
Abstract
Background:
Despite the many studies on running-related injuries (RRIs), risk factors for injury remain unclear in the literature.
Purpose:
To investigate the risk factors of RRIs.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
An online survey was conducted among 3669 injured and noninjured runners. Injury was defined as pain of various kinds, without attention to its consequences on running practice. The survey included 41 questions on 5 main categories—personal characteristics, daily lifestyle, training and running characteristics, practice of other sporting activities, and prevention habits—as well as information about the occurrence of RRI over the previous 12 months. Continuous and qualitative variables were analyzed by Student t test and chi-square test, respectively. Sixteen variables were selected for multivariate binary logistic analysis.
Results:
Among the 3669 runners, 1852 (50.5%) reported at least 1 injury over the previous 12 months. Overuse injuries were largely represented (60.6%). The variables associated with RRIs that remained significant in the fully adjusted model were previous injury (odds ratio [OR], 1.62; 95% CI, 1.42-1.86), higher weight (OR, 1.006; 95% CI, 1.00-1.012), competitive running (OR, 1.53; 95% CI, 1.19-1.98), running >2 h/wk (OR, 1.28; 95% CI, 1.01-1.62), running >20 km/wk (OR, 1.25; 95% CI, 1.001-1.55), and stretching before running (OR, 1.46; 95% CI, 1.25-1.71).
Conclusion:
Previous injury remains the most relevant risk factor for RRIs according to the current study and previous data. Many training characteristics seem to be involved but still have to be confirmed in view of conflicting data in the literature. Further research would help clinicians better understand RRIs and how to prevent them.
Over the past few decades, there has been increased focus on healthier lifestyles in developed countries. Physical activities in daily life and running activities in particular have become popular because of their ease of implementation, low cost, and reputation of being beneficial for health. 6,19,23,27
Endurance running efficiently provides substantial beneficial effects on body mass, body fat, resting heart rate, maximum amount of oxygen, triglycerides, and high-density lipoprotein cholesterol. It has also been shown that the longer the length of training, the higher the achieved health benefits. 9 However, endurance running is associated with a high rate of injuries, especially lower extremity injuries. A large recent systematic review 5 highlighted an injury prevalence in runners of 43% ± 19.8%. The large variability observed in these results may be explained by differences in the characteristics of the target populations investigated as well as in the definition of running-related injury (RRI) used across studies. 8
Acute injuries (ankle strain, fracture) can occur, but most of the time, runners experience overuse injuries. 10 These have been defined as an injury to the muscular-skeletal system that results from repetitive submaximal loading applied over a prolonged period, causing strain that goes beyond the structure’s ability to adapt. 22 This can limit running speed, distance, duration, or frequency for at least 1 week. 10,14 The predominant site of lower extremity overuse injury is the knee, 23 and the most common injury is patellar-femoral pain syndrome. Other common overuse injuries include stress fractures, medial tibial stress syndrome, plantar fasciitis, and patellar and Achilles tendinopathies. 10
Multiple authors have tried to identify the cause and risk factors of RRI to reduce the injury rate. Risk factors are usually classified into 2 categories: intrinsic (anatomic, biomechanical, and global health) and extrinsic (training characteristic). Most studies 8,11,20,23 suggest that previous injuries are the most well-established RRI risk factor. However, these injuries are not the result of an isolated variable but rather the consequence of a structural and functional combination of different factors, and this is the main difficulty for clinicians and researchers. 7 Other risk factors are still not clear in the literature.
The goal of our study was therefore to investigate the risk factors associated with injury in a population of runners. With this survey study in a large population, our aim was to confirm that previous injury is a risk factor for further RRI. Our secondary aim was to investigate a large number of variables as potential risk factors.
Methods
This study followed the guidelines for reporting observational studies from the STROBE checklist (Strengthening the Reporting of Observational Studies in Epidemiology). 25 We conducted an online survey among runners to identify the potential risk factors for lower extremity RRI. As the participants completed the survey anonymously and on a volunteer basis, this study did not require ethical committee approval.
Population
To be included in this study, runners had to be at least 18 years old and have at least 12 months of running experience. After completing the survey, eligible participants were placed into an injured or noninjured group depending on whether they had experienced a lower extremity RRI within the previous 12 months. Injury was considered any kind of pain, without paying attention to its consequences on running practice.
