
Abstract
Background:
Differences in postoperative recovery after anterior cruciate ligament reconstruction (ACLR) between men and women have been demonstrated in the adult population. Sex-based differences have been incompletely investigated in adolescents, which represent the subpopulation most affected by ACL injury.
Purpose/Hypothesis:
The purpose of this study was to compare the 6-month postoperative functional recovery after ACLR between adolescent boys and girls. It was hypothesized that significant differences in postoperative strength, dynamic balance, and functional hop test performance would be seen between the sexes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included in this study were athletes aged 12 to 19 years with closed or closing growth plates who underwent ACLR with hamstring autograft between May 2014 and May 2018 at a single institution. All athletes had undergone strength and functional testing between 5 and 8 months postoperatively. Exclusion criteria were previous knee surgery (contralateral or ipsilateral knee), concomitant injury/surgery other than meniscal tear/repair, allograft supplementation, and incomplete medical records. The limb symmetry index (LSI) for strength (measured with handheld dynamometer), as well as dynamic Y-balance and functional hop test performance, was compared between groups. To account for differences in physical characteristics between the sexes, 1-way between-group multivariate analysis of covariance was used to analyze the data.
Results:
Overall, 543 patients (211 boys, 332 girls) were included. There was no significant difference in age, body mass index, incidence of concomitant meniscal pathology, use of regional anesthesia, or time to functional testing between cohorts. Female athletes demonstrated a statistically significantly greater deficit in quadriceps strength LSI compared with male athletes (boys, +3.4%; girls, –2.3%; P = .011). Both male and female athletes demonstrated 33% hamstring strength deficits, with no statistically significant sex-based differences in dynamic balance or functional hop testing.
Conclusion:
Female athletes demonstrated greater quadriceps strength deficits than male athletes at 6 months after ACLR with hamstring autograft. Severe hamstring strength deficits persisted in both male and female patients at this time point. The correlation of such deficits to risk of ACL retear warrants continued study in the adolescent population and may support a delay in return to sports, which has been suggested in the more recent literature.
The incidence of anterior cruciate ligament (ACL) tear peaks in the adolescent and early adult age groups. 28 The annual incidence of isolated ACL tears has been reported to be 68.6 per 100,000 person-years, with more than 98% of adolescent patients progressing to ACL reconstruction (ACLR) within 1 year of injury. 27 After surgical intervention, there is great investment, on the part of both the patient and the sports medicine community, in postoperative rehabilitation and overall functional recovery. Many rehabilitation programs are standardized and universally applied across widely heterogeneous populations in a noncustomized fashion, without consideration of various patient factors that may influence how a particular patient progresses after ACLR. One such factor may be a patient's sex, as differences in postoperative recovery between the sexes could shed light on the need to tailor rehabilitation protocols to achieve the best results and may help guide discussions and set expectations for patients and their families.
The current understanding of sex-based differences in postoperative recovery after ACLR remains understudied and incompletely explored. Several investigations have attempted to address the question of differences in post-ACLR recovery, function, and performance between the sexes but have largely been limited to the adult population. Comparisons have been assessed through physical examination, patient-reported outcomes, and postoperative functional testing. 2,8,9,13,23,26 To date, studies on adult patients have offered conflicting findings; a number of studies have indicated minimal to no difference between men and women, while others have noted clear differences to consider. Such differences have often been reported based on choice of ACL graft. 1,2,5,8 For example, 2 studies investigating patellar tendon autograft reported no difference in postoperative functional testing 2,8 or patient-reported outcomes. 2 However, differences have been detected between male and female patients regarding pain, crepitus, and arthrofibrosis. After ACLR with patellar tendon autograft, women have reported more pain, 1 crepitus, 1 and stiffness 5 compared with their male counterparts. In another series, women were found to attend an average of 6 more visits of physical therapy compared with men. 3
Postoperative differences have also been noted between adult men and women who have received hamstring autograft ACLR. For example, women have demonstrated increased translational laxity, as measured through Lachman tests, and rotational laxity, as measured through pivot-shift testing. 9,13,23,25,26 Some authors have questioned the clinical significance of this increased laxity on functional testing and postoperative outcomes. 17 Studies have noted differences between the sexes during strength and functional testing in adult patients after ACLR with hamstring autograft. One study 16 reported that women have a significantly increased deficit in quadriceps strength compared with men. Men have also been found to perform better on hop testing at 1-, 2-, and 7-year follow-up visits. 26 Additionally, adult men have been reported to ultimately return to preinjury athletics more frequently than their female counterparts, 23 with a higher rate of return to sports at 1 year after surgery. 34
Despite these previous findings in adult patients, we are unaware of comparative analyses for post-ACLR rehabilitation and functional recovery between the sexes in the adolescent population. The hamstring remains the single most commonly used autograft option for this particular characteristic and has risen in popularity over the last decade. 4,6,7,10 The purpose of the current study was therefore to compare the 6-month postoperative functional recovery after ACLR with hamstring autograft between adolescent boys and girls. We hypothesized that a significant difference in strength, dynamic balance, and functional hop test performance would be demonstrated between the sexes approximately 6 months after ACLR.
