
Abstract
Purpose:
The ideal treatment algorithm is still controversial for Superior Labral Anterior-Posterior (SLAP) tears. In this systematic review, we aimed to clarify and ascertain which treatment modality is effective and more usable in which conditions.
Methods:
In this systematic review, we used the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines established for systematic reviews and meta-analysis. “SLAP or Superior Labral Anterior-Posterior” and “biceps tenodesis” search terms were used in The Cochrane Library database and Pubmed from their inception to the 30th of September 2020. A total of 2326 titles were screened and 2069 articles were removed because of their ineligibility. Full texts of 14 studies were screened and finally, six were suitable for the present systematic review. Demographic details and study characteristics, patient satisfaction, functional outcomes, return to preinjury sports level, reoperation, stiffness, sling time and rehabilitation protocols were reviewed and compared between SLAP repair and biceps tenodesis groups.
Results:
A total of 2326 titles were screened and six studies were detected eligible. Results of 287 patients (SLAP repair: 160, Biceps Tenodesis: 127) were reviewed in included six studies. Biceps tenodesis was showed as more satisfied technique in four of the studies but the statistical comparing results of two groups were not significantly different in each study. Different functional scoring systems used in the studies were not statistically significantly different between the groups. The percentage of return to sport and preinjury level is higher in biceps tenodesis in the five studies. The total reoperation rate for SLAP repair was 19/160 (12%) and biceps tenodesis was 7/127 (6%).
Conclusion:
The biceps tenodesis has a higher return to preinjury sports level, higher patient satisfaction and lower reoperation rates but functional scores are similar between SLAP repair groups in patients with SLAP tear.
Introduction
Superior labrum anterior-to-posterior (SLAP) tears were first described by Andrew 1 in 1985 and classified into four subtypes by Snyder 2 in 1990. Sports activities especially throwing and overhead sports like baseball are related in etiology, 3,4 but falling on the outstretched upper extremity, heavy lifting, hyperextension and direct trauma also have been reported. 2,4 The patient may suffer serious pain and glenohumeral instability after the pathological disruption of the SLAP complex. 5
Type II (55%) is the most common type of SLAP tears which were classified under 4 subtypes by Snyder. 2,6 Non-operative treatment was the first focused treatment modality for SLAP tears but the low rate of return to play and return to previous level led it to surgical solutions. 7
Arthroscopic debridement, biceps tenodesis and SLAP repair are included in surgical treatment options of the SLAP tears. The SLAP repair has been the most commonly used technique but biceps tenodesis has gained popularity in recent years. 8 Repair of the SLAP tears frequently preferred and performed for acute tears, younger patients with no associated long head of the biceps tendon pathology. Older patients with degenerative structures, associated long head of the biceps tendon are usually required for performing biceps tenodesis. 8 –10
The ideal treatment algorithm is still controversial for SLAP tears. In this systematic review we aimed to clarify and ascertain which treatment modality, SLAP repair or biceps tenodesis, is effective and more usable in which conditions.
Materials and methods
In this systematic review, we used the guidelines established for systematic reviews and meta-analysis: PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses). 11
Search strategy
Literature search was performed by the three independent reviewers (O.C, K.B, M.K) according to PRISMA 11 and the search results were evaluated with senior author (A.M.O) for eligibility criteria. “SLAP or Superior Labral Anterior-Posterior” and “biceps tenodesis” search terms were used in The Cochrane Library database and Pubmed from their inception to 30th of September 2020. After reviewing the abstract and the titles full texts were reviewed for the eligibility.
Eligibility criteria
The studies included in the present systematic review were selected according to following criteria: (1) Full text available articles, (2) Full text published in English language, (3) minimum 1 year follow-up, (4) comparing the results of SLAP repair and biceps tenodesis for SLAP tears. Exclusion criteria were as follows: (1) review studies, (2) associated injuries, (3) biomechanical or cadaveric studies, (4) radiologic studies, (5) technical notes, (6) demographic studies, (7) studies in related just SLAP repair of biceps tenodesis, (8) editorial commentaries, letter to the editors, author’s response, (9) written in a language other than English, (10) full text or abstract is not available, (10) not completed studies, (11) case reports, (12) studies about physical examination, physical therapy and scoring systems, (13) course letters and (14) not related studies (Table 1).
Study characteristics.

Data extraction
The authors, the time intervals which the study was conducted, design of the study, minimum follow-up times, number of the patients included in the study, mean ages and sex of the population, scoring system used in follow-ups, patient reported outcomes and type of the SLAP tears included in the studies and the type of biceps tenodesis surgical procedure were extracted from the studies. Oxford Centre for Evidence-Based Medicine guideline was used to determine the evidence level of the study (Table 1). Information about rehabilitation protocols, sling periods, comparative results of the functional outcome scores, return to preinjury level of sports, stiffness, if a secondary operation needed or not were also extracted from the included studies (Table 2).