The link to the survey was published on social media platforms. Several running event organizers also agreed to send the link to their large mailing lists. Numerous running magazines published the survey on their websites, and the survey was promoted at multiple running events. Data were collected from April to July 2017.
Development of the Survey
Our survey was developed through the following steps: (1) We investigated the literature to identify categories of potential risk factors, and (2) we then contacted experts (doctors, physical therapists, running coaches) and asked them to validate our categories or generate additional ones using their expertise. Finally, we developed a survey including all categories identified in steps 1 and 2. The questionnaire was developed by translating items into questions. It was made up of 35 general questions plus 6 questions related to injured runners. The questionnaire was composed of a majority of closed but also semiclosed and open questions.
The survey was divided into 5 parts. Personal characteristics: sex, age, weight, height, laterality, previous injury Daily lifestyle: professional activity type, weekly work hours, daily sleeping hours, dietary habits, tobacco/alcohol consumption Training and running characteristics: running speed, mileage and hours per week, weekly number of workouts, types of practice, trail versus road and drop, years of practice, goals of practice, annual number of competitions and distance, hydration behavior, forefoot versus rearfoot strike, planning methodology, fasted running sessions or not Practice of others sports activities and prevention habits Occurrence of RRI over the last 12 months: 1 question allowed us to categorize athletes as injured or noninjured (“I have suffered from an RRI in the last 12 months”).
Statistical Analysis
Normality of continuous variables were investigated using histogram, Q-Q plot, comparison of mean with median, and the Shapiro-Wilk test. As all the continuous variables followed a normal distribution pattern, data were expressed as means and standard deviations. Furthermore, categorical variables were expressed as absolute (number) and relative (percentage) frequencies. To identify possible associations between risk factors and RRI, we initially