitz et al 51 also displayed less hip and knee flexion, which was not observed for the current cohort.
In combination, the current results provide supporting evidence that women were more likely to undergo the support phase of the VDJ with a greater knee valgus alignment than their male counterparts. Findings for sex differences in coronal knee angles, combined with the finding for greater vertical GRFs, may help to explain the 2 to 6 times greater likelihood for female patients to sustain an ACL (re)injury. 46 In addition to the effects of sex, time since injury also had a significant effect on knee and hip flexion/extension ROM angles (Table 3). However, both injured and control participants appeared to exhibit the same change toward greater knee and hip extension with respect to increasing duration of time since injury. The observed effect of time since injury may therefore be more closely related to changes in participant age rather than being a consequence of the injury.
Based on the findings of the study, biomechanical differences were observed to be associated with ACLR status and sex. However, it is unknown whether the biomechanical differences were a result of ACLR or may have been pre-existing. Nevertheless, it may be argued that both patients with ACLR and women, regardless of injury status, may benefit from participation in injury prevention programs. Injury prevention programs have been shown to modify landing biomechanics 31 (perhaps based on improvements in knee motion control during landing) and to reduce the risk of injuries during sport. 13 It is important to acknowledge that, given the chosen experimental design, the extent to which the observed differences in landing biomechanics may be predictive of the future injury risk cannot be addressed in this research, and this question remains a point of investigation. 26
Strengths and Limitations
This study applied a rigorous design and statistical approach to limit the effects of potential confounders (ie, age, sex, and sport) and reduce statistical errors associated with multiple statistical testing. Multivariate analysis of kinematic and GRF data allowed for simultaneous estimation of effects while taking the potential correlation between outcomes into account. This approach limited the possibility of false discovery by performing one model with all kinematic or GRF outcomes considered together instead of performing one model for each outcome separately. It should be recognized that the analyses were cross-sectional, and it is not possible to know if the identified differences preceded or developed after the injury. While injured and control participants were matched on sex, age, and sport, it should also be recognized that youths may not have participated in only one sport and may have been exposed to injury risk factors associated with different sports. Further, differences in sport participation and level of play since the time of injury, as well as associated differences in strength, may have contributed to movement biomechanical differences between groups.
Although injured patients were recruited through previous studies and a sport medicine clinic, the confirmation of no knee injury in control participants relied on their self-reported history. An injury of the contralateral leg, the specific mechanism of the ACL tear, and ACL graft choice may lead to differences in the movement of the contralateral and index legs. Further, involvement of the growth plate in skeletally immature patients with ACLR may lead to leg length imbalances and altered movement biomechanics. However, because of a lack of more detailed injury information and medical records, as well as sample size limitations, additional data stratification could not be conducted. Control participants may have been subject to recall bias regarding all knee injuries; however, it is expected that the recollection of ACL injuries would not be subject to recall bias. Further, a physical therapy assessment was performed to confirm no ACL deficiency. The results of this study reflect a subgroup of the local clinical population only and are not generalizable. It is important to emphasize that these findings are not reflective of an ACL injury mechanism but rather reflect landing strategies that were either pre-existing or were adopted by patients with ACLR.
Conclusion
Patients with a 3- to 10-year history of youth sport–related ACLR and women, regardless of injury status, exhibited biomechanical outcomes commonly associated with a risk for knee joint injuries and continuing challenges in the control of knee motion during a VDJ task compared with matched uninjured controls. While the specific reasons for the difference between injured and uninjured participants (eg, neuromotor control) cannot be discerned directly, these findings provide evidence in support of implementing primary injury prevention strategies (ie, neuromuscular training) to enhance dynamic knee motion control (eg, landing, change of direction) to reduce the injury risk as well as secondary prevention strategies to reduce injury recurrence.
Footnotes
Acknowledgment
The authors acknowledge all research staff, students, and participants involved for their time and support in completing this research project.
Final revision submitted August 20, 2021; accepted August 25, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Canadian Institutes of Health Research (MOP 133597). Further financial support was received from the Alberta Osteoarthritis Team and Alberta Innovates iCORE Strategic Research Chair. The Sport Injury Prevention Research Centre is one of the Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Calgary (No. REB14-2212).