
Abstract
Background:
There is limited literature evaluating patient-reported outcomes (PROs) in cigarette smokers undergoing hip arthroscopy for femoroacetabular impingement syndrome (FAIS) at midterm follow-up.
Purpose:
(1) To report minimum 5-year PROs for cigarette-smoking patients who underwent primary hip arthroscopy for FAIS and (2) to compare these results with a propensity-matched control group of never-smoking patients.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data were collected for all patients who underwent primary hip arthroscopy for FAIS between June 2009 and March 2016. Patients were eligible if they indicated that they smoked cigarettes within 1 month of surgery and had minimum 5-year postoperative outcomes for the modified Harris Hip Score, Nonarthritic Hip Score, Hip Outcome Score–Sport Specific Subscale (HOS-SSS), and International Hip Outcome Tool–12 (iHOT-12). The percentages of patients achieving the Patient Acceptable Symptom State (PASS) and maximum outcome improvement satisfaction threshold were recorded. The study group was then propensity matched in a 1:2 ratio to patients who had never smoked for comparison.
Results:
Included were 35 patients (35 hips) with a mean age of 39.4 ± 13.0 years and mean follow-up of 64.6 ± 4.1 months. These patients demonstrated significant improvement from preoperatively to a minimum 5-year follow-up for all recorded PROs (P < .05). When compared with 70 control patients (70 hips), smoking patients demonstrated significantly worse preoperative scores for all PROs (P < .05). Study patients also demonstrated worse minimum 5-year scores for all recorded PROs compared with control patients, which did not reach statistical significance but trended toward significance for HOS-SSS (70.4 vs 81.9; P = .076) and iHOT-12 (74.7 vs 82.2; P = .122). Smoking patients also trended toward lower rates of achieving PASS for the iHOT-12 compared with never-smoking patients (50.0% vs 68.2%; P = .120).
Conclusion:
Patients who smoked cigarettes and underwent primary hip arthroscopy for FAIS demonstrated significant improvement in PROs at a minimum 5-year follow-up. When compared with a propensity-matched control group of never-smokers, they trended toward lower postoperative HOS-SSS and iHOT-12 scores and lower rates of achieving PASS on the iHOT-12.
The influence of cigarette smoking has been well studied in the orthopaedic literature and has been shown to have detrimental effects on healing in patients undergoing various orthopaedic procedures. 6,12,18,37 Despite the many known health effects of cigarette smoking, it is still not uncommon practice in the United States. The Centers for Disease Control and Prevention has estimated that more than 40 million Americans smoke on a regular basis. 7
Prior studies have evaluated the effect on patient-reported outcome (PRO) scores in patients undergoing hip arthroscopy for femoroacetabular impingement syndrome (FAIS) at a minimum 2-year follow-up. 6,31 Studies by Cancienne et al 6 and Lall et al 31 compared a cohort of patients undergoing hip arthroscopy against a matched control group of nonsmokers. Both established that patients who smoked cigarettes had lower PROs at a minimum 2-year follow-up compared with the control group. To date, few studies have evaluated the influence of smoking in patients undergoing hip arthroscopy at midterm follow-up.
The purpose of this study was to (1) report minimum 5-year PROs for cigarette-smoking patients who underwent primary hip arthroscopy for FAIS and (2) compare these results with a propensity-matched control group of never-smoking patients. We hypothesized that patients who smoked cigarettes would demonstrate meaningful clinical improvement but that their midterm outcomes would be inferior to a propensity-matched control group of never-smokers.
Methods
Patient Selection Criteria
Retrospective data were collected and reviewed on all patients who received a primary arthroscopic hip surgery during the study period between June 2009 and March 2016. Eligible patients had 5-year minimum postoperative data for the modified Harris Hip Score (mHHS), 2 Nonarthritic Hip Score (NAHS), 10 Hip Outcome Score–Sport Specific Subscale (HOS-SSS), 39 and International Hip Outcome Tool–12 (iHOT-12). 22 Patients were excluded from this study if they had prior hip surgery, had workers’ compensation, were unwilling to consent and enroll in the study, had a Tönnis osteoarthritis grade >1, or had a previous hip condition.