Methods
This institutional review board–approved study was performed at a single, large, metropolitan tertiary care pediatric hospital. Inclusion criteria were adolescent athletes aged 12 to 19 years with closed or closing growth plates as determined on radiographs and magnetic resonance imaging who underwent primary ACLR with hamstring autograft between May 2014 and May 2018, and who subsequently completed strength and functional testing at the affiliated institutional injury prevention center between 5 and 8 months postoperatively. The patients tested at this center are representative of the patient population that we treat at large, as most patients returning for 6-month postoperative visits complete testing at the site, regardless of where they are attending physical therapy. Exclusion criteria were open growth plates or age outside of adolescence (≥20 years), functional testing performed <5 or >8 months postoperatively, revision ACLR, use of allograft for ACLR, early post-ACLR surgery that might confound testing performance (such as lysis of adhesions and manipulation under anesthesia for postoperative arthrofibrosis), concomitant ligament or cartilage surgery that might confound normal postoperative recovery (eg, collateral ligament reconstruction or microfracture), use of all-epiphyseal or nonconventional/nonanatomic tunnel placement or position, and incomplete medical records. The patient selection process is illustrated in Figure 1.

Flowchart detailing the number of screened patients and the criteria for determining the final cohort. ACL, anterior cruciate ligament; LOA, lysis of adhesions; MCL, medial collateral ligament; MUA, manipulation under anesthesia; PCL, posterior cruciate ligament.
The patients’ medical records and imaging were reviewed for characteristic data, which included age at time of surgery and postoperative functional testing, sex, body mass index (BMI), and growth plate status at time of surgery. Data were additionally collected regarding laterality of ACL injury, concomitant injury within the knee, time from ACLR to functional testing, and use of perioperative regional anesthesia via nerve block.
The primary outcomes of interest were the results of postoperative functional testing, which was performed at an institutional injury prevention center by 1 of 3 different certified athletic trainers and kinesiologists with master’s degrees and additional strength and conditioning certification. Previous studies 31,32 have demonstrated substantial interrater reliability for such testing at this center. The functional tests included strength, dynamic balance, and hop testing. Each test was performed twice on the injured limb, and the results were averaged. Each test was then performed on the contralateral, or uninjured, limb, and those results were averaged. We then determined the limb symmetry index (LSI), in which the ratio of the injured to uninjured limb is reported as a percentage. To simplify the reporting, 100% was then subtracted from the calculated LSI 31 ; a resulting positive (+) value indicated a surplus of the operative limb compared with the uninjured limb, and a resulting negative (−) value indicated a deficit compared with the contralateral limb. For example, an LSI of 104% is reported as +4% while 96% is reported as −4%.
