
Abstract
Background:
Preoperative opioid use has been shown to be a negative predictor of patient outcomes, complication rates, and resource utilization in a variety of different orthopaedic procedures. To date, there are no studies investigating its effect on outcomes after hip arthroscopy in the setting of femoroacetabular impingement (FAI).
Purpose:
To determine the association of preoperative opioid use with postoperative outcomes after hip arthroscopy in patients with FAI.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The Truven Health MarketScan Commercial Claims and Encounters Database was queried for all patients who underwent hip arthroscopy for FAI between 2011 and 2018. Opioid prescriptions filled in the 6 months preceding surgery were queried, and the average daily oral morphine equivalents (OMEs) in this period were computed for each patient. Patients were divided into 4 cohorts: opioid naïve, <1 OME per day, 1 to 5 OMEs per day, and >5 OMEs per day. Postoperative 90-day complications, health care utilization, perioperative costs, postoperative opioid use, and 1- and 3-year revision rates were then compared among cohorts.
Results:
A total of 22,124 patients were ultimately included in this study; 31.2% of these patients were prescribed opioids preoperatively. Overall, the percentage of preoperative opioid-naïve patients increased from 64.5% in 2011 to 78.9% in 2018. Patients who received preoperative opioids had a higher rate of complications, increased resource utilization, and increased revision rates. Specifically, on multivariate analysis, patients taking >5 OMEs per day (compared with patients who were preoperatively opioid naïve) had increased odds of a postoperative emergency department visit (Odds Ratio, 2.23; 95% confidence interval [CI], 1.94-2.56; P < .001), 90-day readmission (OR, 2.25; 95% CI, 1.77-2.87; P < .001), increased acute postoperative opioid use (OR, 25.56; 95% CI, 22.98-28.43; P < .001), prolonged opioid use (OR, 10.45; 95% CI, 8.92-12.25; P < .001), and 3-year revision surgery (OR, 2.14; 95% CI, 1.36-3.36; P < .001). Perioperative adjusted costs were increased for all preoperative opioid users and were highest for the >5 OMEs per day cohort ($6255; 95% CI, $5143-$7368).
Conclusion:
A large number of patients with FAI are prescribed opioids before undergoing hip arthroscopy, and use of these pain medications is associated with increased health care utilization, increased costs, prolonged opioid use, and early revision surgery.
Keywords
Femoroacetabular impingement (FAI), a result of an anatomic abnormality of the femoral head, the acetabulum, or both, 43 is present in 10% to 15% of the general adult population. 30 The condition is often diagnosed in young men, particularly those participating in athletic activities, and represents a common generator of hip pain in the young adult population. 29 While nonoperative management remains the mainstay of treatment for FAI, 56,60 surgical options are considered when these options fail. While open operative treatments are the historic standard, hip arthroscopy is gaining popularity, 65 and outcomes have been shown to be favorable when compared with nonoperative management. 20 As this operation gains popularity, it is important to identify potentially modifiable risk factors for poor patient and health care utilization outcomes. One such risk factor is preoperative opioid use.
Nonmedical use of prescription opioids in the United States has increased >3-fold in the past 30 years, 24,32 and the opioid epidemic has been declared a public health emergency. 23 Soaring rates of opioid misuse have resulted in exponential increases in opioid-related deaths, and it is now the leading cause of death for Americans <50 years of age. 47 Despite recommendations against the practice, 7 many patients with chronic pain continue to be prescribed opioids—a concerning trend given studies showing that patients abuse or misuse the medications 32% to 40% of the time. 11 Perhaps not surprisingly, rates of preoperative opioid use are reportedly on the rise in orthopaedic surgery. 61
While opioids are not a recommended component of the nonoperative management of FAI, up to 45% of patients evaluated for hip arthroscopy for FAI have been prescribed preoperative opioids. 60 This is problematic, as multiple studies have demonstrated that these patients—relative to their opioid-naïve counterparts—are more likely to be subject to increased postoperative pain, 11 postoperative opioid utilization, 8 –10,12 complications, 3,26,61,64 and health care utilization 34,61 after various elective orthopaedic procedures. However, the relationship between preoperative opioid use and outcomes after hip arthroscopy for FAI remains unknown. Given the high percentage of patients receiving preoperative opioids, this is a critical relationship to define.
