
Abstract
Background:
In patients with femoroacetabular impingement, preoperative diagnostic injections are commonly used to establish a diagnosis of intra-articular pathology. In some cases, intra-articular steroid injections are also used for therapeutic purposes.
Purpose/Hypothesis:
The purpose of this study was to determine if a positive response to intra-articular steroid injection was predictive of superior outcomes after hip arthroscopy to determine if the response to intra-articular steroid injection was predictive of outcomes after hip arthroscopy. It was hypothesized that a positive response to a preoperative hip injection would be predictive of improved short- to midterm outcomes after hip arthroscopy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a retrospective study of 208 patients who elected to have ultrasound-guided intra-articular steroid injection before they underwent hip arthroscopy between January 2016 and December 2016. Patients were divided into 2 groups: those who showed improvement in pain after the injection (steroid responder group) and those who showed no response (nonresponder group). The authors compared the preoperative and 2-year postoperative patient-reported outcomes (modified Harris Hip Score [mHHS] and Hip Outcome Score–Activities of Daily Living [HOS-ADL]) and radiographic findings between groups. Clinical endpoints, including rates of revision and conversion to total hip arthroplasty, were also reviewed.
Results:
There were 88 patients in the nonresponder group and 120 patients in the responder group, with no significant between-group differences in preoperative descriptive variables. The responder group had significantly higher 2-year mHHS and HOS-ADL, pre- to postoperative change in mHHS and HOS-ADL, percentage of patients achieving the patient acceptable symptomatic state (PASS) on the mHHS, and percentage of patients reaching the minimum clinically important difference and the PASS on the HOS-ADL. There was no difference in Tönnis grade, acetabular labrum articular disruption grade, revision rate, or conversion to total hip arthroplasty between the 2 groups.
Conclusion:
The response to preoperative intra-articular injection did aid in predicting 2-year patient-reported outcomes of hip arthroscopy for femoroacetabular impingement. Overall, the result of a preoperative intra-articular injection can be a helpful clinical tool for surgical decision-making and counseling patients on expected outcomes after hip arthroscopy.
Femoroacetabular impingement (FAI) is a distinct pathologic entity characterized by an abnormal anatomic relationship between the proximal femur and acetabulum. 3 Repetitive contact between an aspherical femoral head and acetabular rim is associated with chondral damage and subsequent development of osteoarthritis if the underlying cause is not corrected. 1,10,17,22 In cases of failed nonoperative treatment, FAI can be surgically corrected via arthroscopic intervention aimed at resection of impinging structures and management of chondral and labral pathology. 16 Prospective studies of arthroscopic treatment for FAI have shown stable functional improvement postoperatively. 11,13,31 When compared with nonoperative management, arthroscopic intervention produces clinically meaningful improvements in function, with few associated side effects and minimal progression to osteoarthritis. 12,27
Despite continued efforts to standardize the diagnosis of FAI, it remains challenging to definitively determine the contribution of intra-articular pathology to patients’ symptoms. 29 The differential diagnosis of hip pain is broad and includes both intra-articular and extra-articular pathology. 24 Physical examination maneuvers to evaluate for intra-articular pathology are associated with both high false-negative and high false-positive rates and are therefore limited in diagnostic value. 24,29 Further diagnostic studies include radiographs and magnetic resonance imaging (MRI). Often a diagnostic injection with local anesthetic with or without corticosteroids may help aid in the diagnosis of FAI as a cause of hip pain. 9,15 Although a patient may or may not have concurrent extra-articular pathology, this does not alter the diagnostic value of hip injections. 17,18
Although FAI is a structural abnormality, there are varied reports of symptomatic improvement after an intra-articular injection of corticosteroids. 10,23 There are limited data regarding the therapeutic value of injections, although smaller studies have shown limited sustained improvement after injection. 19,14 In patients with chondral injury there may be added therapeutic value, as well as diagnostic value, to injections. 23
Regardless, intra-articular corticosteroid injections remain a valuable diagnostic tool in the diagnosis of FAI. In this study, we sought to evaluate the response to intra-articular injections as a prognostic tool for patient-reported outcomes 2 years after arthroscopic intervention for FAI. We hypothesized that patients who responded with symptomatic relief to a preoperative intra-articular injection would have more favorable 2-year patient-reported outcomes after arthroscopic intervention and labral repair.