performed a univariate analysis using the generalized estimating equation for each independent variable, with occurrence of RRI as the dependant variable. Continuous and qualitative variables were analyzed by Student t test and chi-square test, respectively. All variables that had significant associations (P < .05) in the univariate analysis were selected for inclusion in the multivariate binary logistic analysis. The results were expressed as odds ratio (OR) and 95% confidence interval. All data analyses were performed using SPSS Statistics (Version 24.0; IBM).
Results
Participants
The survey was completed by 4105 runners. However, 436 respondents were excluded: 428 did not provide information about injury, and 8 gave inconsistent answers to open questions related to injury. Therefore, 3669 respondents were included for statistical analysis (Figure 1): 2123 (57.8%) men and 1546 (42.2%) women. The mean age of the population was 36.1 ± 10.9 years, and the mean body mass index (BMI) was 22.9 ± 4.5 kg/m2.
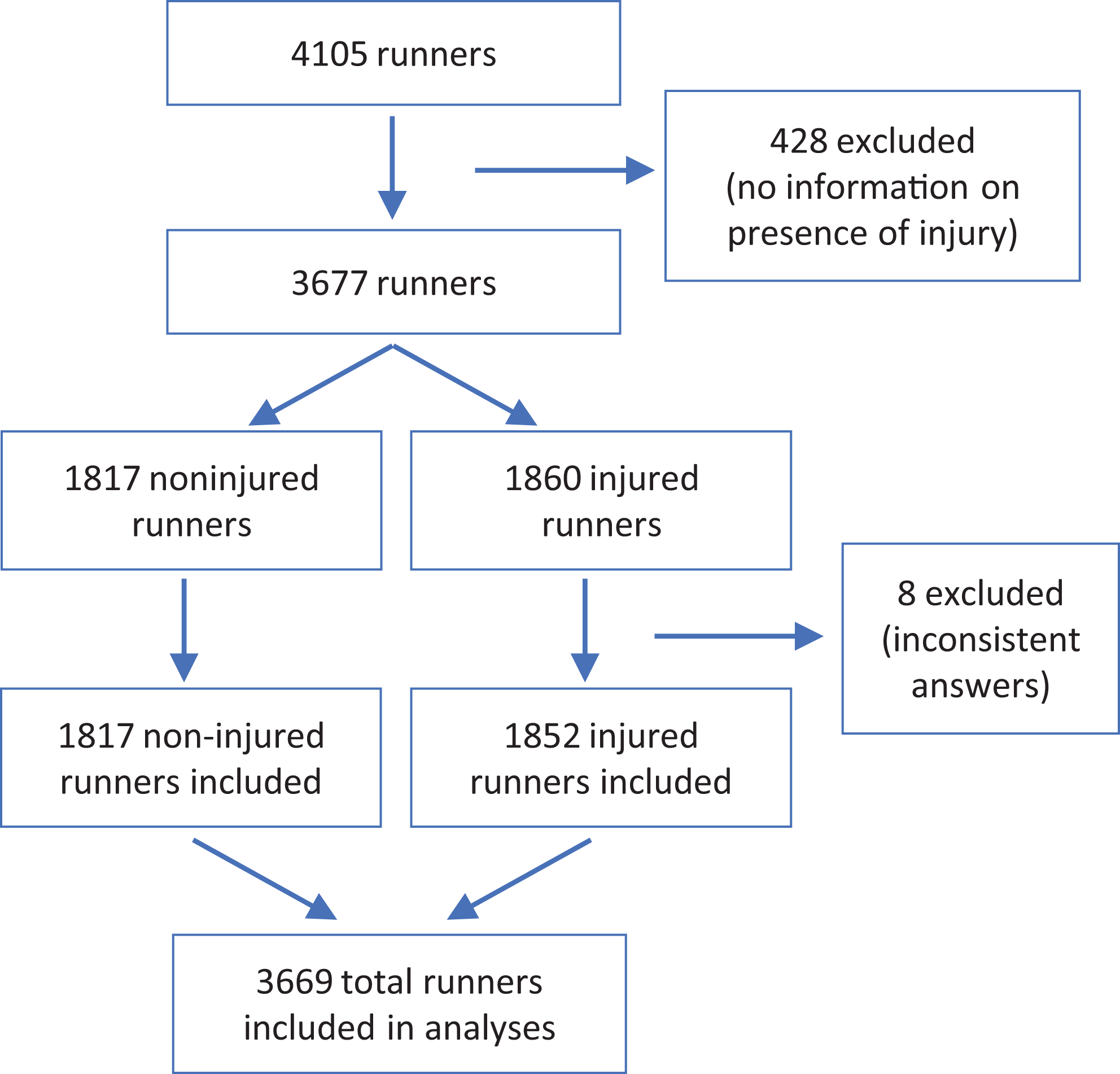
Flowchart of included population.
A total of 1852 runners (50.5%) reported at least 1 lower extremity RRI over the previous 12 months and were included in the injury group. Injured participants were significantly more often older (P < .001), heavier (P = .01), and male (P < .001). They also presented a higher prevalence of previous injuries beyond the previous 12 months as compared with noninjured participants (P < .001) and indicated a greater importance on diet (P = .03). No difference was found for height, BMI, laterality, tobacco/alcohol consumption, professional activity, or hours of work and sleeping time (Table 1).
Characteristics of the Study Participants a
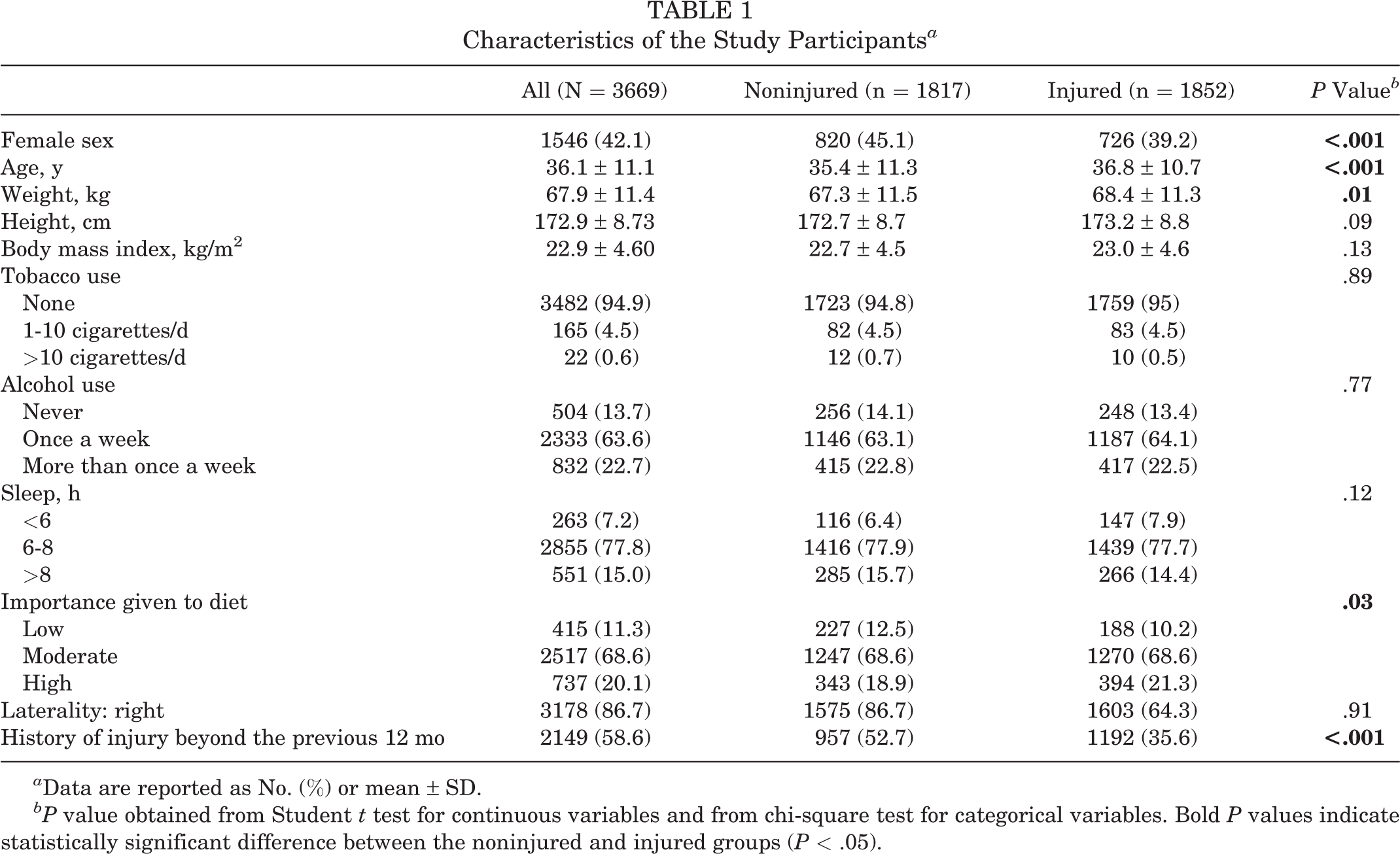
a Data are reported as No. (%) or mean ± SD.
bP value obtained from Student t test for continuous variables and from chi-square test for categorical variables. Bold P values indicate statistically significant difference between the noninjured and injured groups (P < .05).
Incidence and Typology of RRI