The purpose of this study was to determine the association of opioid use before hip arthroscopy with postoperative outcomes, surgical survivorship, prolonged narcotic demand, and health care resource utilization in patients with FAI. We hypothesized that preoperative opioid use would be a dose-dependent risk factor for increased postoperative complications and narcotic requirements, secondary surgery, increased perioperative costs, and increased health care utilization in this patient population.
Methods
Data Source
This was a retrospective cohort study utilizing the Truven Health MarketScan Commercial Claims and Encounters Database. The Truven database includes privately insured patients as well as those who have Medicare with a private supplement and records claims related to inpatient and outpatient services and pharmaceutical prescriptions. It also allows for longitudinal follow-up of continually enrolled patients. This database has been used extensively in health services and clinical outcomes research. 54,58,62
Patient Selection
The Truven database was queried for patients who underwent hip arthroscopy for FAI between 2011 and 2018. We used the following Current Procedural Terminology (CPT) codes: 29914 (arthroscopy, hip, surgical; with femoroplasty), 29915 (arthroscopy, hip, surgical; with acetabuloplasty), and 29916 (arthroscopy, hip, surgical; with labral repair). These CPT codes were first added in 2011, and for this reason, 2011 was the chosen start year for this study. Patients without continuous insurance enrollment in the 6 months preceding surgery and the 90 days after surgery were excluded from analysis. Additionally, 2 other subgroups were created using 1-year and 3-year continuous insurance enrollment for the tracking of longer-term secondary surgery. This resulted in 22,124, 8463, and 2628 patients with data available for 90 days, 1 year, and 3 years, respectively.
Preoperative Patient Data and Preoperative Opioid Cohorts
Baseline patient characteristic, comorbid, and medication data were collected for 6 months preceding surgery. The number of patient comorbidities was collected using the Elixhauser comorbidity index 14 and categorized as 0, 1, or ≥2. Patient smoking status and drug and alcohol use disorders were queried given their potential association with preoperative opioid use and postoperative outcomes. Opioid prescriptions were queried for the 6-month preoperative period. These were identified using National Drug Codes (NDCs; US Food and Drug Administration). NDCs have been used previously to successfully collect and track opioid medication in US Food and Drug Administration claims databases. 6,63 Opioid conversion tables were then used to determine oral morphine equivalents (OMEs). Next, average daily OMEs were calculated for each patient by dividing the total OMEs prescribed in the preoperative period by the length of the preoperative period (180 days). The following cohorts were then created based on preoperative daily OME averages: (1) opioid naïve (ie, no opioid prescriptions in the 6 months before surgery), (2) <1 OME per day, (3) 1 to 5 OMEs per day, and (4) >5 OMEs per day. These cutoffs were selected in order to capture a diverse set of preoperative opioid dosing strategies, and they are similar to those previously reported in the literature. 17
Postoperative Outcomes
The following rates of 90-day outcomes were collected: readmission, all-cause emergency department (ED) visit, pain-related ED visit, pneumonia, myocardial infarction, thromboembolic event, cerebrovascular accident (ie, stroke), and postoperative opioid use (≥2 postoperative opioid refills in the 90-day postoperative period). Medical complications (stroke, myocardial infarction, thromboembolic event, pneumonia) were analyzed as a categorical group given the relative rarity of these complications in the hip arthroscopy cohort. Secondary surgery was analyzed at 1 and 3 years postoperatively in a subgroup of patients with this longer-term follow-up available. Secondary surgery was defined as a patient undergoing a revision hip arthroscopy or total hip arthroplasty (THA) on the ipsilateral extremity within 1 or 3 years. Patients without recorded CPT laterality modifiers were excluded when tracking revision rates. Additionally, at 1-year postoperatively, prolonged opioid use was examined and was defined as ≥2 opioid prescriptions received in the 6- to 12-month postoperative period. The issuing of prescriptions during a specified postoperative period was used to define prolonged opioid use (rather than by an opioid quantity), as previously reported in the literature. 18
In addition, we collected cost data for the 6-month preoperative and 90-day postoperative period. We defined costs as the sum of net health care costs plus any deductibles, copays, or coinsurance in the 6 months before and 3 months after hip arthroscopy. This cost analysis was derived from prior investigations of hip arthroscopy for FAI. 25
Statistical Analysis
Baseline characteristics, comorbidities, and postoperative complications were compared using chi-square analysis. Binomial logistic regression was then performed to compare preoperative opioid-use groups to the opioid-naïve cohort, controlling for baseline characteristic and comorbid patient data. Two-sample t tests and a generalized linear model with gamma distribution and a logarithmic link function were used to compare total health care costs between cohorts. Temporal trends of preoperative opioid use between 2011 and 2018 were also assessed. Statistical analysis in this study was performed using SAS Version 9.4 (SAS) statistical software. We defined statistical significance as P < .05.
