
Abstract
Background:
The loss of extensor mechanism continuity that occurs with patellar and quadriceps tendon rupture has devastating consequences on patient function.
Purpose:
To describe a treatment strategy for extensor mechanism disruption and evaluate the outcomes of 3 techniques: primary repair, repair with semitendinosus tendon autograft augmentation, and reconstruction with Achilles tendon allograft.
Study Design:
Case series; Level of evidence, 4.
Methods:
The authors reviewed surgeries for extensor mechanism disruption performed by a single surgeon between 1999 and 2019. Patient characteristics, imaging studies, surgical techniques, and outcomes were recorded. Primary ruptures with robust tissue quality were repaired primarily, and first-time ruptures with significant tendinosis or moderate tissue loss were repaired using quadrupled semitendinosus tendon autograft augmentation. Patients with failed previous extensor mechanism repair or reconstruction and poor tissue quality underwent reconstruction with Achilles tendon allograft. The primary outcome was extensor mechanism integrity at a minimum 1-year follow-up, with extensor mechanism lag defined as >5° loss of terminal, active knee extension. Secondary outcomes included postoperative knee range of motion, International Knee Documentation Committee (IKDC) and Tegner activity scores, and the radiographic Caton-Deschamps Index.
Results:
Included were 22 patellar tendon and 21 quadriceps tendon surgeries (patients: 82.5% male; mean age, 48.1 years; body mass index, 31). Seventeen (39.5%) cases underwent primary tendon repair, 13 (30.2%) had repair using semitendinosus tendon autograft augmentation, and 13 (30.2%) underwent reconstruction using an Achilles tendon allograft. Seventeen (39.5%) cases had at least 1 prior failed extensor mechanism surgery performed at an outside facility. At the last follow-up, 4 (9.3%) cases had an extensor mechanism lag, no cases required additional extensor mechanism surgery, and all cases were able to achieve >90° of knee flexion. Postoperative IKDC scores were significantly improved with all methods of extensor mechanism surgery, and postoperative Tegner activity scores were significantly improved in patients who underwent primary repair and Achilles tendon allograft reconstruction (P < .05 for all).
Conclusion:
Primary repair alone, repair using quadrupled semitendinosus tendon autograft augmentation, and reconstruction using Achilles tendon allograft were all effective methods to restore extensor mechanism and knee function with the proper indications. Persistent knee extensor lag was more common in chronic extensor mechanism injuries after failed surgery, although patients still reported significantly improved postoperative functional outcomes.
Keywords
Patellar and quadriceps tendon ruptures are uncommon injuries that can have devastating consequences on patient function because of loss of extensor mechanism continuity. Patellar tendon ruptures typically occur in active patients aged <40 years, and quadriceps tendon ruptures are commonly seen in patients aged >40 years. 24 Extensor mechanism rupture is caused by a rapid eccentric quadriceps contraction with the knee in a flexed position. 8,17 Patients describe acute pain, a tearing or popping sensation in the knee, the inability to actively extend the knee or maintain full knee extension against gravity, swelling, and a palpable suprapatellar (quadriceps tendon) or infrapatellar (patellar tendon) gap. 8,17,24 Tendon rupture likely results from chronic tendon degeneration after repetitive microtrauma to the knee and is typically unilateral. 9,11,28 Quadriceps tendon ruptures are more commonly seen in patients with underlying medical diseases. Systemic disorders such as autoimmune diseases, diabetes mellitus, renal disease, obesity, and chronic use of corticosteroids may accelerate degeneration of both patellar and quadriceps tendons, predisposing to bilateral tendon ruptures. 5,13,14,22,25,27
Management of acute extensor mechanism ruptures includes urgent, end-to-end primary repair for midsubstance disruptions or nonabsorbable transosseous patellar sutures or suture anchors for osteotendinous junction ruptures. 6,8,11,17 Chronic extensor mechanism injuries can be more difficult to treat because of tendon scarring, retraction, and poor tissue quality. Multiple surgical options, including primary repair, repair with various methods of augmentation, or reconstruction with a tendon graft, exist. 3,6,10 The goals of this study were to present a treatment strategy for extensor mechanism ruptures and to evaluate the outcomes of 3 techniques: primary extensor mechanism repair, repair using semitendinosus tendon autograft augmentation, and reconstruction using Achilles tendon allograft.
Methods
This was a retrospective case series of extensor mechanism restoration from a single surgeon who evaluates postoperative knee extension, patient function, and radiographic patellar position. After receiving institutional review board approval, we reviewed all surgeries for extensor mechanism disruption performed by a single surgeon (M.J.S.) between 1999 and 2019 at a single institution; 45 patients with extensor mechanism repair were initially identified. Patients with extensor mechanism rupture associated with a total knee arthroplasty or tumor were excluded (n = 5). After application of exclusion criteria, 40 patients with 43 extensor mechanism restoration procedures were identified. All patients had a minimum of 1 year of follow-up.
