
Abstract
Background:
The International Hip Outcome Tool (iHOT-33), which is a self-administered questionnaire that contains 33 questions, was developed to evaluate young to middle-aged physically active adults with hip pathology.
Purpose:
To translate and cross-culturally adapt the iHOT-33 to create a Thai version of the iHOT-33 (TH-iHOT-33) and to determine the validity and reliability of the TH-iHOT-33.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Translation and cross-cultural adaptation of the iHOT-33 were performed according to international guidelines. Patients aged 18 to 60 years with hip disorders who had a score ≥4 on a modified version of the Tegner activity scale completed the TH-iHOT-33 twice, 2 weeks apart. The Thai versions of the HOOS (Hip disability and Osteoarthritis Outcome Score) and EQ-5D-5L (European Quality of Life–5 Dimensions–5 Levels) were also completed at baseline. At 2 weeks, the Global Perceived Effect scale was completed in addition to the TH-iHOT-33. The statistical testing for validity included construct validity and hypotheses testing. Internal consistency, test-retest reliability, and measurement error were analyzed to determine reliability.
Results:
The iHOT-33 was successfully translated and cross-culturally adapted to create the TH-iHOT-33. Seventy-two patients with various hip disorders participated in this study. Of the predefined hypotheses used for construct validity, 86% were confirmed. A Cronbach alpha of 0.98 (95% CI, 0.97-0.99) demonstrated excellent internal consistency. Test-retest reliability was high, with an intraclass correlation coefficient of 0.83 (95% CI, 0.73-0.90). The standard error of measurement was 5.1 points. The smallest detectable change was 14.2 points at the individual level and 1.9 points at the group level. The minimal important change was 10.9 points. The TH-iHOT-33 had no observable floor or ceiling effects.
Conclusion:
The TH-iHOT-33 is a valid and reliable instrument for assessing the functional status and health-related quality of life of young to middle-aged physically active Thai adults with hip disorders.
Keywords
Patient-reported outcomes (PROs) are important tools for evaluation of the patient’s health condition from the patient’s perspective. 14 Either generic or disease-specific questionnaires have been used in research and clinical practice for assessing a change in a patient’s health status after an intervention. 3,14 PROs are considered the gold standard for measuring outcomes for nonsurgical and surgical treatment. 31 Traditional PROs for patients with hip disorders were usually developed for patients with osteoarthritis or for patients who underwent hip replacement surgery. 19 Over the past decades, various conditions that cause hip pain in young adults have gained recognition, especially femoroacetabular impingement syndrome and labral tears. 27 Several hip-specific PROs were developed for assessing the functional status and health-related quality of life (QoL) of young to middle-aged patients who were physically active in their activities of daily living, occupations, and sports. 4,6,13,15,30 Kemp et al 11 showed that the modified Harris Hip Score and the subscales related to activities of daily living of the Hip disability and Osteoarthritis Outcome Score (HOOS), Hip Outcome Score, and HAGOS (Copenhagen Hip and Groin Outcome Score) demonstrated ceiling effects when they were used to evaluate outcomes of hip arthroscopic surgery.
The International Hip Outcome Tool (iHOT-33) is a self-administered questionnaire that was developed by the Multicenter Arthroscopy of the Hip Outcomes Research Network to evaluate young to middle-aged active patients with symptomatic hip pathology. 15 This QoL PRO measure has good psychometric properties relating to validity, reliability, and responsiveness. 11,15,25,31 The iHOT-33 tool has been translated and validated in several languages. 1,12,23,26,32 To use the iHOT-33 to evaluate Thai patients with hip pathology, the aim of this study was to translate and cross-culturally adapt the iHOT-33 questionnaire to create the Thai version of the iHOT-33 (TH-iHOT-33) and to determine the validity and reliability of the TH-iHOT-33. We hypothesized that the TH-iHOT-33 would be a valid and reliable instrument for assessing the functional status and health-related QoL of young to middle-aged physically active Thai adults with hip disorders.
Methods
This cross-sectional study was conducted from August 2018 to September 2020. The study consisted of 2 parts: (1) translation and cross-cultural adaptation of the iHOT-33 from the English-language version into the Thai-language version and (2) evaluation of the validity and reliability of the TH-iHOT-33 in young to middle-aged physically active Thai adults with hip disorders. The protocol for this study was approved by an institutional review board, and informed consent was obtained from all study participants.
Translation and Cross-Cultural Adaptation
After permission was received from the original authors, 15 the iHOT-33 was translated into the Thai language following the international guidelines for the process of cross-cultural adaptation of self-report measures. 2 Forward translation was independently conducted by 2 bilingual translators: an orthopaedic surgeon and an uninformed professional translator. Both translations were compared and synthesized into a preliminary TH-iHOT-33 questionnaire in a consensus meeting. Two professional translators then independently translated that Thai version back into English. Both translators were unaware of the study objectives and the original questionnaire. These back-translations were then compared with the original version by an expert committee. Minor discrepancies regarding word choice were discussed and resolved by consensus; this resulted in a prefinal TH-iHOT-33. This prefinal version was tested on 20 Thai patients with hip disorders to assess understanding and to identify problems. Patient understanding was good and no problems were identified, so the prefinal version was adopted as the final version of TH-iHOT-33 with no additional changes.
Study Procedure
The procedure to evaluate the validity and reliability of the TH-iHOT-33 was performed according to the recommendations in the COSMIN checklist (Consensus-Based Standards for the Selection of Health Measurement Instruments). 16,17 Patients with hip disorders were included if they were aged 18 to 60 years and they had a score ≥4 on a modified version of the Tegner activity scale. 28 This activity level was used to identify physically active individuals in the development of the original iHOT-33. 15 Patients were excluded if they had insufficient understanding of the Thai language or cognitive impairment that prevented reliable completion of the questionnaires used in this study. Patients who had disorder of the back or the contralateral lower extremity, active hip joint infection, or musculoskeletal malignancy were also excluded.
