
Abstract
Introduction
Indoor climbing injuries are often related to overuse, and climbers choose between self-management and seeing a medical practitioner. This study evaluated predictors of prolonged injury and seeking medical care for indoor climbing injuries.
Methods
A convenience sample of adult climbers from 5 gyms in New York City was interviewed about injuries over the past 3 y, because of which they stopped climbing for at least a week or saw a medical practitioner.
Results
In total, 122 of 284 (43%) participants had at least 1 injury, for a total of 158 injuries. Fifty (32%) were prolonged, lasting at least 12 wk. Predictors of prolonged injury included older age (odds ratio [OR], 2.28, per 10-y increase; 95% CI, 1.31–3.96), hours per week spent climbing (OR, 1.14, per 1-h increase; 95% CI, 1.06–1.24), climbing difficulty (OR, 2.19, per difficulty group increase; 95% CI, 1.31–3.66), and years of climbing experience (OR, 3.99, per 5-y increase; 95% CI, 1.61–9.84). Only 38% of injuries were seen by a medical practitioner. Predictors of seeking care included prolonged injury (OR, 3.04; 95% CI, 1.39–6.64) and rope climbing preference (OR, 1.98; 95% CI, 1.02–3.82). The most common theme for seeking care was serious pain or interference with climbing or daily activities.
Conclusions
Despite prolonged injuries being common, especially in older, more experienced, and higher-level climbers, only a third of climbers with injuries seek medical care. Outside of injuries causing minimal pain or limitation, those who self-managed reported receiving advice from other climbers or online research as a prominent reason for that choice.
Keywords
Introduction
Although rock climbing originated from mountaineering, the number of indoor climbers in the United States now more than doubles those who climb outdoors. 1 Indoor climbing injuries are most often overuse injuries of the upper extremity 2 and less often from acute trauma. 3 However, many prior studies have used a severity scale that is most suited to the types of injuries that occur when climbing outdoors 4 that classifies most indoor climbing injuries as minor.3,5,6 As a result, the frequency and duration of injuries that occur indoors are poorly understood as well as the decisions to seek medical care or not.
The purpose of our study was to examine the nature of indoor climbing injuries, focusing on duration of injury and decision to seek medical care. To do this, we conducted an interview study evaluating the frequency, distribution, and duration of injuries in gym-based climbers, the factors associated with prolonged injury, the measured factors associated with seeking medical care, and the subjective reasons for seeking medical care or self-management. We examined age, sex, experience, climbing difficulty and frequency, style of climbing, and injury location as factors that might be associated with prolonged injury and seeking medical care.
Methods
The study was approved by the Montefiore Einstein institutional review board.
Indoor climbers were interviewed about their experience with injuries and their decision to seek medical care. A convenience sample of climbers was recruited in person, subject to researcher availability during the predetermined data collection period, resulting in 19 morning or evening visits to 5 climbing gyms in New York City between October 2020 and July 2021. Climbers were informed about the study and, if interested, were screened to determine eligibility. If eligible, participants were asked for consent and given a choice to be interviewed immediately or contacted at a later date and interviewed over the phone. Verbal responses were written down by the interviewer and then transcribed into the database.
Climbers 18 y or older who climbed ≥4 times in the past year were eligible to be included in the study. An acute injury was defined as one sustained while climbing within the prior 3 y, a timeframe similar to those used in prior studies, 7 that required the participant to either see a medical practitioner or, after the injury, stop climbing for at least a week. Climbers of <18 y of age and pregnant women were excluded. Chronic injuries, such as those with similar characteristics recurring in the same location, were excluded. Additionally, except as part of the calculation of injury prevalence, injuries for which care was sought from the emergency department were excluded.
For each participant, demographic and climbing characteristics were recorded, including the difficulty grade at which they climbed most often. We used the International Rock Climbing Research Association scale 8 to reconcile the Yosemite Decimal System and the Hueco grades used to measure the difficulty of rope climbing and bouldering, respectively. To account for climbers not reporting on subgrades, for instance 5.10a vs 5.10b, we grouped the grades based on rope climbing difficulty: beginner (≤5.9), low intermediate (5.10 or V0), high intermediate (5.11 or V1–3), advanced (5.12 or V4–7), and elite (5.13 or ≥V8). In addition, whether each participant had medical insurance or a primary care practitioner at the time of at least 1 injury was assessed.
The characteristics of each injury were recorded. To classify the anatomic location of each injury, we used the Orchard Sports Injury and Illness Classification System, 9 except for identifying finger injuries specifically. Duration of injury was defined as time from injury to return to climbing activities with little or no pain or limitation. An injury of ≥12-wk duration was considered prolonged, a definition that has been used previously. 10
For each injury, participants were asked whether they sought medical care and whether they required surgery. They were asked to report all of the reasons for their decision to self-manage or seek medical care for their injury in an open-ended semistructured interview format (see online Supplemental Material).