Methods
After receiving institutional review board approval, we performed a retrospective review of prospectively collected data at a large, high-volume hip arthroscopy center. Patients were eligible for study enrollment if they were between the ages of 16 and 65 years and underwent hip arthroscopy by the senior surgeon (K.J.E.) between January 2016 and December 2016. Patients who had received an intra-articular steroid injection before surgery, had undergone hip arthroscopic intervention with labral repair, and had at least 2 years of follow-up were enrolled. Patients with a Tönnis grade >2 and those who had a history of previous ipsilateral hip surgery, fracture, slipped capital femoral epiphysis, avascular necrosis, systemic inflammatory disease, or dysplastic or borderline dysplastic hips (center-edge angle, <25°) were excluded. In addition, we excluded patients who underwent isolated or concomitant lateral hip surgery, either open or endoscopic, including greater trochanteric bursectomy and gluteal tendon repair.
A total of 366 patients with clinical and radiologic evidence of FAI underwent hip arthroscopy during the 12-month study period. Six patients were excluded for concomitant lateral procedures; 34, for revision surgery; 10, for Tönnis grade >2; and 24, for dysplasia or borderline dysplasia. In addition, 34 patients were lost to follow-up. This left a total of 258 patients with 2-year follow-up data. Of these patients, 208 had received an intra-articular steroid injection before surgery and were included in the study (Figure 1). All patients in this series had undergone arthroscopic labral repair, femoral/acetabular osteoplasty, and capsular closure.

Flowchart for patient inclusion and exclusion. CEA, center-edge angle; FAI, femoroacetabular impingement.
All patients enrolled in the study had undergone nonoperative treatment before surgery. Nonoperative treatment included at least 3 months of formal physical therapy, activity modifications, nonsteroidal anti-inflammatory drugs, and rest. All patients were offered an ultrasound-guided steroid injection. Only those who underwent injection were included in the study. All injections were performed within 6 months of surgery. Two milliliters of 3 mg/mL betamethasone and 5 mL of 1% lidocaine without epinephrine were intra-articularly injected into the hip under ultrasound guidance before surgery in our patient population.
Depending on their response to the intra-articular injections, the patients were divided into 2 groups: Those who had any subjective improvement in pain after the injection were placed in the steroid responder group, and those who showed no response were included in the steroid nonresponder group. Response to injection was defined as any subjective improvement for any length of time as identified by the patient at first follow-up after injection. Failure to respond was defined as no subjective improvement as identified by the patient at first follow-up after injection.
Surgical Technique
Each patient underwent standard hip arthroscopy in the lateral position under general anesthesia with full muscle relaxation. The patient was placed in the lateral decubitus position stabilized via a bean bag with the operative leg up. A lateral hip distractor (Smith & Nephew) was used for distraction using a well-padded traction boot on the operative leg. The nonoperative leg was left free. All bony prominences were well protected. Three portals, including the anterior, anterolateral, and midanterior portals, were used for all surgeries. In all patients, an interportal capsulotomy was performed to allow visualization of the entire joint. Initial arthroscopy was used to evaluate the cartilage and ligamentum teres. Attention was then turned to the labrum. All patients in the study underwent labral repair; no patients underwent labral debridement. Labral repair was performed using Knotless SutureTaks (Arthrex). The number of anchors used during the case was determined by the size of the tear. Femoral osteoplasty was then performed with traction off using a 4- or 5.5-mm bur depending on the size of the cam lesion. A No. 2 FiberWire suture (Arthrex) was placed in the anterior and posterior aspects of the distal leaflet of the capsulotomy and used to retract the capsule back to allow visualization of the femoral head-neck junction. After performing femoral osteoplasty, the surgeon confirmed appropriate bone removal using fluoroscopy and dynamic arthroscopy, and appropriate bone removal was confirmed using fluoroscopy and dynamic arthroscopy. The interportal capsulotomy was closed using No. 3 FiberWire sutures (Arthrex) placed in interrupted fashion using a suture-passing device.