Propensity Score–Matched Analysis
Eligible patients were propensity score matched in a 1:2 ratio of smokers to never-smokers. Smokers were defined as having a social history of smoking during their preoperative office visit within 1 month of surgery. Never-smokers were defined as indicating they never smoked in their social history during their preoperative office visit but met all other inclusion criteria. R (Version 4.1.0; R Foundation for Statistical Computing) was used to propensity score match smokers and never-smokers to minimize the noise from possible confounding variables. 17 Smokers and never-smokers were greedy matched without replacement according to the following characteristics: age at the time of surgery, sex, and body mass index (BMI).
Participation in the American Hip Institute Hip Preservation Registry
All patients included in this study participated in the American Hip Institute Hip Preservation Registry. Although this study presents novel findings, previous publications may have used patient data present in this study. All data collection and reporting received institutional review board approval.
Preoperative Evaluation and Surgical Indications
A detailed patient history, physical examination, and radiographic analysis were collectively utilized preoperatively by the senior author (B.G.D.) to evaluate surgical candidates. Patient variables were collected, including age at surgery, BMI, sex, operative side, and follow-up time. Gait, range of motion, strength, points of tenderness, and signs of FAIS or mechanical symptoms (ie, snapping, catching, and locking) were noted during physical examination. Radiographs were obtained and evaluated for signs of cam-type and pincer-type structures, acetabular dysplasia, and osteoarthritis in all patients using the anteroposterior pelvis, Dunn 45°, and false-profile views. 11 Radiographic measurements included the lateral center-edge angle (LCEA), 42 anterior center-edge angle, 33 alpha angle, 3 Tönnis angle of acetabular inclination, 24 and femoral head-neck offset. 23 Osteoarthritis was graded according to the Tönnis classification. 15 Cam appearance was defined as an alpha angle >55° 14,38 or femoral head-neck offset <0.8 cm. 23 Evaluations of these images were performed using a picture-archiving and communication system (General Electric Healthcare). Radiographic measurements have demonstrated good interobserver reliability in previously published studies. 16,35 Magnetic resonance imaging or magnetic resonance arthrography was obtained in all patients before surgical indication and was used to identify intra-articular pathology, such as labral tears or chondral damage. Planning was completed in patients with femoral retroversion as described by Lall et al. 30
Surgical Indications
Before surgery, all patients received at least 3 months of nonoperative treatment. Activity modification, nonsteroidal anti-inflammatory drugs (NSAIDs), intra-articular injections, and physical therapy were recommended by the senior surgeon (B.G.D.) before surgery. Surgery was only recommended when nonoperative treatments failed. 5,21 When necessary to make a diagnosis, a reaction to diagnostic injection was used as an indication for surgery.
Surgical Technique
The senior surgeon (B.G.D.) conducted all hip arthroscopies. During the procedure, patients were placed in the modified supine position on a traction table and received general anesthesia. 13,32 The hip joint was accessed through the anterolateral, distal accessory anterolateral, and modified midanterior accessory portals. During the surgery, a diagnostic arthroscopy and interportal capsulotomy were conducted. 34 Intraoperative measurements including labral tears, chondrolabral junction damage, and acetabular and femoral damage were recorded. Labral tears were assessed according to the Seldes guidelines. 40,46 Chondrolabral junction damage was classified using acetabular labrum articular disruption grades. 49 Acetabular and femoral cartilage defects were analyzed using Outerbridge categorizations. 43
Labral tears in this study were either repaired or reconstructed or underwent selective debridement. Under fluoroscopic guidance, acetabuloplasty and femoral osteoplasty were performed to address pincer-type (LCEA, >40°) and cam-type (alpha angle, >55°) morphologies, respectively, when needed. 29,44 At the end of each procedure, repair of the interportal capsulotomy was performed unless excessive stiffness, adhesive capsulitis, or insufficient capsular tissue was noted. 19
Rehabilitation Protocol
All patients received individualized rehabilitation programs customized based on the procedures conducted by the surgeon. Patients received a brace (DJO Global) to restrict the range of motion and hip flexion to 0° to 90°. Patients were also advised to use crutches to allow no more than 20 pounds (9.07 kg) of weightbearing activity for 2 weeks. Additionally, 8 weeks of physical therapy and daily stationary bike exercises were recommended, starting as early as the first postoperative day. Patients were also instructed to take NSAIDs twice daily for 4 weeks to prevent heterotopic ossification.