Characteristics of participating climbers and injuries are reported using summary statistics. The primary outcomes were prolonged injury and seeking medical care. The associations between each predictor and outcome were examined using univariable logistic regression models with Wald statistics used to measure significance. P values of <0.05 were considered significant. Because the study is considered exploratory, no adjustment for multiple hypothesis testing was done. Stata, version 17.1 (College Station, TX), was used for all statistical analyses.
Thematic analysis was performed on the responses to the open-ended question of why each climber sought or did not seek medical care. Reported themes included both those that were anticipated and asked about explicitly and those that were elucidated during follow-up questioning. These themes were then categorized into the final major themes in each of the self-management and seeking care groups.
All recruitment and interview activities were conducted by 1 researcher. Thematic analysis, including categorization and revision of themes, was conducted by the interviewer and a second researcher.
Results
Of the 284 climbers who met eligibility criteria and agreed to participate, 122 had an acute injury, resulting in a 3-y prevalence of 43%. Of the injured participants, 22 did not complete the interview, leaving a remaining sample of 100 climbers and 158 acute injuries, excluding those who were seen in the emergency department (Figure 1).
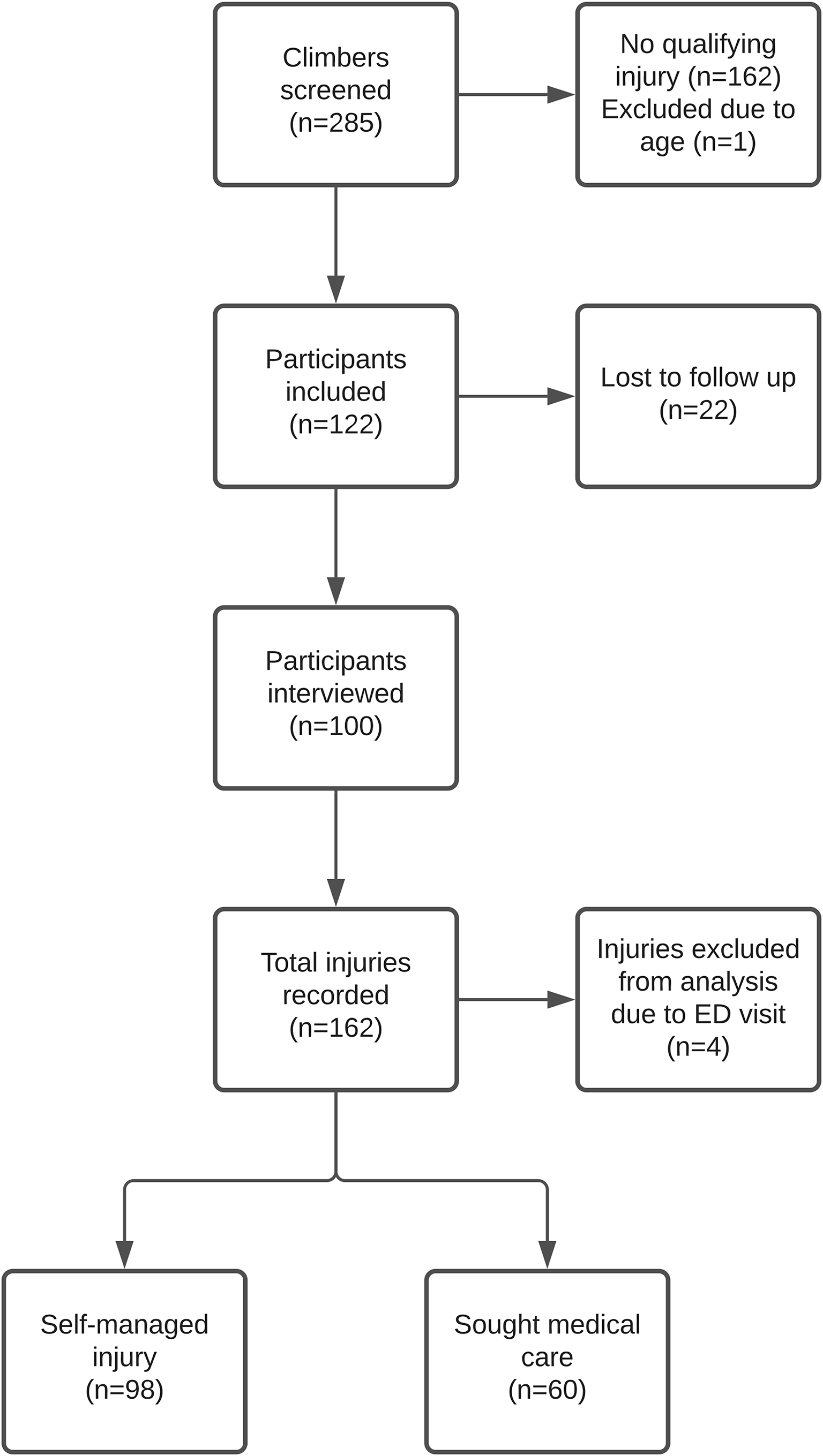
Consolidated Standards of Reporting Trials flow diagram. ED, emergency department.