Patient characteristics, imaging studies, surgical technique, and outcomes were recorded. Primary ruptures with robust tissue quality were repaired primarily. Primary ruptures with significant tendinosis or moderate tissue loss were treated with a novel semitendinosus tendon autograft augmentation technique. Reconstruction using Achilles tendon allograft was performed on patients with previous extensor mechanism surgeries and poor tissue quality. The specific surgical procedure was subjectively chosen by a single surgeon based on patient age and medical comorbidities, history of prior extensor mechanism surgeries, evidence for enthesopathy, chronic tendinopathy or tendon gapping on preoperative magnetic resonance imaging (MRI) scans, and intraoperative tissue quality assessment. No standardized scoring methods for tissue quality were used, and all patients gave consent for the possibility of all 3 surgical options based on intraoperative findings and surgeon judgment.
The principal outcome was extensor mechanism integrity at a minimum 1-year follow-up, with extensor mechanism lag defined as >5° loss from full extension (0°) of seated, active terminal knee extension. This determination was made on manual physical examination and was compared with the contralateral knee by the senior author and operating surgeon (M.J.S.). Additional outcomes included knee range of motion, postoperative International Knee Documentation Committee (IKDC) and Tegner activity scores, and postoperative radiographic Caton-Deschamps Index at the last follow-up.
Primary Repair Technique
The surgical technique for primary patellar or quadriceps tendon repair began with exposure and then evaluation of the tissue quality and gapping at the rupture site. The tendon ends were debrided of nonviable tissue, and 2 No. 2 nonabsorbable locking whipstitch sutures (Arthrex) were placed in the distal (quadriceps) or proximal (patellar) tendon remnant. Three parallel, longitudinal drill holes were placed in the patella, and the 4 suture ends were passed through the drill holes. Two suture anchors were placed in the proximal patellar pole (quadriceps tendon) or distal patellar pole (patellar tendon), and these sutures were passed into the tendon remnant. The tendon was then anatomically reduced to the patella, and all sutures were tied, providing dual fixation using both transosseous sutures and suture anchors. The tendon ends and tear extension into the retinaculum were closed using interrupted No. 0 Vicryl (Ethicon) suture. 12
Semitendinosus Tendon Autograft Augmentation Technique
The surgical technique for primary patellar or quadriceps tendon repair using semitendinosus autograft augmentation began with exposure and debridement of nonviable tissue at the ruptured tendon ends, followed by placement of 2 No. 2 nonabsorbable locking whipstitches in the tendon remnant. The ipsilateral semitendinosus tendon was harvested in a standard fashion and cleaned of any remaining muscle fibers. A No. 0 nonabsorbable locking whipstitch suture was placed on the proximal and distal ends. The graft was passed through a TightRope device (Arthrex) and folded in half to create 2 arms of equal length. The folded graft size was measured to determine the diameter of the patellar socket (typically 5-6 mm). Attention was then turned to the patella. Enthesophytes were removed to expose healthy, bleeding bone (distal patellar surface for patellar tendon rupture and proximal patellar surface for quadriceps tendon rupture). A spade-tipped guide pin was inserted in the central aspect of the patellar pole and directed out the opposite patellar pole. Two parallel, longitudinal 2.5-mm drill holes were placed approximately 10 mm medial and lateral to the central hole. A cannulated reamer equal to the diameter of the doubled semitendinosus tendon was placed over the central guide pin to create a 10 mm–deep patellar socket (Figures 1 and 2).

Drill hole placement for patellar tendon primary repair using semitendinosus augmentation.
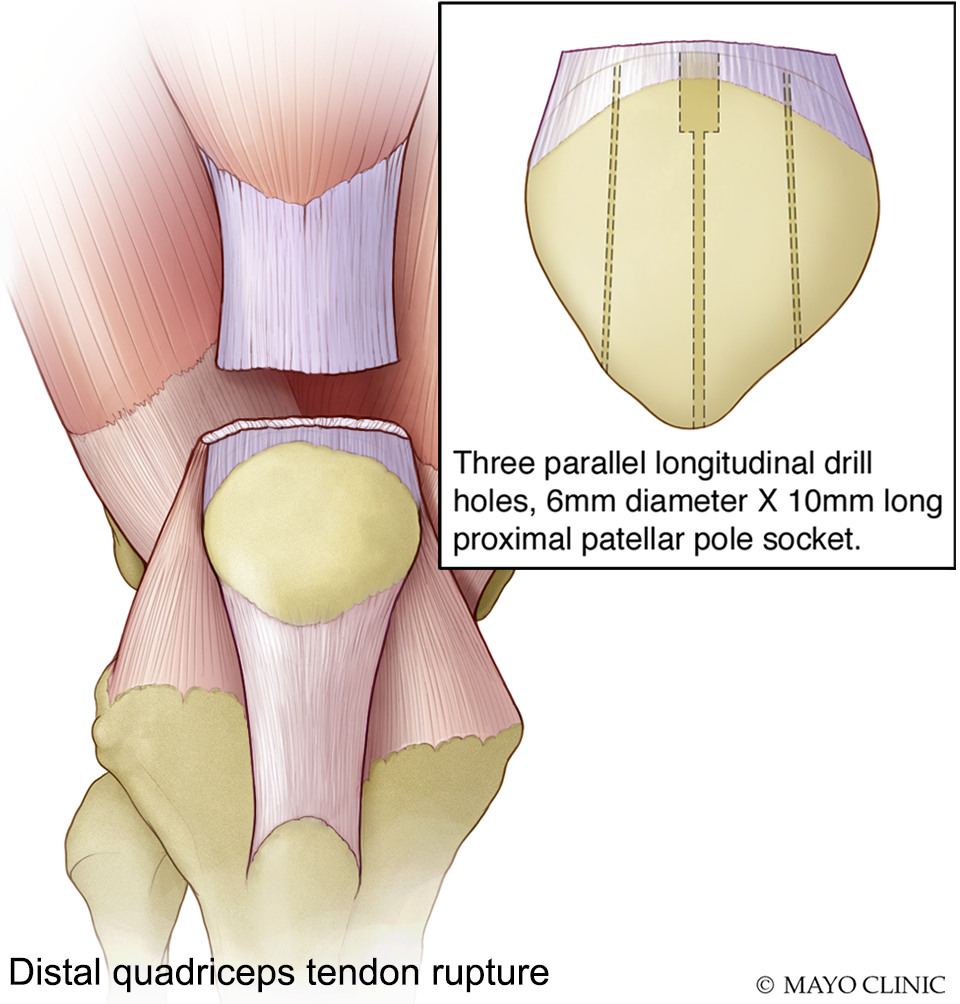
Drill hole placement for quadriceps tendon primary repair using semitendinosus augmentation.