Results
Baseline Characteristics
There were 22,124 patients who met inclusion criteria, of whom 68.8% were opioid naïve in the 6-month preoperative period. The percentage of patients who were opioid naïve changed over the study period (Figure 1). Moreover, 31.2% of patients received preoperative opioids—specifically, 7.2%, 12.7%, and 11.3% of patients received <1, 1 to 5, and >5 OMEs per day, respectively (Table 1). The majority (65.0%) of patients were women and >45 years of age (31.9%). Baseline differences between cohorts were found in patient age, sex, Elixhauser comorbidity index, smoking status, and drug/alcohol use disorders (Table 1).

Trends in preoperative opioid use in patients undergoing hip arthroscopy for femoroacetabular impingement, 2011-2018. In general, an increase in the proportion of opioid-naïve patients and a decrease in opioid-use patients was observed over the study period. OMEs, oral morphine equivalents.
Characteristics and Comorbidities of the Study Groups a

a Data are reported as n (% of each group). P values indicate a statistically significant difference among any 2 of the groups (P < .05). OME, oral morphine equivalent.
Postoperative Health Care Utilization and Medical Complications
Univariate analysis was conducted, demonstrating that 90-day all-cause (opioid naïve vs >5 OMEs cohort; 6.3% vs 15%; P < .001) and pain-related (0.28% vs 1.04%; P < .001) ED visits were greater in the preoperative opioid-use cohorts. Similarly, 30-day (1.1% vs 2.2%; P < .001) and 90-day (1.6% vs 4.8%; P < .001) readmissions were more common in this group. These associations were generally dose-dependent and most pronounced in patients taking >5 OMEs daily (Table 2).
Univariate Analysis of Postoperative Complications in the Study Groups a

a Data are reported as n (% of each group). P values indicate a statistically significant difference among any 2 of the groups (P < .05). ED, emergency department; OME, oral morphine equivalent.
Multivariate analysis demonstrated preservation of these findings even when controlling for baseline patient characteristic and comorbid information (Table 3). All 3 preoperative opioid cohorts had higher odds of a 90-day ED visit, 90-day readmission, and the need for ≥2 opioid refills. Of note, on multivariate analysis, the >5 OME cohort was additionally associated with higher odds of ED visits related to pain (Odds Ratio, 3.31; 95% confidence interval [CI], 1.91-5.73; P
Adjusted Odds of 90-Day Complications, Opioid-Naïve vs Opioid-Use Groups a

a Bolded P values indicate a statistically significant difference compared with the opioid-naïve condition (P < .05). ED, emergency department; OME, oral morphine equivalent; OR, odds ratio.
On univariate cost analysis, median cost of care was highest in those consuming >5 OMEs daily at $24,744 (interquartile range, $16,841-$37,034). Adjusted cost differences demonstrated a dose-dependent relationship with preoperative opioid use and when compared with opioid-naïve patients: $1555 (95% CI, $279-$2832; P = .008), $3334 (95% CI, $2328-$4358; P < .001), and $6255 (95% CI, $5143-$7368; P < .001) in the <1, 1-5, and >5 OME use groups, respectively (Table 4).