Postoperatively, patients were 50% weightbearing for 2 weeks followed by weightbearing as tolerated. All patients underwent the same physical therapy protocol after surgery. External rotation past 10° was avoided in all patients for the first 2 weeks.
Data Collection
Manual chart review of all included patients was completed in the electronic medical record by multiple reviewers (T.M., J.D.H., K.J.E.). Patient characteristics were reviewed, as were outcomes of prior physical therapy. Preoperative and 2-year postoperative patient-reported outcome scores (modified Harris Hip Score [mHHS] and Hip Outcome Score–Activities of Daily Living subscale [HOS-ADL]) were assessed. Radiographic and intraoperative factors assessed were Tönnis grade, acetabular labrum articular disruption (ALAD) grade, and pre- and postoperative alpha angle as measured on frog-leg lateral radiographs. Clinical endpoints, including rates of revision and conversion to total hip arthroplasty (THA), were also reviewed.
Data Analysis
Comparison statistics between the responder and nonresponder groups were performed for continuous variables utilizing t tests. In addition, improvement of each group was compared using previously reported anchor-based minimum clinically important difference (MCID) and patient acceptable symptomatic state (PASS). 6,21,30 Significance was set with an alpha of .05. Statistical analysis was conducted using SPSS (Version 25, IBM Corp).
Results
There were 88 patients identified who had no response to intra-articular injection (steroid nonresponder group; age, 38.61 ± 12.54 years; 44 men and 44 women; BMI, 26.42 ± 4.43). A total of 120 patients who did positively respond to steroids were identified (steroid responder group; age, 37.48 ± 12.56 years; 65 men and 55 women; BMI, 26.08 ± 4.17). The groups had similar characteristics (Table 1).
Comparison of Characteristics by Steroid Response Group a
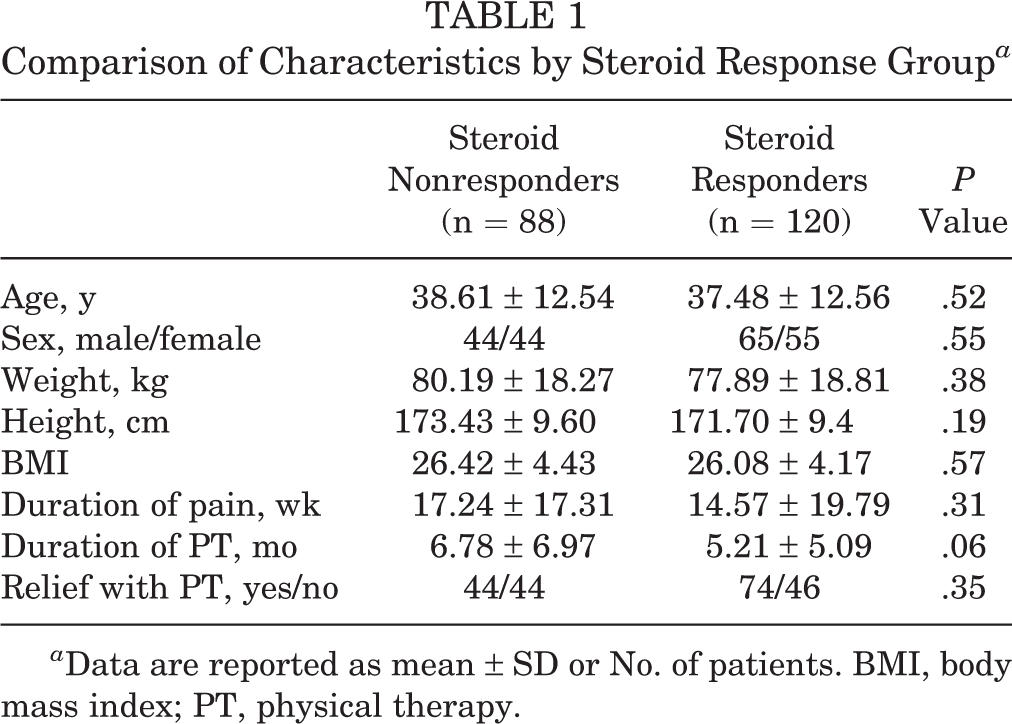
a Data are reported as mean ± SD or No. of patients. BMI, body mass index; PT, physical therapy.