Two suture anchors were then inserted on either side of the socket. The ends of the No. 2 nonabsorbable locking whipstitch suture in the native tendon remnant were passed through the medial and lateral transosseous tunnels, and the 2 central sutures along with the TightRope sutures were passed through the central patellar tunnel. The TightRope button was flipped and engaged on the opposite patellar pole, and the shortening strands were used to dock the doubled semitendinosus tendon graft into the patellar socket. The native tendon remnant sutures were tensioned and tied over the opposite patellar pole. This restores patellar height in the setting of a patellar tendon rupture. The anchor sutures were passed through the native tendon and tied, creating the dual-repair construct. In the case of patellar tendon augmentation, the 2 arms of the graft were crossed and passed underneath the intact distal tendon, sutured, and then flipped proximally and sutured to the native tendon and patella. In the case of quadriceps tendon augmentation, the 2 arms of the graft were passed through a longitudinal split in the intact proximal tendon, sutured, and then flipped distally and sutured to the native tendon and patella. This technique creates a dual-repair construct with a 4-stranded (quadrupled) semitendinosus tendon autograft augmentation (Figures 3 and 4). 29

Final construct for patellar tendon primary repair using semitendinosus tendon autograft augmentation. The doubled graft is inserted into the distal patellar pole socket with suspensory fixation on the proximal pole. The 2 arms of the graft are passed through a longitudinal split in the intact distal tendon and then flipped proximally and sutured to the native tendon and patella.
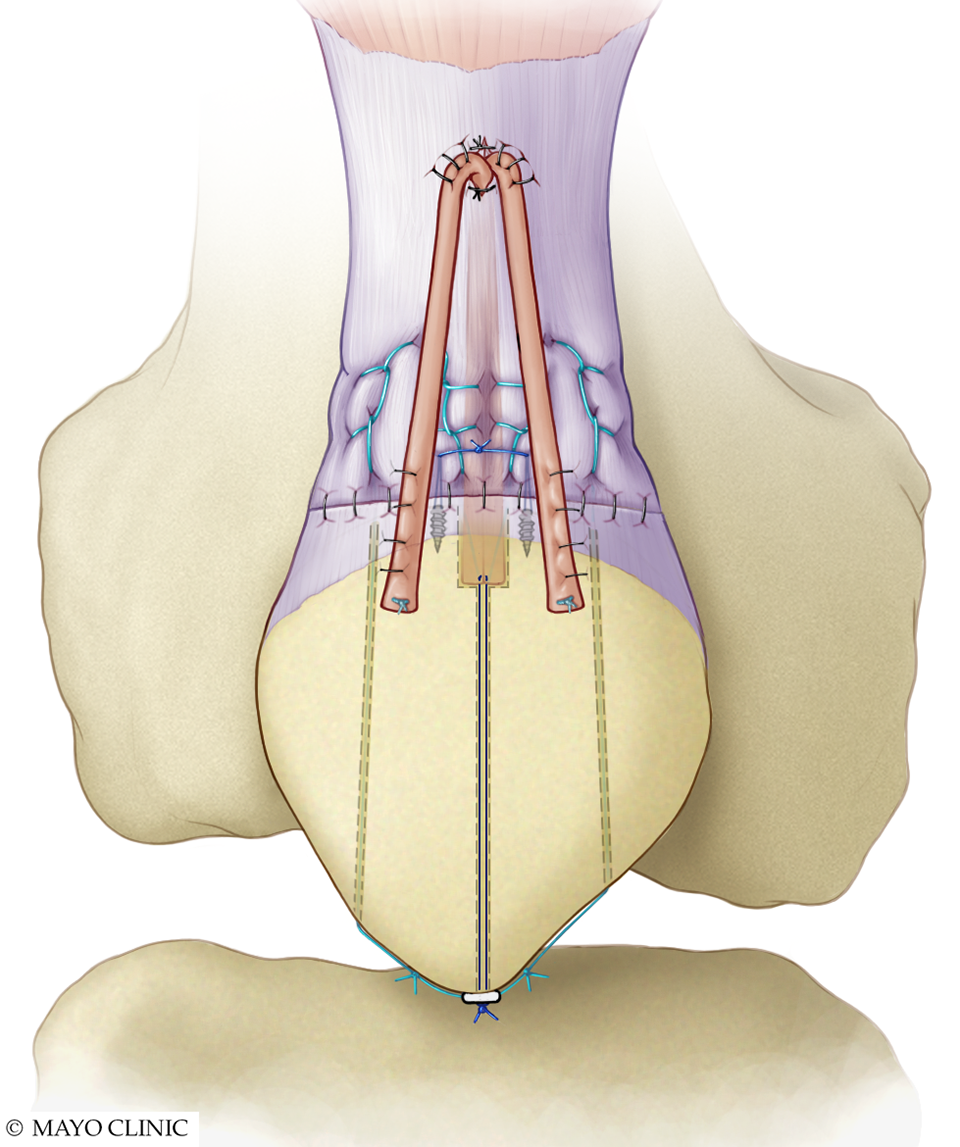
Final construct for quadriceps tendon primary repair using semitendinosus autograft augmentation. The doubled graft is inserted into the proximal patellar pole socket with suspensory fixation on the distal pole. The 2 arms of the graft are passed underneath the intact proximal tendon and then flipped distally and sutured to the native tendon and patella.