Postoperative protocols and follow-up parameters.

Results
Search results
The literature search included 2326 results and after duplications were removed we had 2083 abstracts. Following investigation of the abstracts for eligibility 2069 were excluded for reasons and we had 14 studies. Full texts of these 14 studies were detected and eight of them were excluded because of the reasons listed in Figure 1. At last we included six studies 12 –17 meeting the criteria (Figure 1).
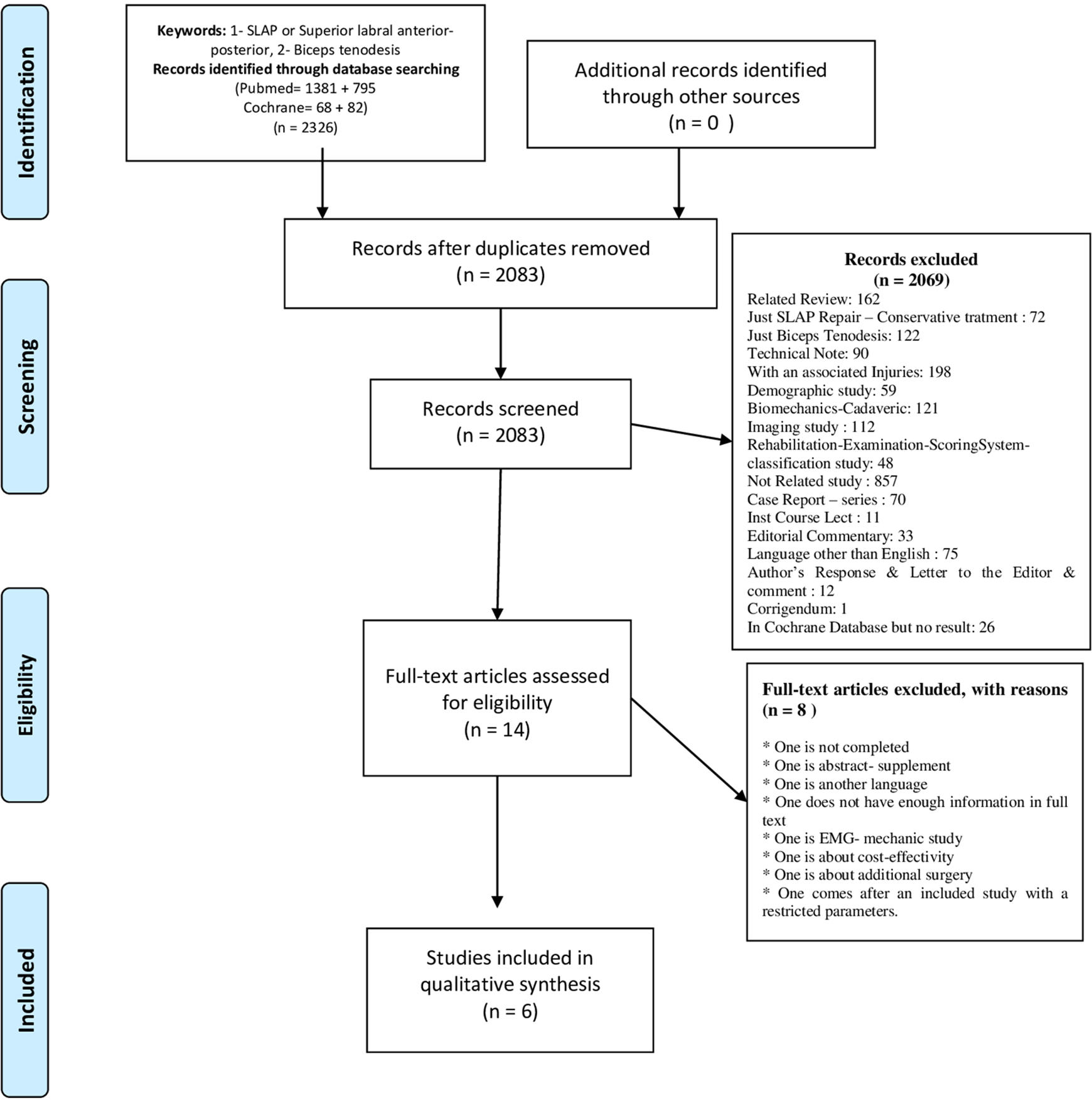
PRISMA diagram.