In the nonresponder group, there was an average improvement of 22.28 points in the mHHS (Table 2 and Figure 2A). The MCID was achieved in 79 patients (90%), and the PASS was achieved in 55 patients (63%). The average improvement in HOS-ADL was 22.21 points (Figure 2B), with the MCID achieved in 79 patients (90%), and the PASS achieved in 23 patients (26%). Compared with the nonresponder group, the responder group saw greater improvement in all outcome metrics except for MCID on the mHHS: 2-year postoperative improvement of 26.78 points in the mHHS (P = .01), with the MCID achieved in 113 patients (94.0%; P = .24) and the PASS achieved in 103 patients (86%; P < .01), and improvement of 28.82 points in the HOS-ADL (P < .01), with the MCID achieved in 117 patients (98%; P = .02) and the PASS achieved in 62 patients (52%; P < .01) (Table 2).
Comparison of Patient-Reported Outcomes by Steroid Response Group a
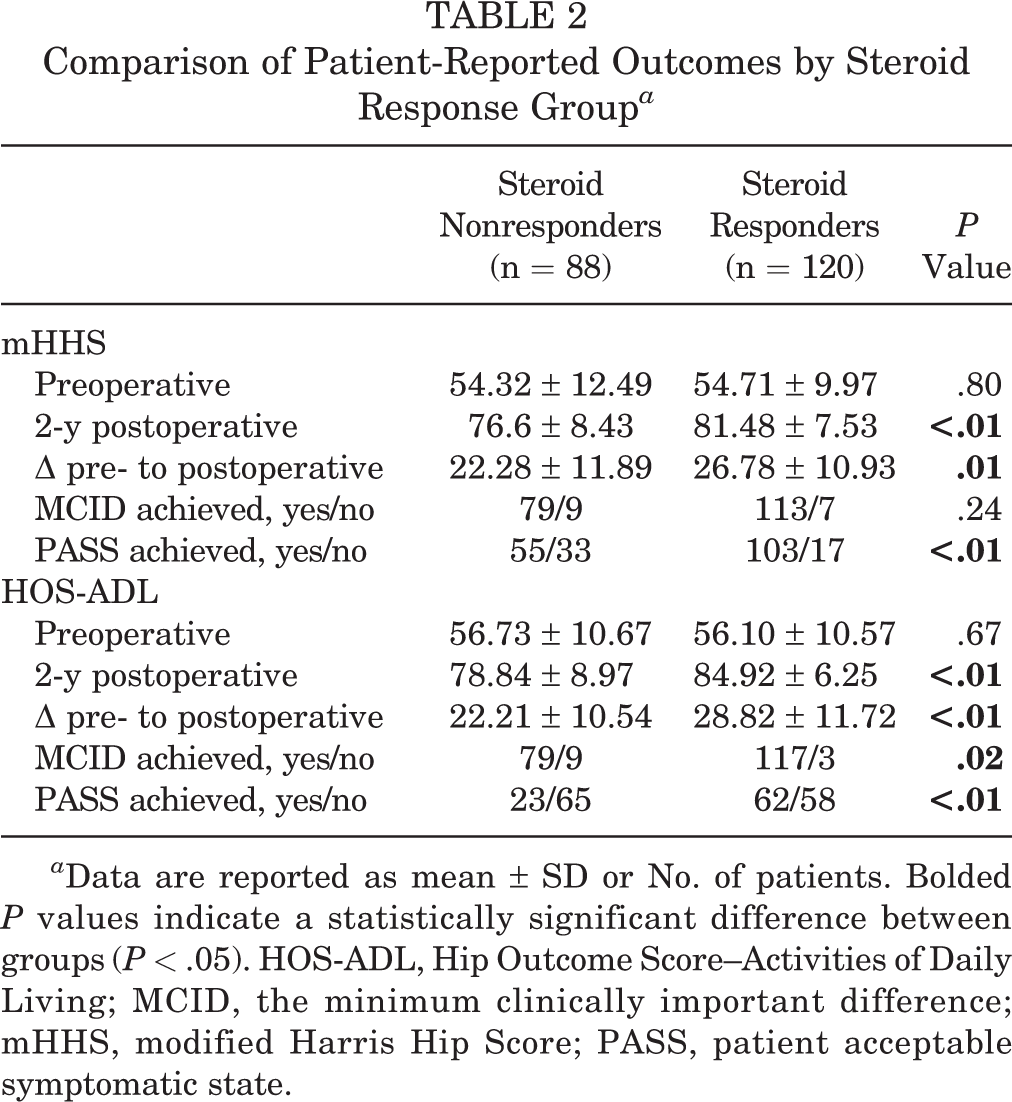
a Data are reported as mean ± SD or No. of patients. Bolded P values indicate a statistically significant difference between groups (P < .05). HOS-ADL, Hip Outcome Score–Activities of Daily Living; MCID, the minimum clinically important difference; mHHS, modified Harris Hip Score; PASS, patient acceptable symptomatic state.

Pre- and postoperative (A) modified Harris Hip Score (mHHS) and (B) Hip Outcome Score–Activities of Daily Living (HOS-ADL) in patients who had no response to intra-articular steroid injections (steroid nonresponder) versus those who had a positive response (steroid responder). *Statistically significant difference between groups (P < .05).