Univariate and Multivariate Analyses of Perioperative Cost a

a Costs are reported in inflation-adjusted US dollars based on the Consumer Price Index from the Federal Reserve Bank in 2015. P values indicate a statistically significant difference compared with the opioid-naïve condition (P < .05). IQR, interquartile range; OME, oral morphine equivalent; -, not applicable.
Last, 90-day postoperative medical complications were uncommon after hip arthroscopy, and no differences were found in medical complications among cohorts on multivariate analysis.
Secondary Surgery and Postoperative Opioid Use
Revision arthroscopy and conversion to THA were analyzed at 1 and 3 years postoperatively. A total of 8463 patients and 2628 patients were included for analysis at 1 year and 3 years, respectively. The unadjusted 1-year revision hip arthroscopy rate followed a dose-dependent trend, from 2.3% in opioid-naïve patients to 4.8% in those taking >5 OMEs daily. Likewise, 3-year revision surgery rates also increased from 5.5% to 9.6% (Table 5). Multivariate analysis confirmed these findings. At 3 years, there was a 70% increased odds of revision in those taking 1 to 5 OMEs (OR, 1.70; 95% CI, 1.09-2.66; P = .019) and a 114% increased odds in those taking >5 OMEs daily preoperatively (OR, 2.14; 95% CI, 1.36-3.36; P < .001) (Table 5).
Analysis of 1-Year and 3-Year Revision Surgery and THA Rates, Opioid-Naïve vs Opioid-Use Groups a
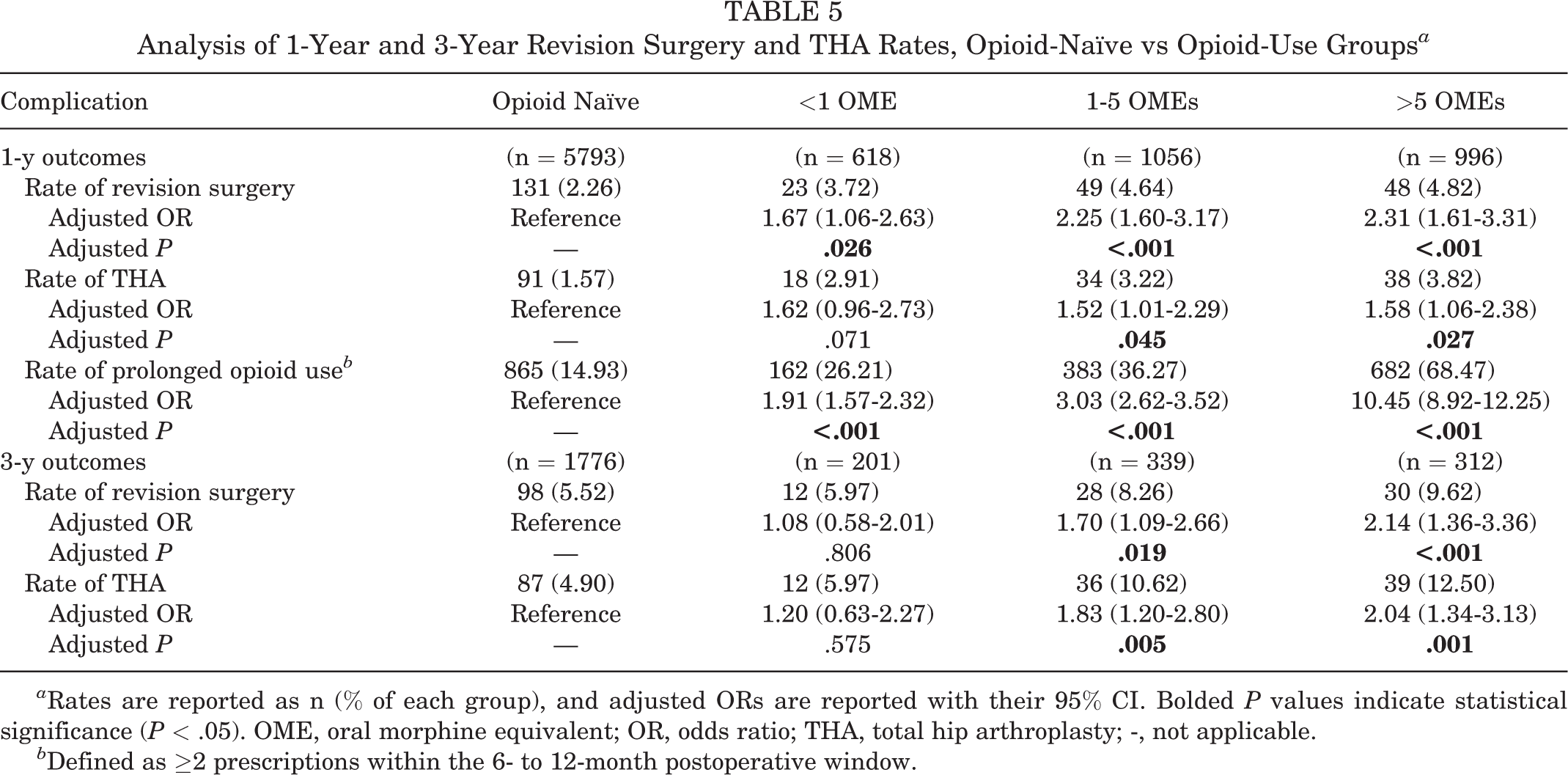
a Rates are reported as n (% of each group), and adjusted ORs are reported with their 95% CI. Bolded P values indicate statistical significance (P < .05). OME, oral morphine equivalent; OR, odds ratio; THA, total hip arthroplasty; -, not applicable.
b Defined as ≥2 prescriptions within the 6- to 12-month postoperative window.
Similarly, rates of THA after arthroscopy increased with opioid use in a dose-dependent fashion. On multivariate analysis, patients prescribed ≥1 OME daily had a significant increase in both 1-year and 3-year rates of THA. At 3 years, patients had an 83% increased odds of THA if prescribed 1 to 5 OMEs daily (OR, 1.83; 95% CI, 1.20-2.80; P = .005) and a 104% increased odds if prescribed >5 OMEs daily (OR, 2.04; 95% CI, 1.34-3.13; P = .001) (Table 5).