The isometric strength of individual muscle groups was performed using a handheld dynamometer (Hoggan Scientific). This technique is used at our institution with excellent interrater and intrarater reliability. 31 The muscle groups we tested included the quadriceps, hamstrings, hip abductors, and hip extensors. To test the quadriceps, the participant was seated at the edge of the examination table with the knee at 90° of flexion. The arms were crossed over the chest, and he or she extended the knee with the dynamometer held at the anterior tibia just proximal to the ankle joint. To test the hamstrings, the participant was positioned prone on the examination table, the knee and hip were flexed to 90°, and he or she attempted to flex the knee further with the dynamometer placed posteriorly at the distal tibia. Hip abduction strength was measured with the participant on his or her side and the study limb facing up, with the dynamometer at the lateral malleolus. Hip extension was measured with the participant positioned supine, knee flexed to 90°, and the dynamometer placed at the middle third of the posterior thigh. 31
Dynamic balance was quantified using a commercially available Y-balance assessment system (Functional Movement Systems) as previously described. 21,31 The participant stood on a platform in the center of the equipment and subsequently slid a plastic piece along a track in the anterior, posteromedial, and posterolateral directions. The maximum reach distance was measured in centimeters, and the average value was used in the analysis.
Functional hop testing included single hop for distance, single-leg triple hop for distance, 6-m timed single-leg hop, and crossover single-leg hop. 24,31 In the single-leg hop, participants hopped using the tested limb and were asked to maintain balance upon landing. Triple hop was similar, where the participant hopped forward 3 times on the tested limb, maintaining balance with each individual hop for several seconds. In the crossover hop, the participant hopped 3 times over a piece of tape placed in the middle of their path. The sequence of hops was medial, lateral, and then medial again. Each of these 3 hop tests was measured in total distance in meters. The final hop test was timed and measured in seconds. Participants hopped a total of 6 m, as many times as was necessary to cover the distance in the shortest amount of time.
Statistical Analysis
Analyzed dependent variables included muscular strength, dynamic balance, and functional hop. To identify asymmetry in these 3 variables, we determined the deficit as a percentage, which was calculated through the LSI. The independent variable was patient sex. Given the presence of normal distributions in the continuous variables analyzed, including LSI, independent t tests were used when applicable. Differences in patient characteristics were assessed, including characteristics (age, height, weight, and BMI) and duration from ACLR to the functional testing. Chi-square tests were used to compare the status of meniscal tears and usage of regional anesthesia by sex. If any differences were detected by independent t test and chi-square tests, that particular variable was treated as a covariate. To account for those differences (detected covariates) by sex at baseline, 1-way between-group multivariate analysis of covariance (MANCOVA) was used to compare the effects of sex on muscular strength, dynamic balance, and functional hop.
Results
A total of 543 adolescent patients met the inclusion criteria for analysis. There were 211 boys (38.9%) and 332 girls (61.1%), with a mean age of 16.1 years (range, 13-19 years for boys vs 12-19 years for girls). Overall, boys and girls shared similar characteristic information (Table 1). While male patients had a greater mean height and weight, there was no significant difference in mean BMI (P = .427). Patient height and weight were treated as covariates and entered in the MANCOVA model. There was no significant difference between the sex-based cohorts in the mean time from surgery to functional testing (P = .402), in the use of perioperative regional anesthesia blocks (P = .19), or in the presence of meniscal tear (P = .055) (Table 1).