The radiographic and intraoperative findings between groups are shown in Table 3. The postoperative alpha angle was significantly greater in the nonresponder group than the steroid responder group (45.27 ± 3.43 and 43.71 ± 4.83, respectively; P = .01). There was no statistically significant difference in mean Tönnis grade or mean ALAD grade between the 2 groups.
Comparison of Radiographic and Intraoperative Findings by Steroid Response Group a
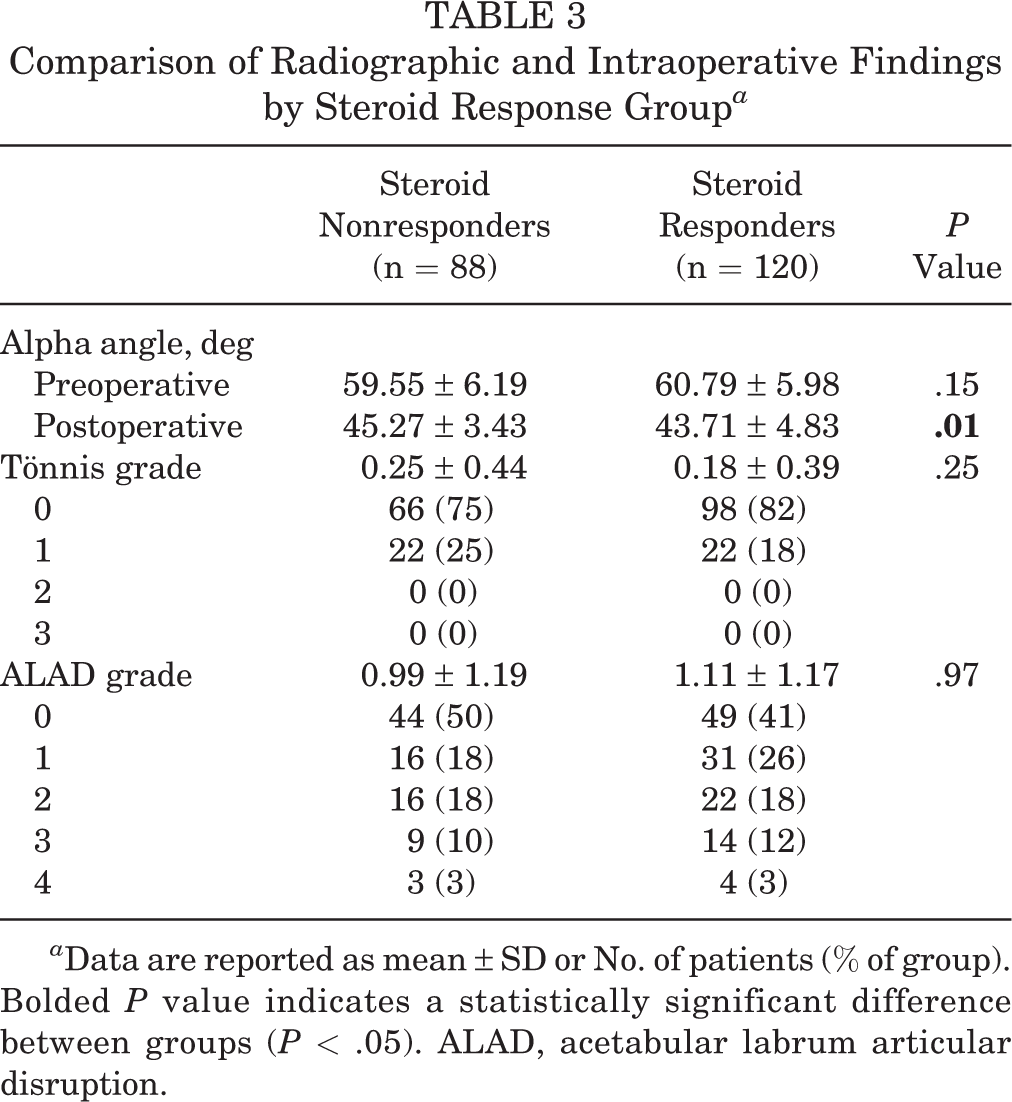
a Data are reported as mean ± SD or No. of patients (% of group). Bolded P value indicates a statistically significant difference between groups (P < .05). ALAD, acetabular labrum articular disruption.
Regarding complications, 4 patients (5%) in the nonresponder group underwent revision surgery compared with 6 patients (5%) in the steroid responder group (P = .88). To date, none of the patients has undergone conversion to THA.
Discussion
Overall, the findings of this study suggest that there is prognostic value in response to intra-articular steroid injections as a predictor of patient-reported outcomes after arthroscopic intervention in patients with FAI. There was a significant difference between patients who responded to the intra-articular injections and those who did not respond to injections regarding mHHS (P < .01) and HOS-ADL (P < .01) at the 2-year follow-up. In addition, 94% of the responder group achieved the MCID for mHHS, and 86% achieved the PASS as compared with 90% and 63%, respectively, for the nonresponder group (P = .24 and P < .01, respectively). For HOS-ADL, 98% of the responder group achieved the MCID, and 52% achieved the PASS as compared with 90% and 26%, respectively, for nonresponders (P = .02 and P < .01, respectively). However, there was no significant difference in the rates of revision surgery or conversion to THA.