Most injured runners (69.5%) cited only 1 injury (Table 2). A total of 2538 injuries were reported, and 2218 pathologies were identified. The remaining 320 were classified as other because of unclear description. Among pathologies, overuse was widely represented (60.6%) and included patellofemoral pain syndrome, Achilles tendon injury, medial tibial stress syndrome, plantar fasciitis, iliotibial band syndrome, stress fracture, and back pains. Traumatic injuries (fracture and strain) and muscular injuries (stiffness/tear) represented 19.1% and 20.3%, respectively.
Information on Injuries a

a Data are reported as No. (%).
Risk Factors for RRIs
Univariate analyses revealed that some lifestyle factors were significantly associated with the risk of injuries (Table 3). Regarding training characteristics, results showed higher risks for training >2 sessions per week, training >2 h/wk, running >21 km/wk, and running >10 km/h during training (P < .001 for all). We also found significant differences for type of practice (trail runners at higher risk vs road runners; P < .001), practice goals (runners preparing for a competition at higher risk vs runners not preparing; P < .001), number of competitions per year (higher risk if >5; P < .001), running surface (higher risk if on an athletic track [P < .001] or in the woods [P = .01]), vertical drop (higher risk if the usual route includes significant elevation; P < .001), stretching session (higher risk for the ones who stretch before running; P < .001), prevention technique (higher risk for those who performing prevention techniques; P < .001).
Injury Risk Factors: Univariate Analyses a

a Data are reported as mean ± SD or No. (%).
bP value obtained from Student t test for continuous variables and from chi-square test for categorical variables. Bold P values indicate statistically significant difference between the noninjured and injured groups (P < .05).
Based on the analysis, 16 variables were included in the multivariate binary logistic analysis, and some of these associations were maintained in the multivariate model (Table 4). The following variables increased the risk of injury: heavier weight (OR, 1.006; 95% CI, 1.00-1.012), presence of a previous injury (OR, 1.62; 95% CI, 1.42-1.86), participating in competitions (OR, 1.535; 95% CI, 1.19-1.98). running >2 h/wk (OR, 1.28; 95% CI, 1.01-1.62), running >20 km/wk (OR, 1.25; 95% CI, 1.001-1.55), and, surprisingly, stretching before running (OR, 1.46; 95% CI, 1.25-1.71).