Patient, Injury, and Surgery Data a
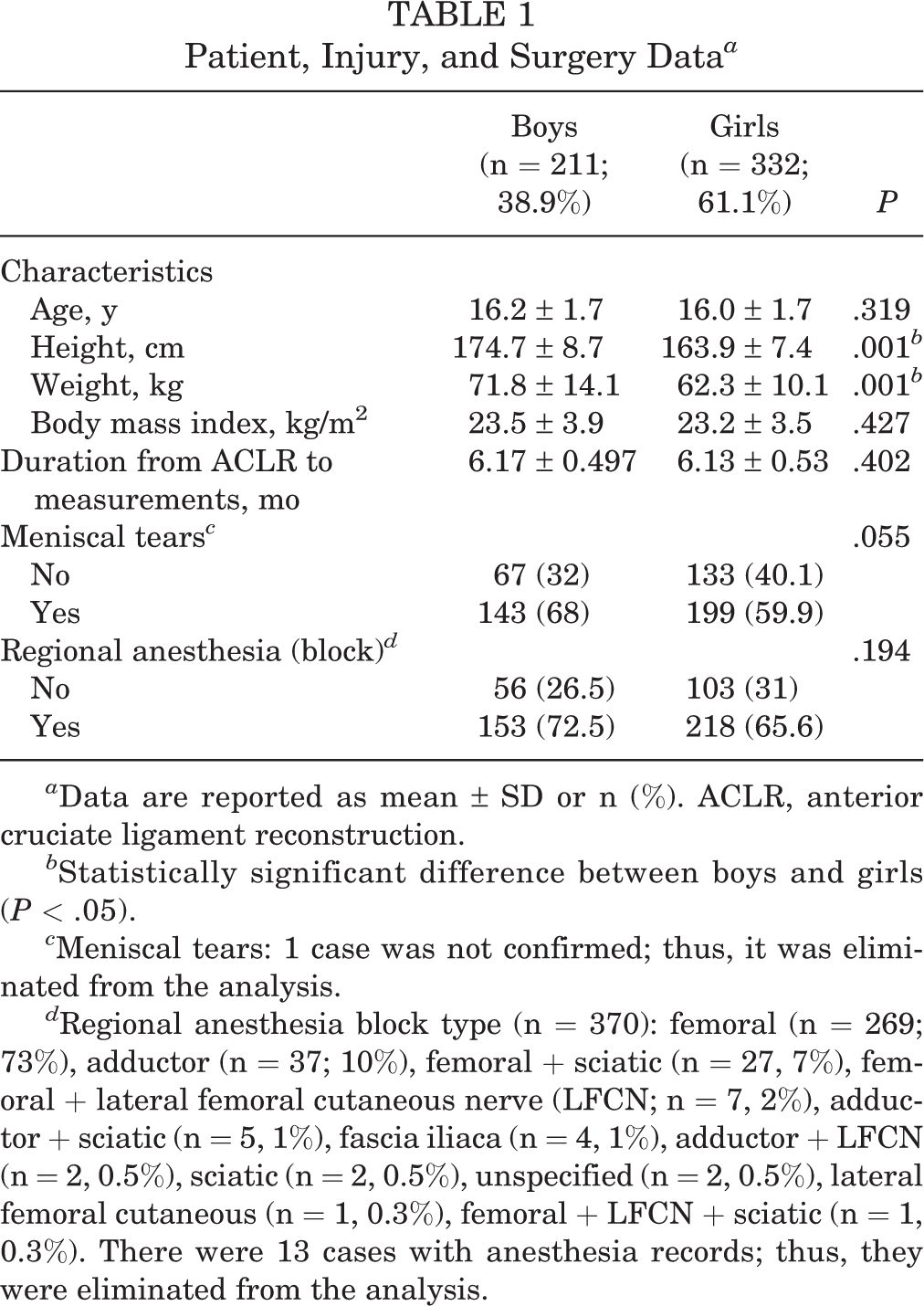
a Data are reported as mean ± SD or n (%). ACLR, anterior cruciate ligament reconstruction.
b Statistically significant difference between boys and girls (P < .05).
c Meniscal tears: 1 case was not confirmed; thus, it was eliminated from the analysis.
d Regional anesthesia block type (n = 370): femoral (n = 269; 73%), adductor (n = 37; 10%), femoral + sciatic (n = 27, 7%), femoral + lateral femoral cutaneous nerve (LFCN; n = 7, 2%), adductor + sciatic (n = 5, 1%), fascia iliaca (n = 4, 1%), adductor + LFCN (n = 2, 0.5%), sciatic (n = 2, 0.5%), unspecified (n = 2, 0.5%), lateral femoral cutaneous (n = 1, 0.3%), femoral + LFCN + sciatic (n = 1, 0.3%). There were 13 cases with anesthesia records; thus, they were eliminated from the analysis.
At the time of functional testing (Table 2), girls demonstrated a quadriceps strength LSI deficit, while boys showed a strength surplus (boys, +3.4%; girls, –2.3%; P = .011). There was no difference in the strength parameters between male and female athletes for the other muscle groups. Hamstrings demonstrated a strength deficit in both sexes (boys, –33.0%; girls, –33.2%; P = .943), while hip abductors (boys, +3.8%, girls, +6.2%; P = .490) and hip extensors (boys, +4.2%, girls, +2.2%; P = .637) demonstrated small strength surpluses in the operative limb in both sexes.