Reconstruction Using Achilles Tendon Allograft Technique
The surgical technique for extensor mechanism reconstruction used an Achilles tendon allograft with a calcaneus bone block. For patellar tendon reconstruction, the calcaneus bone block was fashioned to fit into a trapezoidal tibial tubercle recipient site. The bone block was press-fit and then fixed to the tibial site using a single countersunk cortical lag screw. Two suture anchors were placed just proximal to the tubercle, passed through the Achilles tendon, and tied to further secure the allograft distally. Two No. 2 nonabsorbable locking whipstitch sutures were placed in the allograft, and 2 No. 2 nonabsorbable locking whipstitch sutures were placed in the remaining native patellar tendon remnant. Enthesophytes, if present, were removed to expose healthy, bleeding distal patellar bone. Three parallel longitudinal drill holes were placed through the patella. The allograft and native tendon sutures were passed through the drill holes and tensioned to recreate the native patellar height using fluoroscopic guidance and then tied over the proximal patellar pole. The allograft was secured to the native patellar tendon using interrupted No. 0 Vicryl sutures. The remaining Achilles tendon allograft was sutured to the quadriceps tendon, flipped distally, and secured using interrupted sutures, creating a doubled Achilles tendon allograft reconstruction (Figure 5).

Patellar tendon reconstruction using Achilles tendon allograft. (A) Tibial tubercle trough and 3 parallel, longitudinal patellar drill holes. (B) Calcaneus bone block fixed with a cortical lag screw and suture anchor; allograft sutures were passed through the patellar drill holes and then tied. (C) Allograft is passed through and sutured to the intact proximal quadriceps tendon. (D) Allograft is flipped distally and sutured to the native patellar tendon, creating a doubled Achilles tendon allograft reconstruction.
For quadriceps tendon reconstruction, enthesophytes were removed to expose healthy, bleeding distal patellar bone. Three longitudinal drill holes were placed in the patella, and 2 suture anchors were placed between the drill holes. Two No. 2 nonabsorbable locking whipstitches were placed in the Achilles tendon graft, and 2 No. 2 nonabsorbable locking whipstitches were placed in the remaining native distal quadriceps tendon (if present). Three longitudinal drill holes were placed through the Achilles calcaneus bone block, and the anchor sutures were passed through the bone block and tied to secure it to the proximal patellar pole. The distal quadriceps tendon sutures and the Achilles tendon graft sutures were then passed through the patellar drill holes and retrieved through small slits in the patellar tendon. The sutures were tensioned and tied, securing the quadriceps tendon and Achilles tendon allograft to the proximal patellar pole. A locking whipstitch was placed in the distal end of the Achilles tendon graft. The graft was then passed through a 1- to 2-mm longitudinal incision in the intact proximal quadriceps tendon, sutured in place, and then flipped distally. The graft was sutured to the native quadriceps tendon and the patella using interrupted sutures, creating a doubled Achilles tendon allograft reconstruction (Figure 6). 10