Radiographic findings, including preoperative alpha angle and Tönnis grade, and arthroscopic findings (ALAD grade) also did not differ between the 2 groups. Postoperative alpha angles did differ between the 2 groups (P = .01); however, this radiographic measurement of <2° was small and not clinically relevant. These findings suggest that in patients who receive injections for diagnostic purposes, there is prognostic value in regard to patient-reported outcomes but not in regard to rates of revision surgery or conversion to THA.
To our knowledge, few studies have evaluated the relationship between response to intra-articular injection and arthroscopic outcomes. One such study demonstrated positive correlation between diagnostic injections and 1-year patient-reported outcomes. 8 However, Krych et al 20 concluded that injections were poor predictors of patient-reported outcomes at an average of 14.8 months after arthroscopy. They recommended that imaging studies and positive provocative physical examination maneuvers rather than response to injections should guide decisions regarding whether or not to proceed with surgery. Ayeni et al 2 noted similar findings in their prospective study with patient-reported outcomes obtained 6 months postoperatively. However, they noted that lack of response to intra-articular injection reduced the posttest probability of positive surgical outcome more than a positive response to injection increased the posttest probability of a positive surgical outcome. Our study adds to the existing literature by evaluating outcomes in the short to midterm with data 2 years postoperatively. This demonstrates that while there may not be prognostic value for intra-articular steroid injections in the short term, a positive response to injections may be predictive of improved patient-reported outcomes in the mid- to long term.