Prolonged opioid use was additionally examined at 1 year postoperatively. When compared with opioid-naïve patients, those taking >5 OMEs daily preoperatively had >10 times the odds of prolonged postoperative opioid use (OR, 10.45; 95% CI, 8.92-12.25; P < .001), and 68.5% of patients in this cohort had prolonged opioid use (Table 5). Of note, prolonged opioid use was also common in the previously opioid-naïve patients (14.9%).
Trends in Preoperative Opioid Use in Patients With FAI Undergoing Hip Arthroscopy
The proportion of opioid-naïve patients increased steadily from 64.5% to 72.2% between the years 2011 and 2017. By the year 2018, 78.9% of patients were not consuming any opioids before undergoing surgical management. Furthermore, a steady decline in the proportion of opioid-consuming patients was observed, with percentage of patients in the >5 OME group decreasing from a maximum of 12.9% in 2011 to a minimum of 6.5% in 2018 (Figure 1).
Discussion
The results of this study demonstrated that opioid use before hip arthroscopy is associated with increased health care utilization, secondary surgery, and prolonged postoperative opioid use in a dose-dependent manner. We found that preoperative opioid use is common in this group of patients and is associated with outcome inferiority in all measured domains. Preoperative opioid use was seen in >30% of patients, with 11.3% averaging >5 OMEs per day before surgery. These patients had greater 90-day health care utilization, including ED visits and hospital admissions, as well as significantly increased rates of secondary surgery at 1 and 3 years. Not surprisingly, adjusted perioperative costs were significantly higher for patients receiving preoperative opioids. Preoperative opioid use was also associated with increased postoperative opioid needs and with a sobering rate of prolonged postoperative opioid use. Examined complications were nearly universally associated with preoperative opioid use in a dose-dependent manner. No association was found between preoperative opioid use and postoperative medical complications. Fortunately, we found that over the study period, preoperative opioid use before hip arthroscopy was decreasing.