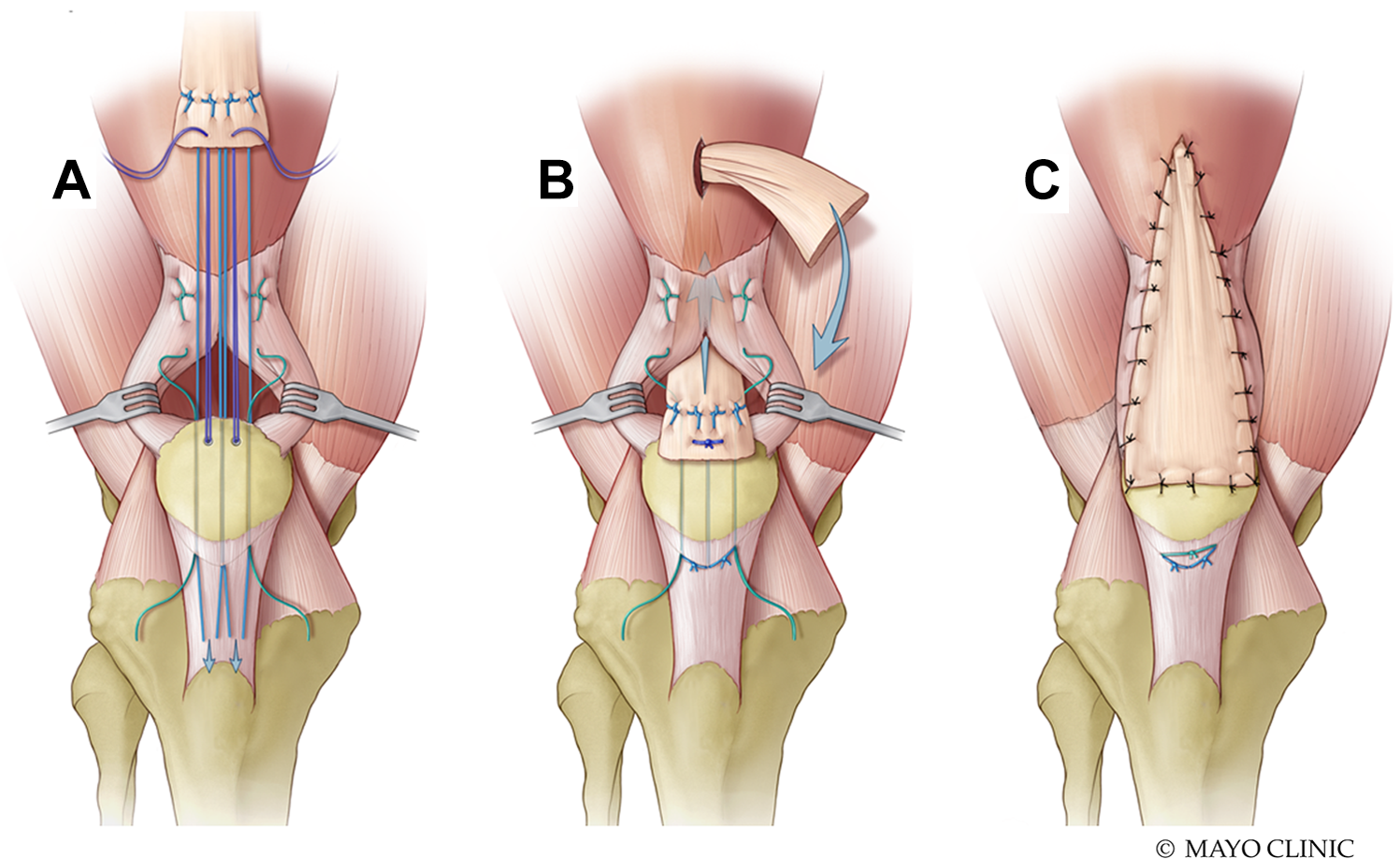
Quadriceps tendon reconstruction using Achilles tendon allograft. (A) Proximal patella with 3 parallel, longitudinal patellar drill holes, 2 suture anchors, and a locking whipstitch in the native quadriceps tendon. (B) Suture anchors are passed through the bone block to secure it at the proximal patella. Allograft and native quadriceps tendon sutures are passed through the patellar drill holes. Allograft is passed through a midline slit in the intact proximal quadriceps tendon and sutured in place. (C) Allograft is flipped distally and sutured to native quadriceps tendon and patella, creating doubled Achilles tendon allograft reconstruction.
Postoperative Rehabilitation
The operative leg was placed in a hinged rehabilitation brace locked in full extension. Progression of the therapy program was individualized according to patient age, comorbidities, preinjury activity level, and intraoperative assessment of the construct strength. Patients were typically instructed to wear the brace at all times except for showering, to bear partial weight using crutches, and to perform quadriceps sets/straight-leg lifts with the brace locked. They were encouraged to unlock the brace for active flexion/passive extension to 30° maximum. At 3 weeks postoperatively, patients progressed to weightbearing as tolerated with the brace locked in extension, and active flexion/passive extension was increased to 60° maximum. At 6 weeks postoperatively, patients were weaned from gait aids, knee motion was progressed to 90°, and straight-leg lifts were performed with the brace unlocked. At 9 weeks postoperatively, the brace was worn only when walking, full knee motion was allowed, and closed-chain resistance exercises were begun. Patients continued progressive resistance quadriceps strengthening until they returned to their prior level of activity.
Statistical Analysis
The pre- and postoperative IKDC and Tegner activity scores were compared within each surgical technique using the Wilcoxon signed rank test. A subgroup analysis of each surgical technique compared postoperative outcome scores between patellar and quadriceps tendon ruptures using the Wilcoxon rank sum test. Characteristics were compared between patellar tendon and quadriceps tendon ruptures using the chi-square test for nominal variables and the Wilcoxon rank sum test for continuous variables. Statistical significance was set at P < .05. Statistical analysis was performed using JMP (Version 13.0; SAS Institute).