No statistically significant difference was seen between boys and girls regarding deficits in dynamic balance, all of which were less than 1% in either balance score deficit or surplus (Table 2), including composite score. No statistically significant side-by-side difference was noted between boys and girls with regard to functional hop testing. Female patients demonstrated a greater deficit in single hop compared with boys (boys, –4.0%; girls, –8.1%; P = .062), but the difference was not statistically significant.
Strength, Balance, and Functional Hop Testing Deficits in Quadriceps, Hamstrings, Hip Abductors, and Hip Extensors a

a Data are reported as mean ± SD (95% CI). ACLR, anterior cruciate ligament reconstruction; LSI, limb symmetry index.
b Statistically significant difference between boys and girls (P < .05).
Discussion
In assessing the performance of a large number of adolescent athletes in an expansive array of strength, balance, and functional hop testing parameters approximately 6 months after ACLR with hamstring autograft, the current study elucidated a statistically significant difference in quadriceps strength recovery between boys and girls. While a relatively small mean female deficit in quadriceps strength was detected (–2.3%, by LSI) and was not so clinically significant that it would denote a failed test, it was statistically different from that of boys, who demonstrated a mean strength surplus (+3.4%) in their operative lower extremity. The difference in quadriceps strength between the sexes is greater than 5%, which given the large number of patients included, places it outside the realm of user error and therefore warrants discussion.
Previous authors have demonstrated differences in quadriceps strength between the sexes after ACLR in adults. Huston and Wojtys 15 suggested that deficits in quadriceps strength might be more clinically significant in female athletes, because female athletes recruited their quadriceps to stabilize an anteriorly translating knee more than their male or nonathlete female counterparts. At 1 year after ACLR with hamstring autograft, Kim and Park 16 reported that adult women had a greater quadriceps strength deficit in LSI compared with men at both 60 deg/s (men, 15.8%; women, 22.9%; P = .019) and 180 deg/s (men, 13.5%; women, 19.7%; P = .007) using an isokinetic dynamometer. Snyder-Mackler and Di Stasi 30 compared male and female patients with an average age of 19 years at 6 months from ACLR surgery and also found that female patients demonstrated greater quadriceps weakness (male patients, +1.9%; female patients, –12.74%; P = .017). Additionally, they reported that male patients were more likely to be cleared for return to sports compared with their female counterparts. They concluded from their preliminary data that female patients may have a differential response to physical therapy after ACLR.
Interestingly, in the current study, no statistically significant difference was found in hop test performance between the sexes, and despite boys demonstrating greater quadriceps strength on their operative side, mean deficits were seen in LSI values for all 4 hop tests in boys. Notably, girls did have a greater deficit (–8.1%) in the single-hop test than boys (–4.0%) to a degree (P = .062) that may suggest a trend toward statistical significance. Previous literature is somewhat conflicting regarding the association between lower extremity muscle strength and performance on hop testing. For example, Wilk et al 35 found no correlation between knee flexion strength and hop test performance. Hurd et al 14 noted that quadriceps strength influences performance testing, but emphasized that this effect may be quite small; therefore, they suggested that a combination of factors ultimately influence the functional performance test (FPT) results.
The current study did not investigate the effect that strength and functional test performance has on the ability to return to sports nor ACL retear risk. Symmetrical quadriceps strength before return to sports has been shown to reduce the rate of reinjury in the adult population. 11 Kuenze et al 18 found that women experience a greater magnitude of reduction in quadriceps function after 30 minutes of exercise than men. They postulated that this reduced ability to absorb load through the knee as fatigue sets in may have implications on reinjury.