Our results suggested that preoperative opioid use may be associated with worsened perioperative pain and may lead to subsequent need for medical care. This relationship has been observed in open procedures such as hip and knee arthroplasty, as well as arthroscopic rotator cuff repair, where preoperative opioid use was associated with increases in postoperative complication rates, 4,6,17,26,38,45 postoperative narcotic consumption, 45 readmission, 6,26,58 revision, 5,17,26,52,58 costs, 6,17 and patient dissatisfaction. 19,51 The reasons for our findings are likely multifaceted and probably involve both physiologic and psychosocial factors. Physiologically, because opioid use potentiates the activity of nociceptive pain receptors and paradoxically induces hyperalgesia, 35,50 patients with a history of opioid use are more prone to poor perioperative pain control. This relationship likely contributed to both the increased and prolonged postoperative opioid use in our cohort. This may also be a significant driver of increased postoperative hospitalizations, ED visits, and need for early secondary surgery. The relationship between opioids and psychosocial aspects of health is also complex. Evidence has suggested that opioid use may result in unrealistic expectations about pain management after surgery 37 and may aggravate the anxiety associated with painful stimuli. 53 Perhaps, then, it is not surprising that a relationship with opioid misuse exists between both active cigarette smoking and drug/alcohol abuse syndromes. 15,66 Additionally, patients receiving preoperative opioids may be more likely to experience dissatisfaction after surgery and lower patient-reported outcome measures (PROMs). While PROMs could not be analyzed in this study, prior work by Westermann et al 60 found that patients with FAI with preoperative opioid use reported lower PROMs and overall decreased hip function after arthroscopic management.
We also found that increased preoperative opioid consumption is associated with the need for early secondary surgery. These findings are similar to those reported after other orthopaedic procedures. 5,26,27,52,58,61 The reasons for this association may again be related to physiologic alterations associated with opioid use. This class of medication is known to impair platelet aggregation, 22,44 the immune response, 36,39,57 and wound healing. 41,49 However, nonphysiologic mechanisms are likely the predominant driver of arthroscopy survivorship. Surgical indications for arthroscopic treatment of FAI are, in part, pain-dependent, and dissatisfied patients who report unsatisfactory pain relief are pragmatically more likely to seek further surgical treatment. While prior work examined risk factors for revision hip arthroscopy, preoperative opioid use was not examined. 59 Our overall reported revision rates of 3.0% at 1 year and 6.4% at 3 years are comparable to those reported by previous authors. 55,59 Additionally, previous research has investigated survivorship of hip arthroscopy and risk factors for conversion to THA. 48 Our overall reported conversion rates of 2.1% and 6.6% at 1 year and 3 years, respectively, were lower than those reported by previous authors, which ranged from 12% to 20%, but these studies were performed in older patient cohorts that likely had a lower threshold for conversion. 40,48 For instance, in our study, 68.1% of patients were aged <45 years, whereas these prior studies focused more on the older patient, in whom chronologic age has been deemed an independent risk factor for failure of hip arthroscopy. 21
In addition to clinical outcomes, our findings suggested dose-related preoperative opioid use is increasingly associated with greater perioperative health care utilization, which mirrors findings in the arthroplasty population. 6 In our population, even patients receiving on average <1 OME daily preoperatively had increased rates of ED visits and readmission and incurred significantly increased costs relative to opioid-naïve patients. Importantly, in those patients receiving >5 OMEs daily preoperatively, peri-operative adjusted costs were >$6000 greater than those of opioid-naïve patients. This cost relationship is likely explained in large part by our other findings of increased ED visits, need for readmission, and secondary surgery. A similar cost relationship has been demonstrated after spine procedures, 28,33 lower extremity arthroplasty, 61 and shoulder arthroplasty. 6 Thus, it is likely that preoperative opioid use should be considered when calculating preoperative risk of high longitudinal costs of care.