Demographic details and study characteristics
Level of evidence was I for one study and III for five studies. The six studies meeting the criteria included 160 patients with performed SLAP repair and 127 patients performed biceps tenodesis. Sex and age distribution according to groups are reported in Table 1. Five of the studies included just type II SLAP tears. One of the studies included type I, II, III and IV. All of the SLAP repair procedures were performed arthroscopic but biceps tenodesis was performed via both arthroscopic (3 studies) and open procedures (3 studies). Demographic information of the patients and the study characteristics are listed in Table 1.
Patient satisfaction
Four of the six included studies mentioned about patient satisfaction. 12 –14,17 These four studies included 75 patients in SLAP repair group and 65 patients in biceps tenodesis group. Three of these studies 12 –14 including 42 patients with SLAP repair and 45 with biceps tenodesis mentioned about “satisfaction or very satisfaction” of a patient via using percentage and one used 17 a mean score value of the population. In all four studies, the biceps tenodesis was showed as more satisfied technique but the statistical comparing results of two groups was not significant in each studies.
Functional outcomes
Included six studies mentioned about different functional scoring systems that they used. American shoulder and elbow surgeons score (ASES) was the most commonly used one in the included studies. 13 –15,17 Comparing of the ASES results for the two methods in each group did not show significantly different results. Western Ontario Shoulder Instability Index (WOSI) and Rowe 18 scores were used in the study established by Schrøder et al. and the comparing results were not significantly different. 16 Visual Analog Scale (VAS) was used to determine the development of the pain in four studies. 13 –15,17 These four studies reported no significant difference of VAS scores between two methods. Constant was used only in one study 12 to evaluate the functional status. General Constant score was not statistically different between the biceps tenodesis and SLAP repair group. But the “activity” subscore was statistically higher in the biceps tenodesis group (p < 0.001). 12 Denard et al. 13 used University of California Los Angeles (UCLA), Single Assessment Numeric Evaluation (SANE) and VAS for the evaluation and they did not mention any significant difference between groups. Ek et al. 14 used Subjective Shoulder Value (SSV) as an addition to the ASES and VAS. They did not report any significant difference. 14 Chalmers et al. 15 used Simple Shoulder Test (SST), ASES and VAS for the clinical evaluation and reported no significant difference.
Return to sport
Five of six studies reported about return to sportive activities. 12 –15,17 These five studies included 120 of the SLAP repair group and 88 of the biceps tenodesis. The percentage of return to sport and preinjury level was higher in biceps tenodesis in all five groups (Table 2). Boileau et al. 12 reported statistically significant difference between biceps tenodesis and SLAP in related to return preinjury level of sportive activities.
Reoperation
All six studies reported about their reoperation rates for each methods. 12 –17 Total reoperation rate for SLAP repair was 19/160 (12%) and biceps tenodesis was 7/127 (6%). Reoperation rate was high in SLAP repair group in four studies, 12,13,15,17 equal in one 14 and high in biceps tenodesis in one study. 16
Stiffness, sling time and rehabilitation
Three out of six studies including 72 SLAP repair and 69 biceps tenodesis mentioned about
The
The
Discussion
The present systematic review showed that both biceps tenodesis and SLAP repair are effective for the treatment of SLAP tears. The functional outcomes were higher for each group individually but the scores were not significantly different between SLAP repair and biceps tenodesis groups. The mean age of the patients whom biceps tenodesis was performed to, become lower over the years and there is a tendency toward biceps tenodesis instead of SLAP repair for the SLAP tears.
However, Constant, UCLA, SSV, SST, WOSI and DASH-Sport were also used in the included studies, the most commonly used
Stiffness and reoperation are the specific complications after treatment of SLAP tears. Stiffness was reported in three of the included studies 13,14,16 and the rate was always higher in the SLAP repair group. Reoperation rate changed between 0% and 40% in the SLAP repair groups of the included studies 12 –17 and always equal or higher from the biceps tenodesis group except one study. 16
Rehabilitation protocol was different in all included studies and this difference makes it difficult to compare the results. But it is clear that included studies performed more aggressive therapies 13 –15,17 or equal 12,16 to the SLAP repair and biceps tenodesis groups. It’s important to recover in a short time with a potential lower risk of stiffness is important factors especially in older populations. 14 The quality of the biceps tendon and the presence of the tendinitis always have to be taken into consideration. 24
Four of included six articles were retrospectively designed cohort studies.
13
–15,17
Two were prospectively designed and one of these two was Level I
16
and one was Level III
12
cohort study. The parameters that could not be standardized and the level of included studies are the
Conclusion
This systematic review showed that the biceps tenodesis has higher return to preinjury sports level, higher patient satisfaction and lower reoperation rates but functional scores are similar between SLAP repair groups in patients with SLAP tear.
Footnotes
Author contributions
Conception or design of the work: OC, KB, and AMÖ. Analysis or interpretation of data: OC, KB, MK, and AMÖ. Revised the manuscript critically for important intellectual content: OC, KB, MK, and AMÖ.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.