Results
Included in this study were 43 patellar or quadriceps tendon ruptures treated surgically in 40 patients, including 3 patients with bilateral ruptures. The surgical technique included 17 (39.5%) primary extensor mechanism repairs, 13 (30.2%) repairs using semitendinosus autograft augmentation, and 13 (30.2%) reconstructions using an Achilles tendon allograft. The patellar tendon was involved in 22 cases; the quadriceps tendon, in 21 cases. Thirty-three (82.5%) patients were male, including all 3 patients with bilateral ruptures (Table 1). The average age at the time of surgery was 48.1 years (range, 17.3-90.7 years). The most common comorbidity in our cohort was obesity, with 55% of patients with a body mass index (BMI) >30. The average BMI was 31 (range, 19.7-53.3). Age was the only significant characteristic difference between patients with patellar and quadriceps tendon ruptures, with mean age of 36.4 years for patellar tendon cases and 60.4 years for quadriceps tendon cases (P < .001). Seventeen (39.5%) cases had at least 1 prior extensor mechanism surgery performed at an outside facility. Failed previous surgery was noted in 1 patient with primary repair, 3 patients with repair using semitendinosus augmentation, and 13 patients with reconstruction using Achilles tendon allograft. The average follow-up was 3.88 years (range, 1-15.63 years).
Characteristics of Knee Extensor Mechanism Injuries a
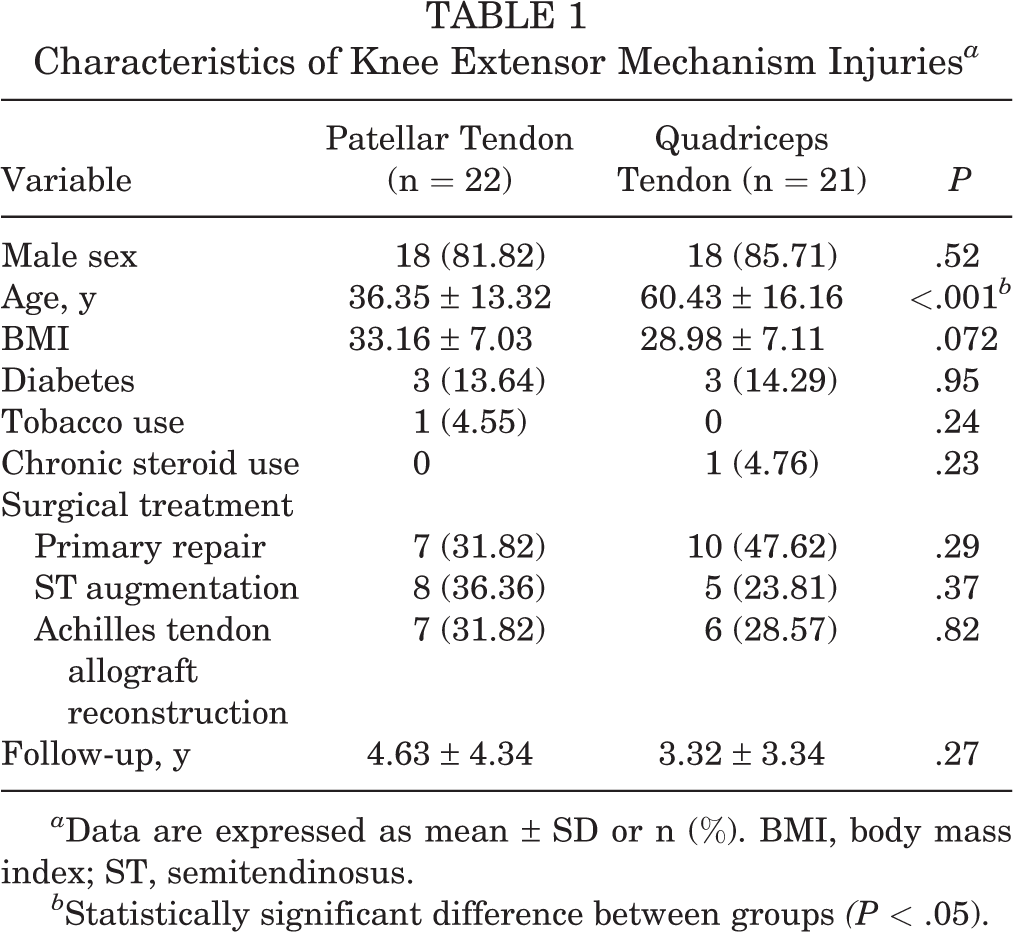
a Data are expressed as mean ± SD or n (%). BMI, body mass index; ST, semitendinosus.
b Statistically significant difference between groups (P < .05).
Extensor mechanism lag >5° was measured in 4 (9.3%) cases at the last follow-up (1 patellar tendon repair using autograft augmentation, 3 quadriceps tendon reconstructions using Achilles tendon allograft). All patients were able to achieve knee flexion >90°. Postoperative IKDC scores were significantly improved for all surgical methods (P < .005), and postoperative Tegner activity scores were significantly improved in patients who underwent primary repair and reconstruction using allograft (P < .05) (Table 2). Average pre- and postoperative Caton-Deschamps Indices are listed in Table 3. Patellar tendon ruptures often presented with patella alta on radiographs (n = 18, 81.8%), which improved to normal patellar height after surgery in the majority of cases (n = 18, 81.8%). Conversely, 95.2% (n = 20) of quadriceps tendon cases treated with repair and reconstruction had a normal patellar height on presenting radiographs, and 81% (n = 17) of cases had a normal patellar height on postoperative radiographs.