Perhaps as important as the sex-based differences detected in the study are the similarities between boys and girls. Specifically, both groups, who had undergone hamstring harvest using similar techniques, demonstrated significant donor site morbidity in the form of persistent hamstring weakness greater than 30% when using the LSI metric. Given that the hamstrings may be the most important dynamic stabilizer of the knee, 6 months post ACLR emerges as a clear time point at which the average adolescent undergoing this particular technique may be unable to return to sports safely or effectively. Given the 30% deficit, none of the patients in our cohort were cleared to return to sports at 6 months post ACLR. Despite a trend toward accelerated rehabilitation protocols and return-to-sports allowances closer to 6 months after ACLR over the course of the 1990s and early 2000s, the current study fits with a variety of work in the 2010s that has swung the pendulum back toward the 9- to 12-month postoperative mark for return to sports. 6,11,19,22,28,29 While this current study did not examine functional testing at the 9- to 12-month postoperative time points or offer data on return to sports and ACL retear rate, this clinically significant finding of hamstring weakness in both sexes does warrant further investigation.
“A number of other study findings have clinical significance worthy of attention. Because growing evidence in the literature has suggested that postoperative FPTs can be predictive of patients’ ability to return to sports, consideration can be given toward extra attention to both hamstring strength and quadriceps strength, particularly in female patients for the latter. Given the retrospective design of this current study, return-to-sport recommendations cannot be offered, nor can retear rates be reported at this time. The differences in clinical and functional performance between the sexes are, however, important to recognize. The ultimate role this has in determining the ability to return to sports and avoid new injury between the sexes is being further examined in a prospective manner at this study's institution. Lephart et al 20 demonstrated that patients who reported an ability to return to athletic competition at preinjury levels of competition scored significantly higher on the FPTs than those who were unable to do so. Those authors recommended implementation of FPTs when establishing criteria for return to competition. Performance on functional testing has also been correlated to patient-reported functional outcome scores such as the Knee Injury and Osteoarthritis Outcome Score and International Knee Documentation Committee. 12
Several study limitations warrant discussion. This was a nonconsecutive series of patients who underwent surgery by 1 of 6 sports surgeons. All strength testing was performed through manual muscle testing, and therefore they may be subject to human error or inconsistency affecting the results. However, strength was compared in each patient between the lower extremity side that had previously undergone surgery and the contralateral, non-surgical side in sequence on the same day by a single athletic trainer, which allowed for consistency in measurement technique and the creation of a true ‘control limb' against which the ‘study limb' was compared. 31 Also, the testing protocol did not include standardization of the position of the dynamometer, potentially allowing longer limbs to produce lower force at the dynamometer for a given amount of muscle force applied. While this ought to have been corrected by comparisons between limbs, more standardized testing techniques might have been preferable. Another limitation is that there may have been variation in postoperative rehabilitation protocols between providers or different interpretation and implementation of the protocol between physical therapists. However, this variation may be more representative of the experience of a larger population, and therefore makes the current results more generalizable than use of a specific or individual protocol that may not be favored by other clinicians. Additionally, we recognize that preoperative quadriceps strength correlates with postoperative quadriceps strength and single-leg hop performance. 33 Given the retrospective nature of the data, we were unable to compare preoperative strength between the sexes. Finally, we recognize the potential for sampling bias, as patients were selected from those who participated in functional testing at our injury prevention center 6 months after surgery. However, these patients represent the vast majority of the population that we treat as this 6-month functional testing is performed by almost all postoperative patients, regardless of the location of their physical therapy.
Conclusion
When assessing lower extremity recovery and performance testing 6 months after ACLR with hamstring autograft, adolescent girls demonstrated a deficit in quadriceps strength that was statistically significantly different from the quadriceps strength surplus detected in adolescent boys. There was no significant difference in the functional hop testing between boys and girls nor in the hamstring strength deficits, which were approximately 33% in both groups, when compared with the contralateral limb. Additional research is needed to further explore the association of the described hamstring strength deficits with clinical outcomes such as ACL retear and functional outcomes as elucidated by patient-reported outcome measures. Overall, these data may support delaying return to sports beyond 6 months postoperatively, which has also been suggested in more recent literature.
Footnotes
Final revision submitted May 20, 2021; accepted June 23, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.M. has received education payments from Smith & Nephew. M.S.K. has received consulting fees and royalties from OrthoPediatrics and hospitality payments from Smith & Nephew. B.E.H. has received education payments from Arthrex and Kairos Surgical and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Boston Children’s Hospital (protocol No. IRB-P00015975).