Although there are limited data regarding the prognostic value of intra-articular injections in FAI and labral tears, the diagnostic value is well established. Byrd and Jones 5 have previously shown that positive response to intra-articular anesthetic injections is 90% accurate in identifying intra-articular pathology. Pain relief after injection can be interpreted to indicate the presence of intra-articular pathology regardless of the presence of simultaneous extra-articular hip pathology. In patients with cam-type FAI, approximately 81% of patients respond to injections. 18 Pateder and Hungerford 25 have previously studied the utility of fluoroscopically guided intra-articular hip injections in differentiating hip versus lumbar spine sources of pain. They reported a sensitivity of 100% and specificity of 81%. The diagnostic value of intra-articular injections is thus well established. However, the therapeutic value remains uncertain, with some anecdotal reports of clinical success and larger studies reporting limited therapeutic benefit. 18,19,25 Krych et al 19 reported a 37% positive response in patients with FAI undergoing intra-articular steroid injections for therapeutic purposes.
As such, diagnostic response may be helpful in confirming pain contributions of intra-articular pathology; however, it has not been shown to be prognostic of outcomes after hip arthroscopy in the past. This may be related to the structural nature of FAI. Hip arthroscopy directly targets the structural abnormalities, while intra-articular steroids primarily modulate the inflammatory response within the joint. The cause of FAI is multifactorial and encompasses a combination of genetic, developmental, and activity-related factors. 7,10,28 Repetitive structural impingement contributes to microtrauma and cartilage turnover. In athletes with FAI, Bedi et al 4 noted a 276% increase in C-Reactive Protein (CRP) levels as well as biochemical signs of increased cartilage turnover and systemic inflammation. Patients with a more prominent systemic inflammatory component as a result of chronic FAI are more likely to experience pain relief after a diagnostic intra-articular steroid injection. However, when used therapeutically, the injection often has a short-lived benefit. The majority of nonoperative measures often fail because of the continued presence of structural abnormality and microtrauma caused by repetitive hip motion. 15
Traditionally, surgical prognosis for FAI treated with hip arthroscopy has been challenging. 26,30 To assess who would be the most likely to benefit the most from surgical intervention, we evaluated the prognostic value of response to intra-articular steroid injections. Our data suggest that response to steroid injection does predict positive response and improvement in patient-reported outcomes after surgical intervention. However, poor response to steroid injection does not preclude improvement with hip arthroscopy in the correct patient group with true radiographic and clinical FAI symptoms. Although prior studies have shown limited prognostic value of steroid injections in the short term, our data suggest increased prognostic value in the short to midterm, indicating that there may be a postoperative inflammatory response contributing to pain in the short term that resolves over time. 2,8,20 It is likely that resolution of this inflammation combined with correction of the underlying mechanical abnormality contributes to overall improved patient outcomes.
Our study has several limitations, including the small sample size and the retrospective nature of the study. Additionally, although we included ALAD grades, we did not study the extent of chondral damage and severity of labral tearing, which could potentially affect patient-reported outcomes. In addition, this study is limited in that only patients undergoing arthroscopy by a single surgeon were included. Although this assisted in controlling for confounding in surgical technique and rehabilitation protocols, it does limit generalizability. Finally, our study did not include long-term follow-up.
Conclusion
A positive response to preoperative steroid injection in patients with FAI did positively predict higher patient-reported outcomes at the 2-year postoperative time point compared with no response. However, both responders and nonresponders showed significant increases in all outcome scores at the 2-year follow-up compared with preoperative levels. Response versus nonresponse can be a helpful clinical tool for surgical decision-making and counseling patients on expected outcomes.
Footnotes
Final revision submitted June 29, 2021; accepted August 6, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D.H., J.L.M., and K.A.P. have received education payments from Arthrex. K.J.E. has received education payments from Arthrex and consulting fees from Arthrex, Desert Mountain Medical, Smith & Nephew, and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mayo Clinic Arizona (study No. 1251075).