Injury Risk Factors: Multivariate Analysis

a Bold P values indicate statistical significance (P < .05).
Discussion
In the context of the growing interest in running and the numerous injuries resulting from it, the goal of our study was to investigate the risk factors associated with injuries among a large and heterogeneous population of runners. Several risk factors were identified, but only some were confirmed through multivariate regression analyses: presence of previous injury, doing competitions, running >2 h/wk, running >20 km/wk, heavier weight, and, quite surprisingly, stretching before running.
In our sample of 3669 runners, we found a 50.5% prevalence of RRIs. The prevalence of injuries has been reported to range from 19.4% to 79.3% in 1 systematic review published in 2007. 8 The large range of observed prevalence can be explained by several assessment biases. First, the RRI definition seems often to be poorly described. For example, Buist et al 4 defined an injury when pain is responsible for a total stop of running for a week, while Hespanhol et al 9 considered an injury to be a single training session not performed because of pain. In our study, we considered an injury as any kind of pain without paying attention to its consequences on running practice. Despite this very broad definition of injury, the percentage of injured runners remained modest as compared with other studies. Second, we observed large heterogeneity among studies in terms of the definition of runner and one’s level of running. Indeed, most of the training factors and personal characteristics could be different when comparing, for example, recreational and elite runners.
In our study, more than half of the injuries were overuse ones (60.6%), which seems in accordance with the available literature. 13,18 Our results highlighted that the presence of previous injuries increased the odds of injury by 62%. This is the largest association found in our multivariate model. Studies 11,23,24 have reported previous injury as one of the most common factors associated with RRI. However, Buist et al 4 emphasized that studies did not used to pay attention to the nature of these previous injuries (eg, type of injury, connection or not with running practice). Furthermore, it would be very useful to know whether the recurrent injuries are the same or related.
In addition, the results of the current study indicated that runners who took part in competitions were more at risk to develop RRI, with an increased risk of 53%. We found that only 1 study, by Walter, 26 considered this risk factor. It was a prospective study with a cohort of 1680 runners monitored during a 12-month follow-up, and the authors noted a similar strength of association (risk ratio, 1.73 [95% CI, 1.21-2.49] for men and 1.93 [95% CI, 0.97-3.89] for women). Competitive runners will usually run at a faster speed, run more kilometers, and run more frequently. However, the association of competition with higher RRI risk seems confirmed in the multivariate analysis that considered these individual parameters. Moreover, when nonprofessional runners sign up for a competition, they often do it rather late, mainly because of their other activities (eg, family, professional activities, other sports). As a result, a significant increase in the volume and intensity of their practice is typically observed within a short period. Workout-planning error (ie, errors in the variation and distribution over time of the volume and intensity of training) may also be a major factor in the occurrence of RRI, but we did not investigate this parameter in our study.
Our survey included several questions on training characteristics. Training errors are considered to be responsible for a large part of RRI. 2,8,12,26 According to our data about weekly mileage, running >20 km/wk multiplied runners’ risk of having an injury by 1.25. In the same vein, we observed that the risk of injury is increased for runners who perform >2 hours of running per week. In 2 prospective studies, Walter 26 and Macera 14 provided strong evidence that a weekly distance >64 km increased the risk of RRI. Conversely, Kelsey et al 12 and many other studies found that either there was no connection or longer distances had a protective effect. Bovens et al, 2 who expressed rate of injuries on 1000 hours of exercise, reported that the number of injuries decreased when weekly mileage during an 18-month period increased from 15 to 37 miles per week. Accordingly, in a recent systematic review that took into account data from 36 studies, Hulme et al 11 found no compelling evidence to support whether longer or shorter absolute running distances affect RRI. In this same review, the authors concluded, using 8 prospective and retrospective studies, that there was not enough scientific evidence of any relation between duration and RRI development.