Surgical Outcome Tools
Patients completed questionnaires containing PROs preoperatively and postoperatively at the following time intervals: 3 months, 12 months, and annually thereafter. The mHHS, NAHS, and HOS-SSS were recorded. 2,10,27,39 Because of the study period, preoperative data for the iHOT-12 were not available for this study. Patients completed questionnaires during clinic visits. Patients unable to fill out questionnaires in the clinic were administered questionnaires through encrypted email or phone interviews. For this study, PROs from the preoperative and minimum 5-year checkpoints were analyzed.
We also reported achievement of the Patient Acceptable Symptom State (PASS), established for the mHHS, NAHS, HOS-SSS, and iHOT-12 as scores ≥74, ≥85.6, ≥75, and ≥75.2, respectively. 8,9,28,45 The maximum outcome improvement satisfaction threshold (MOIST) was calculated for all hips in the study for the mHHS and NAHS using the formula created by Maldonado et al 36 : mHHS ≥54.8% and NAHS ≥52.5%.
Statistical Analysis
All statistical analyses were performed using Microsoft Excel with the Real Statistics Add-In package (Microsoft Corp). The F test and the Shapiro-Wilk test were used to calculate the equality and normality of variance. Statistical significance in continuous data was determined using the 2-tailed t test or its nonparametric equivalent. The Fisher exact test or chi-square test was used instead in categorical data. Statistical significance was established at P < .05.
Before statistical analysis was conducted, an a priori power analysis set at 80% power was used to establish the number of hips needed when using a 1:2 matching ratio. The mHHS-expected average difference of 8 points and standard deviation of 10 points were used when running the power analysis. 25 The calculation determined that 20 hips from smokers and 39 hips from never-smokers were required to minimize type 2 errors.
Results
Patient Characteristics
A total of 35 patients met inclusion criteria for the smoker study cohort (smoking group). After inclusion and exclusion criteria were applied, 35 patients (100%) had a 5-year follow-up. The never-smoking group consisted of 70 hips. The mean ages of the smoking group and the never-smoking group were 39.4 and 38.1 years, respectively (P = .604), and the mean BMIs were 27.2 and 27.4, respectively (P = .898). Follow-up times between the smoking group and nonsmoking group were comparable (P = .060). Patient characteristics are listed in Table 1.
Patient Characteristics a

a Values are presented as mean ± SD. BMI, body mass index.
Radiographic Measurements
The mean LCEAs for the smoking and never-smoking groups were 28.8° and 30.6°, respectively (P = .250). All other radiographic measurements were also similar between both groups (Table 2).
Radiographic Measurements a
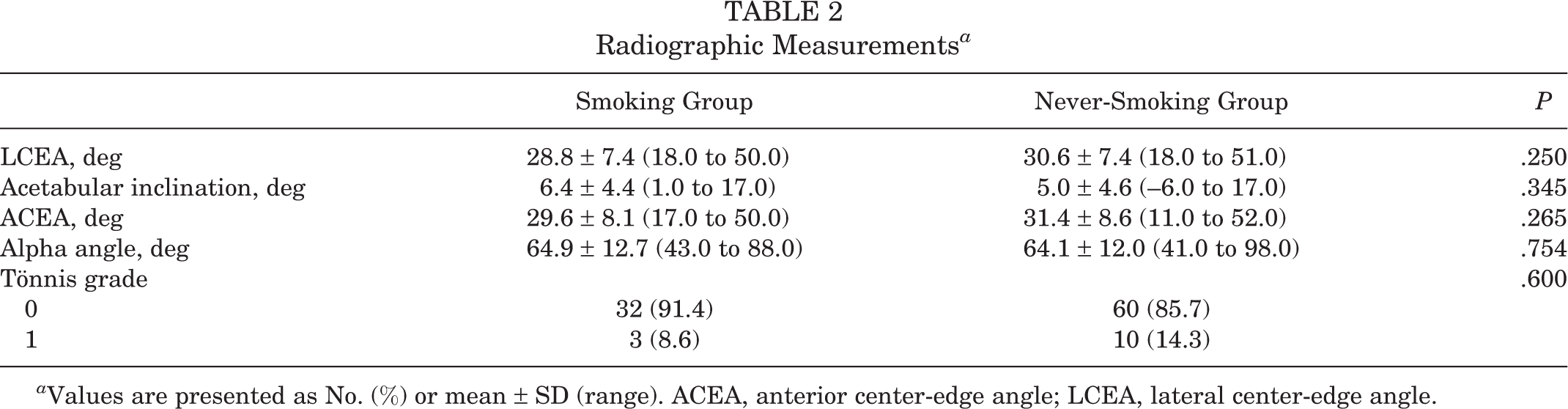
a Values are presented as No. (%) or mean ± SD (range). ACEA, anterior center-edge angle; LCEA, lateral center-edge angle.