Of the 100 injured participants who were interviewed, the mean age was 31.4 y, and 75 (75%) were men. They reported a mean climbing experience of 5.6 y and a mean climbing frequency of 8.3 h/wk. The most common climbing levels were high intermediate (5.11 or V1–3), 24%, and advanced (5.12 or V4–7), 52%. During the 3-y period, 93% of the participants reported having had medical insurance but only 58% a primary care practitioner (Table 1).
Participant characteristics
avg, average.
Of the 158 injuries, 68% were of the upper extremity, 22% were of the lower extremity, and 9% were of nonextremity origin. The 5 most common injury locations were finger (39%), shoulder (14%), ankle (13%), elbow (10%), and knee (6%). Only 6 injuries required surgery, and of those, 3 were for the shoulder (Table 2).
Injury characteristics
avg, average.
The number of prolonged injuries (≥12 wk) was found to be 50 of 158 (32%). Of the 5 most common injury locations, the knee (40%) had the highest proportion of prolonged injuries, followed by shoulder (32%), finger (29%), ankle (25%), and elbow (25%).
Factors significantly associated with prolonged injury included older age (odds ratio [OR], 2.28, per 10-y increase; 95% CI, 1.31–3.96), hours per week dedicated to climbing (OR, 1.14, per 1-h increase; 95% CI, 1.06–1.24), climbing difficulty (OR, 2.19, per difficulty grade group increase; 95% CI, 1.31–3.66), and years of climbing experience (OR, 3.99, per 5-y increase; 95% CI, 1.61–9.84). Sex, climbing style preference, and injury location were not associated with prolonged injury (Table 3).
Predictors of prolonged injury
OR, odds ratio.
Of the 158 injuries examined, 98 (62%) were self-managed and 60 (38%) prompted seeking medical care. Factors significantly associated with seeking medical care included prolonged injury (OR, 3.04; 95% CI, 1.39–6.64) and rope climbing preference (OR, 1.98; 95% CI, 1.02–3.82). Age, sex, climbing experience, hours per week, climbing difficulty grade, and having a primary care practitioner or having medical insurance were not significantly associated with seeking medical care (Table 4). Injury location was not significantly associated with seeking medical care, but the knee had the highest proportion of injuries for which medical care was sought (60%), and fingers had the lowest proportion (26%).
Predictors of seeking medical care for injury
OR, odds ratio.
Among injuries that were self-managed, reasons for self-management were represented by 5 major themes (Table 5): minimal pain or interference with climbing or daily activities (55%), reassured by another person or self-research (47%), prior experience or knowledge managing the injury (39%), unwillingness to seek medical care (37%), and difficulty accessing medical care (28%) (Table 5).
Thematic analysis of the reasoning behind self-management or seeking medical care (major themes)
Among injuries for which the climber sought medical care, reasons for seeking care were represented by 2 major themes: serious pain or interference with climbing or daily activities (87%) and worry about the diagnosis or long-term effects (33%) (Table 5). Less frequent themes included prior positive relationship or experience with a medical practitioner (14%), influenced to see a medical practitioner by another person (14%), and injury recurrence or interest in prevention (12%).
Discussion
In this retrospective study of self-reported injuries from a convenience sample of climbers at indoor gyms, we found that 32% of injuries studied were prolonged, with symptoms lasting ≥12 wk. Several factors were associated with prolonged injury, including age, increasing years of climbing, increasing climbing difficulty, and increasing climbing volume. Injured climbers only sought care for 38% of injuries. Prolonged injury was associated with an increased likelihood of seeking medical care. No association was found between whether the climber had medical insurance or a primary care practitioner and seeking care. The most common theme cited for seeking care was severe pain or limitation to climbing or daily activities.
Two prospective studies evaluating recreational indoor climbers also described elevated injury rates with 1-y incidences of 43% and 44%.2,5 Our finding of a 3-y prevalence of 43%, although high, may have been an underestimation of true injury burden, as we excluded chronic injuries and those presenting to the emergency department.