Outcomes of Knee Extensor Mechanism Surgeries a

a Data are expressed as mean ± SD unless otherwise indicated. IKDC, International Knee Documentation Committee.
b Statistically significant difference.
Caton-Deschamps Index a

a Data are expressed as mean ± SD unless otherwise indicated. PT, patellar tendon; QT, quadriceps tendon.
No patients in the primary repair cohort had an extensor lag at the last follow-up. Postoperative IKDC and Tegner activity scores improved by an average of 27% and 2.2 points, respectively (P < .001). There was no difference when comparing primary repair of patellar and quadriceps tendons according to postoperative IKDC or Tegner activity scores. No complications occurred in the primary extensor mechanism repair cohort.
One patient had a 10° extensor mechanism lag after patellar tendon repair using semitendinosus autograft augmentation. This patient had 2 failed prior patellar tendon repairs performed at an outside facility. This patient reported overall satisfaction with their functional outcome despite the persistent extensor mechanism lag. No patients treated with quadriceps tendon repair using semitendinosus autograft augmentation had an extensor mechanism lag at the last follow-up. All patients (both patellar and quadriceps tendon rupture groups) treated with semitendinosus autograft augmentation had significant improvement in postoperative IKDC scores, with a mean increase of 22.7% (P = .003). Tegner activity scores improved by a mean of 1.5 points, but this did not reach statistical significance (P = .058). There was no difference in postoperative IKDC and Tegner activity scores between patellar and quadriceps tendons repaired using semitendinosus augmentation (P > .2).
Three (50%) patients treated with quadriceps reconstruction using Achilles tendon allograft had a persistent extensor lag (mean, 23.3°; range, 10-30°) at the last follow-up. These 3 patients had 2 prior attempts at quadriceps tendon repair performed at outside facilities and had improvement in their postoperative IKDC scores by a mean of 13.9% despite a persistent extensor mechanism lag after surgery. No patients with patellar tendon reconstruction using Achilles tendon allograft had a persistent extensor mechanism lag at the last follow-up. All patients (both patellar and quadriceps tendon rupture groups) treated with Achilles tendon allograft reconstruction improved their mean IKDC scores by 23.7% (P = .0002), and the Tegner activity scores improved by 1.23 points (P = .003). There were no differences in postoperative IKDC or Tegner activity scores when comparing between quadriceps and patellar tendon reconstructions.
Reoperations
One patient returned to the operating room approximately 11 months postoperatively for irrigation and debridement for Staphylococcus epidermidis septic arthritis, and the extensor mechanism remained intact during and after this procedure. A second patient developed an acute deep venous thrombosis approximately 1 week after surgery and was diagnosed with factor V Leiden thrombophilia. This same patient went on to develop Parsonage-Turner syndrome affecting the left upper extremity approximately 2 weeks postoperatively, which resolved over the following year. No patient required further extensor mechanism surgery.
Discussion
This study presented a strategy for restoring continuity of the extensor mechanism after patellar or quadriceps tendon disruption using 3 approaches: (1) patients with first-time ruptures and good tissue quality were treated with primary patellar tendon or quadriceps tendon repair; (2) patients with significant tendinopathy or mild tissue loss were treated with repair and quadrupled semitendinosus autograft augmentation; and (3) patients with significant tissue loss or failed prior repair or reconstruction attempts were treated with reconstruction using a doubled Achilles tendon allograft. Choice of surgical technique was based on preoperative MRI scans, patient factors such as history of prior extensor mechanism surgery, and intraoperative findings. Patients were informed of all 3 treatment options, and the final surgical decision was based on the surgeon’s intraoperative judgment. While 9.3% of cases had a persistent extensor lag >5° after surgery, no patients required further surgery to their extensor mechanism, and postoperative IKDC scores were significantly improved after all surgical techniques in this cohort. Our results mirror those of Gilmore et al 6 in a review of patellar tendon ruptures. In their series, primary repair of acute patellar tendon ruptures, defined as repair within 2 weeks of injury with adequate tissue, had the best outcomes and a 2% reoperation rate. 6 The most common surgical procedure for chronic patellar ruptures, defined as surgery >2 weeks after injury or poor tissue quality, utilized autogenous graft reconstruction with various tendons, and no reruptures were reported. 6
A recent study 20 demonstrated a decrease in rerupture rate using suture anchors compared with transosseous sutures. We prefer to use both suture anchors and transosseous sutures for dual fixation, which, in our opinion, creates a stronger construct and decreases micromotion. While the rare complication of patellar stress fracture has been described after transosseous extensor mechanism repair, 7 none of our patients developed patellar cystic changes, osteolysis, or a patellar fracture.