Intraoperative Findings and Surgical Procedures
Intraoperative findings are outlined in Table 3, and surgical procedures are listed in Table 4. All intraoperative findings were comparable between the smoking and never-smoking groups. Regarding surgical procedures, there were no differences between groups in type of labral treatment (P = .134). All other surgical findings were similar between the 2 groups.
Intraoperative Findings a

a Values are presented as No. (%). ALAD, acetabular labrum articular disruption.
Surgical Procedures a

a Values are presented as No. (%).
Surgical Outcome Tools
Smokers had significantly lower preoperative scores on the mHHS (P = .043), NAHS (P = .012), and HOS-SSS (P < .001) compared with never-smokers. Smokers also trended toward lower minimum 5-year postoperative scores for the HOS-SSS (P = .076) and iHOT-12 (P = .122). All PRO data are recorded in Table 5. All data regarding PASS and MOIST are listed in Table 6.
Patient-Reported Outcomes a
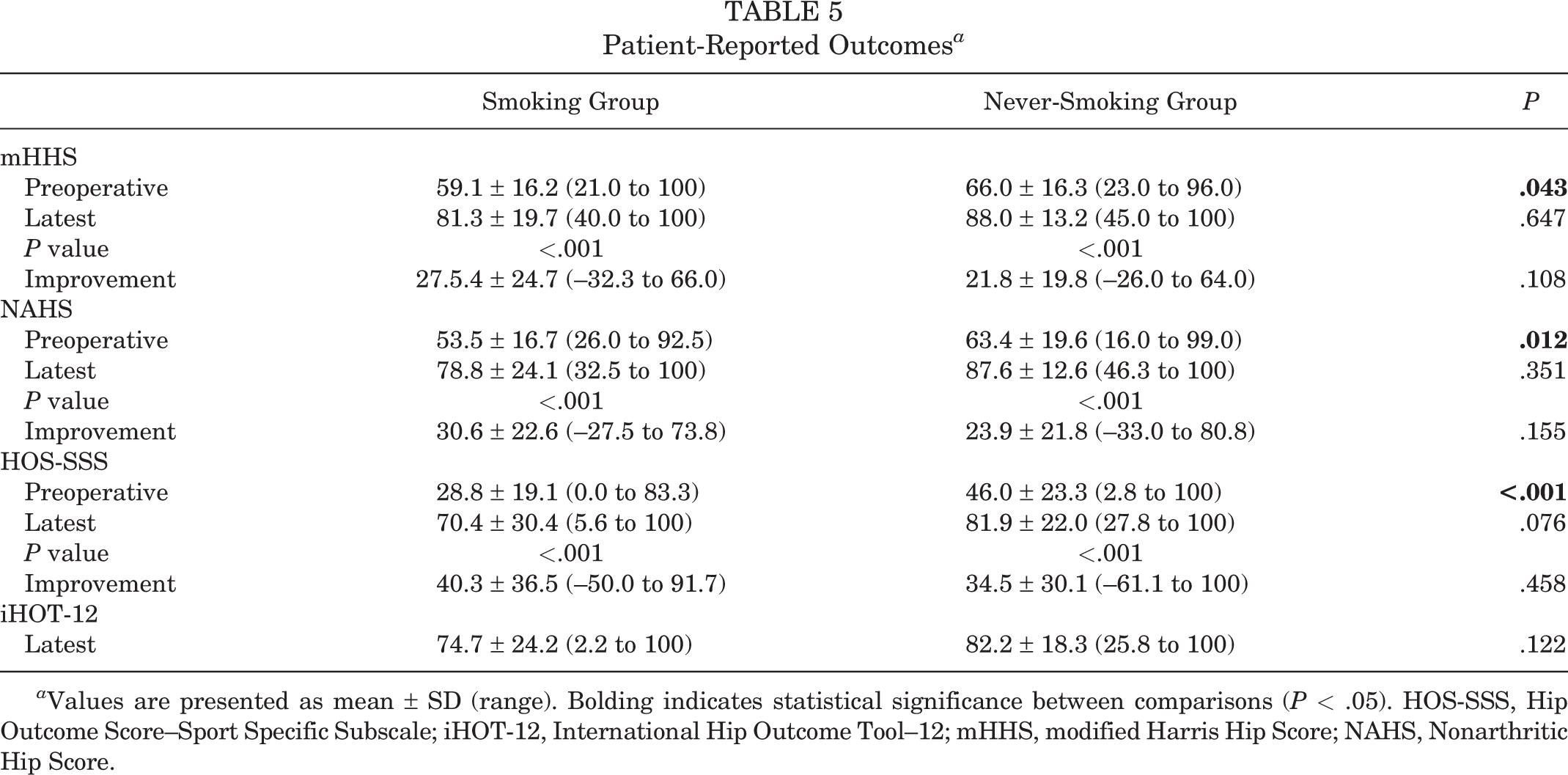
a Values are presented as mean ± SD (range). Bolding indicates statistical significance between comparisons (P < .05). HOS-SSS, Hip Outcome Score–Sport Specific Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score.
PASS and MOIST Achievement Rates a

a Values are presented as %. iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; MOIST, maximum outcome improvement satisfaction threshold; NAHS, Nonarthritic Hip Score; PASS, Patient Acceptable Symptom State.
Secondary Surgical Procedures
None of the hips in either the smoking group or the never-smoking group received a revision hip arthroscopy (P > .999). One hip in the smoking group and 4 hips in the never-smoking group received total hip arthroplasties (P = .663). Secondary surgical procedures are recorded in Table 7.
Secondary Surgical Procedures a

a Values are presented as No. (%) or mean ± SD (range), single value refers to one datapoint. THA, total hip arthroplasty.
Discussion
The important findings of this study were that patients who smoked cigarettes and underwent primary hip arthroscopy for FAIS had significant improvements in all recorded PROs at the minimum 5-year follow-up. Smoking patients had lower preoperative scores for mHHS, NAHS, and HOS-SSS when compared with a propensity-matched control group of never-smokers. Further, smoking patients trended toward lower postoperative scores for the HOS-SSS (P = .076) and iHOT-12 (P = .122) when compared with the control group; however, these trends in PROs were not significant. Smoking patients also trended toward lower rates of achieving PASS for iHOT-12 compared with never-smokers (50% vs 68.2%; P = .120).