We found not only a high frequency of injuries but also a high proportion of prolonged injuries, 32%. Our finding illustrates how duration of acute injury may be important to characterize injury severity in addition to the UIAA (Union Internationale des Associations d'Alpinisme) MedCom Score. 4
There have been many studies evaluating the risk factors for climbing injury. In the literature review by Woollings et al, 11 some studies found increasing age,12,13 male sex,12,14 increasing years of climbing,14,15 increasing climbing difficulty,14,15 increasing climbing volume, 15 and bouldering 16 to be associated with increased risk of injury. Other studies did not find such associations. 17 -19 In our study, we examined these risk factors, in addition to injury location, not for their association with injury in general but rather for their association with prolonged injury. Despite this difference in study design, we found that the associated factors were similar to many of those described in previous research. 14
In our study, 38% of climbing injuries were seen by a medical practitioner. This was consistent with other studies showing that a minority of injured climbers (31–40%) seek medical care. 20 -22 We found prolonged injury and preference for rope climbing to be the only 2 factors associated with seeking care. An explanation for the association with rope climbing was not elucidated in our study and could warrant further research. It is notable that we did not find an association between having a primary care practitioner or health insurance with seeking care. Among the climbers who sought care, the predominant reported theme was that of serious pain or limitation. Other themes such as concern about long-term effects or interest in injury prevention were much less common. Accordingly, among those who did not seek care, the absence of such pain or limitation was the most common theme reported. Taken together with the association between prolonged injury and seeking care, this suggests that climbers may seek care only out of necessity. However, there were additional reported themes that were almost equally as common in injuries that were self-managed, including first, advice or reassurance being obtained from another person or self-research, and second, an unwillingness to seek medical care, such as having a belief that a medical practitioner could not do anything for the injury. Grønhaug et al 23 found similar themes in their study in which 24% of climbers reported a similar doubt about the knowledge of health professionals regarding climbing-related injuries, and 6% reported receiving help from a friend. However, our discovery that many climbers prefer self-research, often online, is a new observation.
Limitations
The study has several limitations. Retrospective survey data have the risk of recall bias, and participants were asked to recall the details surrounding injuries over the previous 3 y. In-person recruitment and convenience sampling may have increased the risk of sampling bias and led to a low sample size. The participants were recruited from a small number of gyms in New York City, which may limit the generalizability of the results to other geographic areas due to factors such as variability in grading practices. The study was conducted during the early stages of the COVID-19 pandemic, which may have affected injury prevalence and the participants’ decision to seek care for some injuries. We did not specifically exclude competitive climbers and those who also climb outdoors. Climbers who engage in these activities may have characteristics or attitudes that may not be found in all gym-based climbers. We excluded injuries for which care was sought in the emergency department. Although we did so to avoid the inclusion of potentially severe injuries in which the climber did not have the choice between self-management and seeking medical care, and there were only 4 such injuries, this may have led to an underestimation of prolonged injury and the neglect of reasons for seeking care unique to those injuries. We excluded chronic injuries, which may have similarly led to an underestimation of injury burden. Furthermore, chronic injuries causing lengthy pain and disability may be common, 24 and we were unable to examine their association with prolonged injury. We did not collect demographic characteristics from the noninjured climbers. Further analysis between noninjured and injured climbers was not possible. The qualitative nature of the semistructured interview process could have led to reasons for self-management or seeking care being incompletely captured.
Conclusions
In conclusion, in our limited retrospective study of self-reported injuries from a convenience sample of gym-based climbers, we found a 3-y injury prevalence of 43%. Of the injuries analyzed, 32% were prolonged. The results of this study suggest that prolonged injury was common among gym-based climbers, especially those of older age, those who climb at high difficulty levels, those with higher levels of experience, and those who climb frequently, yet only a third of injured climbers sought medical care. Outside of injuries causing minimal pain or limitation, those who self-managed reported receiving advice from other climbers or online research as a prominent reason for that choice.
Footnotes
Acknowledgments
The authors acknowledge the 5 gyms that permitted data collection: The Cliffs at LIC, Brooklyn Boulders Queensbridge, Brooklyn Boulders Gowanus, Vital Brooklyn, and GP81. The authors also thank Amanda Lopez for assistance in data organization.
Author Contributions: study concept and design (JL, WS); IRB approval (JL, WS); data acquisition (JL, WS); data analysis (ZP); drafting and critical review of the final manuscript (JL, ZP, WS); approval of the final manuscript (JL, ZP, WS).
Financial/Material Support: None.
Disclosures: None.
Supplemental Material(s)
Supplementary material associated with this article can be found in the online version at