Univariate and multivariate analysis uncovered connections with weight. The heavier runners would be more at risk of RRI. In contrast, no significant differences were found for BMI. Most of the studies did not find any connection with weight, 11,26 while others reported some conflicting data. Our data are consistent with several studies 11,15,23 showing no significant connections between BMI and RRI. In contrast, Nielsen et al, 16 who performed a 1-year follow-up of 930 novice runners, stated that runners with a BMI >30 kg/m2 were significantly more at risk to injury. Buist and Bredeweg 3 noted similar results: increased risk by 31.8% of sustaining an RRI among novice runners with a BMI >25 kg/m2 versus <25 kg/m2. Faced with the conflicting results, more studies should be performed to assess this point.
We found more injured runners among the ones who are used to stretching before training sessions or at another time. Shrier 21 conducted a meta-analysis on this variable. Among 17 studies that examined stretching before running, 7 suggested that it was beneficial, 3 indicated that it was detrimental, and 7 noted no difference. When results of all these studies are pooled, the clinical evidence does not support the evidence that stretching before exercise prevents injury. Authors also highlighted that stretching at another time than just before or after the race may have a protective effect. However, only 2 studies isolated the effect of stretching after running or at another time. From our point of view, it is very hard to study the effect of stretching because of numerous variables (number of muscles stretched, tension level, duration, number of repetitions, active or passive stretches, etc). Even if we frequently see in clinical practice that athletes who perform stretching have already been injured and stretch precisely to avoid any new injury, our results did not support this hypothesis. Indeed, results revealed that the contribution of stretching beforehand was independent of history of injury.
One of the particularities of our study was to study RRI incidence between road runners and trail runners. Indeed, we did not find a single study that focused on this aspect. However, once again, these 2 kinds of practices included several variables, and it would be very difficult to extract clear data out of this study. We found significantly more injured runners among trail runners, but the relationship was not confirmed in multivariate analysis. Several points could be discussed regarding this relationship. First, it would be interesting to study injury typology and incidence of traumatic injuries (eg, ankle and knee strain, fracture). Without considering traumatic injuries, this relationship would nevertheless be conserved, explained by the course’s topography (eg, more demanding ascents and descents) as well as the ground’s topography (importance of the muscles supporting the pelvis and the back when the ground is not flat). Moreover, we found a significant difference regarding vertical drop (ie, more injured runners with higher vertical elevation). Furthermore, the theoretical protective effect of running on a soft surface was discussed in 1 study in which authors measured vertical acceleration of the tibia on 35 runners who ran on different surfaces at different speeds. 1 In contrast, Hulme et al 11 gathered results from 19 studies focusing on this point and concluded that topographic features and the compliancy of particular surfaces did not affect RRI risk. Our data on surface uncovered more injured runners among those who perform some athletic track sessions. This result makes sense because track racers usually do a lot of interval running. In hindsight, it would have been interesting in our questionnaire to consider this type of training as a potential risk factor of RRI.
We consider that the main strength of this study was the large number of respondents and variables studied. Furthermore, to our knowledge, no studies have compared injury rate between trail runners and road runners. There are, however, some limitations to this study. First, it was a retrospective study, and runners had to remember a lot of information about last 12 months, leading to a recall bias. Second, the injured status was self-reported. There was no medical diagnosis allowing for the objectification of the injury. Last, regarding training characteristics, we took into account the mean value for pace, mileage, and frequency over a period of time. For these parameters, we discussed the importance of variation over time to explain injury occurrence.
In light of these last sections, the link between training characteristics and running injuries seems to be very complex. We discussed several methodological discrepancies that can explain some of this complexity. Some other points could be considered. Theoretically, injury occurs when cumulative training load, over 1 or several runs, exceeds the capacity of various tissues to perform adaptive repair. 10 Accordingly, this training load should be evaluated at each training session. Furthermore, this training load will have a different impact on tissues depending on distribution over a period of time. This final point explains why fixed or absolute data, such as mean weekly values, seem to be inappropriate. Nielsen et al 17 conducted a systematic review on this point (training errors) and came up with the hypothesis that a complex relationship involving distance, frequency, duration, and pace should exist and has not been investigated yet. It is probably the reason why data recorded until now have not allowed us to better understand these running-related risk factors.
Conclusion
This study confirms that previous injury remains the primary risk factor for RRI. Other main risk factors for RRIs have been highlighted in our survey: being a trail runner, doing competitive running, running >2 h/wk, and stretching before running. Future targeted and prospective studies should be able to improve risk factor knowledge and result in the implementation of effective preventive measures.
Footnotes
Acknowledgment
The authors thank all participants who kindly responded to the survey.
Final revision submitted April 20, 2021; accepted May 25, 2021.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.