Our patients treated with primary extensor mechanism repair and a novel semitendinosus autograft augmentation technique using a distal or proximal patellar pole socket had significantly improved postoperative outcomes without an associated increase in complications. None of our patients sustained a patellar fracture or required removal of the TightRope metallic button. These results are similar to those of multiple studies 1,15,26 that have demonstrated significantly improved outcomes after chronic patellar tendon repair using hamstring tendon autograft augmentation. Hamstring tendon autografts more closely match the biomechanical properties of the native extensor mechanism and decrease strain across the repair site when compared with primary suture repair. 2,16,18,29 Semitendinosus autografts are strong 18 and routinely harvested during anterior cruciate ligament reconstruction, making their use a reliable option. 15,16 While studies have shown biomechanical superiority using synthetic material as an internal brace compared with suture repair alone, 23 we prefer to augment the repair with autogenic tendon tissue to improve the initial biomechanical strength and restore the deficient collagen. In addition, the extensor mechanism strength is enhanced with the quadrupled tendon technique, allowing earlier range of motion and weightbearing compared with primary repair alone. 2,4,16,18,21,29 The use of semitendinosus autograft augmentation has been advocated for chronic extensor mechanism ruptures or failed attempted primary repairs if mild tendon retraction is observed, 1,15,16,21,26 coinciding with our preferred treatment algorithm.
Chronic extensor mechanism ruptures with poor native tissue, significant tendon retraction, or failed prior repair attempts pose additional treatment challenges. A deficient, scarred, and retracted tendon creates a gap that precludes adequate reapproximation. 8,17 We prefer a reconstruction technique using a doubled Achilles tendon allograft in these patients. Our cohort review showed significantly improved postoperative outcomes scores but demonstrated a higher incidence (23%) of persistent extension lag. These findings are somewhat better than those in the series published by Karas et al, 10 who noted a 33% incidence of persistent extensor lag after extensor mechanism allograft reconstruction. Patients were able to achieve pain relief, return to activities of daily living, and maintain knee range of motion at the final follow-up, although overall satisfaction rates were mild to moderate. 10 Similar functional outcomes were noted in a case series by Murgier et al, 19 although no patients in this series had a persistent extensor mechanism lag at the final follow-up. While excluded from this study, allograft extensor mechanism reconstruction in the setting of total knee arthroplasty poses additional challenges in management, with a reported 38% failure rate by Brown et al. 3
Our cohort was similar to that of Siwek and Rao in that patients with patellar tendon ruptures were significantly younger than patients with quadriceps tendon ruptures. 24 However, no difference in postoperative outcomes was discovered when comparing patellar and quadriceps tendon ruptures treated with primary repair, semitendinosus augmentation, or Achilles tendon allograft reconstruction. A difference in postoperative Caton-Deschamps Index was measured between patellar tendon and quadriceps tendon procedures, as expected given the direction of patellar displacement when the quadriceps or patellar tendon is deficient. To our knowledge, no studies have compared outcomes between patellar and quadriceps tendon ruptures.
Limitations in this study include its retrospective nature and limited power to detect differences in outcomes on subgroup analysis given the small sample size. In addition, a long study period was required to maximize patient numbers, which may have altered clinical outcomes since postoperative rehabilitation protocols changed over the 2 decades. Postoperative protocols progressed to earlier range of motion, weightbearing, and strengthening as confidence improved with the semitendinosus augmentation procedure. Furthermore, surgical techniques evolved during this time frame, which may have altered postoperative clinical outcomes. However, this long study period allowed for further development of a treatment algorithm in this relatively uncommon condition. Additional limitations in this study include the short 1-year postoperative follow-up for inclusion in this study, which may have missed late surgical failures. Although postoperative radiographs were obtained to assess Caton-Deschamps Indices, MRI was not performed to be able to assess healing of the restored extensor mechanism. Lastly, extensor mechanism lag was assessed without the use of a goniometer, and no objective strength testing was performed beyond manual muscle testing; however, all physical examinations were performed by the same, experienced operating surgeon.
Conclusion
Our strategy for treatment of patellar and quadriceps tendon rupture was based on native tissue quality, chronicity of the extensor mechanism disruption, and history of prior surgery. Primary repair alone, repair using semitendinosus tendon autograft augmentation, and reconstruction using Achilles tendon allograft were all effective methods to restore extensor mechanism and knee function with the proper indications. Persistent knee extensor lag was more common in chronic extensor mechanism injuries requiring revision surgery, although patients still reported significantly improved postoperative functional outcomes.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: M.J.S. and A.J.K. received support from the Quattrone-Foderaro Musculoskeletal-Orthopaedic Surgery Research Innovation Fund and the National Institute of Arthritis and Musculoskeletal and Skin Diseases for the Musculoskeletal Research Training Program (T32AR56950). C.R.C.S. has received hospitality payments from Stryker. M.D.L. has a family member with the following disclosures: research support from Smith & Nephew; consulting fees from Arthrex, Linvatec, Ossur, and Smith & Nephew; speaking fees from Smith & Nephew; and royalties from Arthrex, Smith & Nephew, and Thieme. A.J.K. has received research support from Ceterix and Gemini Medical, consulting fees from Arthrex and MTF, speaking fees from MTF, and honoraria from MTF. M.J.S. has received research support from Stryker and consulting fees and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Final revision submitted May 20, 2021; accepted June 23, 2021.
The contents of this study are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health. Ethical approval for this study was obtained from Mayo Clinic (application No. 15-000601).