The results presented in this paper are similar to those of prior studies evaluating the effect of cigarette smoking on outcomes after hip arthroscopy at a minimum 2-year follow-up. 6,31 Cancienne et al 6 evaluated minimum 2-year outcomes in 40 smokers undergoing primary hip arthroscopy and labral repair compared with a control group of never-smokers. In that study, the authors established inferior postoperative scores for HOS–Activities of Daily Living (ADL) and HOS-SSS, increased pain levels, and lower odds of achieving the minimal clinically important difference for HOS-ADL compared with patients who never smoked. 6 The present study found that at midterm follow-up, smoking patients trended toward lower postoperative scores for HOS-SSS but had similar rates of reaching psychometric thresholds compared with nonsmoking patients. These findings indicate that smoking cigarettes may negatively affect outcomes after hip arthroscopy at both short- and midterm follow-up but that the effect may be less pronounced at midterm follow-up. Additionally, the 2- and 5-year outcomes may be different because of the patient populations. Lall et al 31 previously matched patients with labral treatment and workers’ compensation status, but the current study did not.
Recent biomechanical studies have evaluated the biomechanical and histological effects on Achilles tendon repair in rat models. 20,26 Kennedy et al 26 established that in a rat model, nicotine exposure significantly impeded the biomechanical healing properties of Achilles tendon surgical repair, as evidenced by a lower mean load to failure compared with a control group (32.2 ± 8.4 N vs 41.0 ± 10.4 N; P = .026). Similarly, in a rat shoulder model Galatz et al 20 evaluated tendon-to-bone healing after nicotine exposure. Both the nicotine-exposed and control groups had improvement of mechanical properties over time, but the nicotine-exposed group had diminished maximal stress and force during the early healing phases. These biomechanical results offer a possible explanation for the comparatively worse outcomes seen in cigarette-smoking patients at short-term follow-up compared with midterm follow-up.