Fortunately, this study demonstrates an encouraging trend—the rate of preoperative opioid use in patients with FAI undergoing hip arthroscopy appears to be decreasing. Throughout our 8-year study period, we found that an average of ∼69% of patients were opioid naïve before hip arthroscopy, and that between 2011 and 2018 there was a ∼15% increase in the proportion of those not using opioids preoperatively for pain management. This is contrary to the findings of Westermann et al 60 in 2018, and likely is a result of the contemporary cohort included in this study. Our study period coexists with an epidemic-driven paradigm shift away from narcotic prescribing practices. These trends may also stem from the creation of bodies such as prescription drug monitoring programs 2 and legislation permitting increased scrutiny of prescription patterns by licensing agencies, law enforcement officials, and health care institutions. 42 Additionally, this reduction in the rate of preoperative opioid utilization also likely reflects the progress of initiatives at the federal and institutional levels to avoid opioids as a long-term strategy for pain management. 13,31 As a result, several studies have supported preoperative opioid education in curbing excess opioid utilization. 1,16,46 However, the general prevalence of opioid use before hip arthroscopy is extremely high relative to its arthritis counterparts and may reflect a poor understanding of the role of FAI as a generator of chronic hip pain in the young patient. Given that the most common prescriber of opioids is not an orthopaedist, it is feasible that the opioid prescriber is simply unaware of the subspecialty surgical treatment options and is aiming to temporize the poorly understood hip pain. However, as the orthopaedist’s understanding of FAI continues to improve, so must the education of referring providers, as avoidance of opioids clearly has the potential for a positive effect on the natural history of a surgically treated hip with FAI.
Limitations
While there are many strengths to the current study, it is obviously not without limitations, and these should be considered when interpreting the results. As this analysis utilized a claims database, accurate results hinged on proper coding for all preoperative and postoperative events. Along the same lines, we excluded patients with missing laterality modifiers from the analysis of reoperation or revision procedures. It is possible that this led to underreporting of revision and reoperation rates. Additionally, the Truven MarketScan database only includes data on insured patients; therefore, the generalizability of our results is limited by the absence of information on uninsured patients or those with Medicaid. Further, because this database does not include information on laboratory data, some comorbidities, surgical parameters, and patient-reported outcomes, this introduces potential uncontrolled confounding. Similarly, the characteristics of the study cohort, while reflective of what is being performed nationally, 25 should be considered. There was a strong female predominance, and a large number of patients aged >45 years. The potential exists that surgical indications were not always optimal, but this cannot be assessed using our study design. Another limitation is that OME groups were determined by averaging daily OMEs over a 180-day period. Although this is a reproducible, effective way to quantify opioid use, it does not eliminate the possibility of patients being inaccurately assigned into OME groups that do not reflect their true preoperative opioid consumption. Similarly, we cannot guarantee that filled prescriptions led to actual consumption by patients. Lastly, because patients in whom primary surgical management fails are more likely to have lasting pain after surgery, this may have contributed to rates of postoperative opioid use seen in this study. Similarly, these patients are more likely to undergo secondary surgery, representing a confounding effect on revision and THA rates seen in this cohort.
Conclusion
A large number of patients with FAI are prescribed opioids before undergoing hip arthroscopy, and use of these medications is associated with increased health care utilization, costs, prolonged opioid use, and early revision surgery. The results from this study should be used to inform both surgeons and referring physicians about the risks of opioid utilization for managing pain associated with FAI, guide initial efforts to wean narcotic use in patients preparing for surgery, and bring focus to longitudinal interdisciplinary efforts for opioid avoidance and early referral in patients with FAI.
Footnotes
Final revision submitted May 11, 2021; accepted June 9, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.X. has received consulting fees from Arthrex, My-Eye, and Trice Medical and nonconsulting fees and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.