The physiologic response to nicotine in cigarette smoke has been well-documented and is likely responsible for the inferior outcomes demonstrated in the current study. The main mechanisms by which cigarette smoking impedes healing are via the vasoconstrictive and platelet-activating effects of nicotine combined with the hypoxic environment induced by carbon monoxide. 47 From a cellular level, cigarette smoking has been implicated in impeding oxidative metabolism as well as inhibiting collagen synthesis, fibroblast activity, and macrophage function. 1,41 As a result, it is likely that these cellular-level effects could have a detrimental effect on labral, capsular, and bony healing after hip arthroscopy for FAIS.
Cigarette smoking may be associated with many psychosocial factors. Brook et al 4 demonstrated that cigarette smoking in midlife women was significantly associated with alcohol use and disorder problems, financial stress, family conflict, and negative life events. This finding is not uniquely associated with women. Slopen et al 48 reports similar findings in African American adults in midlife, in which the presence of life stressors has a strong association with smoking. As a result, it is likely that smoking status may be associated with other behaviors and circumstances that may affect a person’s PROs.
This study has some notable strengths. It is among the first to compare cigarette smokers and never-smokers in patients undergoing hip arthroscopy for FAIS at midterm follow-up. Further, the present study used a propensity-matched control group to account for confounding variables and underwent an a priori power analysis to ensure adequate power. In addition, several established PROs were used to assess patient outcomes, and clinical correlation was provided by evaluating rates of achieving PASS and MOIST.
Several limitations of the current study must be mentioned. First, this was a retrospective study design, which carries inherent limitations. Smoking status was considered a binary yes/no variable, and data were not available to stratify patients based on amount of cigarette smoking. Next, determination of smoking status was based on the patient indicating that he or she smoked at the preoperative visit within 1 month of surgery. Patient smoking status was not assessed at the 5-year follow-up. It is possible that patients in the smoking group may have quit after this point and within the study period; conversely, it would be possible for patients in the never-smoking cohort to have started smoking within the study period. Additionally, other confounding variables that have a strong association with smoking, such as alcohol use and stress levels, were not matched between cohorts and could limit the external validity of these findings. Furthermore, although the conditions for an 80% threshold for power analysis were met, the nonsignificant findings of this paper might have become significant in a larger population size, warranting further studies analyzing larger cohorts. Last, the study was performed at a single institution and surgical procedures were performed by 1 high-volume hip preservation–trained surgeon. As a result, the findings of this paper may have limited generalizability.
Conclusion
Patients who smoked cigarettes and underwent primary hip arthroscopy for FAIS demonstrated significant improvement in PROs at a minimum 5-year follow-up. When compared with a propensity-matched control group of never-smokers, they trended toward lower postoperative HOS-SSS and iHOT-12 scores and lower rates of achieving PASS for iHOT-12.
Footnotes
Final revision submitted November 1, 2021; accepted November 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.E.J. has received education payments from Medwest. D.R.M. has received hospitality payments from Arthrex, Stryker, and Smith & Nephew. B.R.S. has received grants from Arthrex, education payments from Medwest and Smith & Nephew, and speaker fees from DJO Global. A.C.L. has received research support from Arthrex, Stryker, and Medacta; education payments from Medwest and Smith & Nephew; consulting fees from Arthrex and Graymont Medical; speaking fees from Arthres; and hospitality payments from Zimmer Biomet. B.G.D. has received research support from Arthrex, the Kauffman Foundation, and Stryker; consulting fees from Adventist Hinsdale Hospital, Arthrex, Medacta, and Stryker; education payments from Arthrex, Breg, and Medacta; speaking fees from Arthrex; honoraria from Medacta; royalties from Amplitude, Arthrex, DJO Global, Medacta, Stryker, and Orthomerica; and hospitality payments from Zimmer Biomet; and has had ownership interests in the American Hip Institute, Hinsdale Orthopaedics, SCD#3, North Shore Surgical Suites, and Munster Specialty Surgery Center. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Advocate Health Care Institutional Review Board (reference No. 5276).