All patients were first evaluated in an outpatient setting. They were asked to complete 3 paper-based questionnaires: the TH-iHOT-33, the Thai version of the HOOS, 33 and the Thai version of the European Quality of Life–5 Dimensions–5 Levels (EQ-5D-5L). 22 They were also provided with a stamped preaddressed envelope and the second set of questionnaires, including the TH-iHOT-33 questionnaire and the Global Perceived Effect (GPE) scale, which patients were instructed to complete 2 weeks after the first set of questionnaires were completed. This interval was considered sufficiently long to prevent recall of previous responses and recent enough to ensure minimal clinical changes. 29 All PROs used in this study were paper-based questionnaires.
Questionnaires
The iHOT-33 is a disease-specific self-report questionnaire that consists of 33 questions. These questions are divided into 4 domains: symptoms and functional limitations (16 items); sports and recreational activities (6 items); job-related concerns (4 items); and social, emotional, and lifestyle concerns (7 items). 15 Every question uses a visual analog scale response format that is designed for conversion to computer- and web-based self-administration. Each question is scored from 0 to 100 points. The total score represents the sum of all answered questions divided by the number of answered questions. Higher scores represent better physical function and health-related QoL. 15 It is possible to calculate a separate score for each domain, but there was no attempt to score the 4 domains separately. 15
The HOOS is a disease-specific questionnaire to evaluate patients with hip disability with or without osteoarthritis. 19,20 This questionnaire has been translated into Thai and has shown good psychometric properties. 33 The HOOS consists of 40 items with a 5-point Likert scale format. These 40 items are divided into 5 subscales: symptoms, pain, activities of daily living, sport and recreation function, and hip-related QoL. The HOOS can be transformed into a 0 to 100 scale of total score or separate subscale. 20 Higher scores represent better function and fewer symptoms.
The EQ-5D is a generic health-related QoL assessment tool. 7,24 This questionnaire was developed by the EuroQol Group. 24 It consists of 5 items assessing 5 dimensions of health status: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D-5L is a new version of the questionnaire, and each item has 5 levels of response. 7 The calculated utility score of the EQ-5D-5L ranges from 0 to 1. Higher scores indicate better health-related QoL. This questionnaire has been translated into many languages worldwide, including Thai. 22
The GPE scale is used to assess changes in the patient’s health status according to the patient’s perception. The scale asks the patient to rate how much his or her condition has deteriorated or improved from baseline. 10 This study used an 11-point GPE scale ranging from –5 (vastly worse) to 0 (no change) to +5 (completely recovered). 5 In the second assessment, the GPE scale was completed with the TH-iHOT-33 to identify a group of patients with no clinically relevant change (who had a GPE scale score of –1, 0, or +1) for assessment of test-retest reliability.
Statistical Analysis
Statistical analyses were performed using PASW Statistics for Windows (Version 18.0; SPSS Inc). A P value <.05 was considered statistically significant. A Bland-Altman plot was also produced using MedCalc Statistical Software (Version 16.4.3). Patient demographic and clinical characteristics are summarized using descriptive statistics. Categorical variables are presented as number and percentage, and normally distributed continuous variables are given as mean, standard deviation, and range.
Validity
Construct validity represents the degree to which the scores of a PRO measure are consistent with the scores of another relevant PRO measure. 17,25 The construct validity of the TH-iHOT-33 was examined by testing a priori hypotheses specific to expected associations between the TH-iHOT-33 and the HOOS and EQ-5D-5L (Table 1). The Spearman rank correlation coefficient (r s) was used to assess these associations (0-0.3, negligible correlation; 0.3-0.5, low; 0.5-0.7, moderate; 0.7-0.9, high; 0.9-1.0, very high). 18
A Priori Hypotheses Concerning the Correlations Between the Thai Version of the iHOT-33 and the HOOS and the EQ-5D-5L a

a ADL, activities of daily living; EQ-5D-5L, European Quality of Life–5 Dimensions–5 Levels; HOOS, Hip disability and Osteoarthritis Outcome Score; iHOT-33, International Hip Outcome Tool; QoL, quality of life; TH-iHOT-33, Thai version of the International Hip Outcome Tool.
b Values are given as Spearman rank correlation coefficients.
Reliability
Reliability is defined as the degree to which a PRO measure is free from measurement error. 17 Reliability of the TH-iHOT-33 was evaluated in 3 measurement properties: internal consistency, test-retest reliability, and measurement error. 17
Internal consistency represents the degree of interrelatedness among the items in the same domain or questionnaire, thus measuring the same concept. 17,29 The homogeneity of questions was measured by Cronbach alpha coefficient. 16,17 A Cronbach alpha value within the range of 0.70 to 0.95 is considered ideal. 29 A value <0.70 indicates a lack of correlation among items, and a value >0.95 indicates redundancy of questions. 25,29
Test-retest reliability was calculated in a group of patients who had a GPE scale score of –1, 0, or +1 in the second response, which was completed 2 weeks after the first set of questionnaires. 1,26,29 Intraclass correlation coefficient (ICC; 2-way random-effects model) was used to measure test-retest reliability. An ICC value ≥0.70 indicates high reliability in a sample size of at least 50 patients. 29
Measurement error was evaluated by the standard error of measurement (SEM), which was converted to the smallest detectable change (SDC).
16
The SEM was calculated using the formula
Floor and Ceiling Effects
Floor or ceiling effects were considered significant if >15% of patients had the lowest or highest possible scores, respectively. 29 These effects indicate limitations of the questionnaire in terms of its content validity, reliability, and responsiveness. 29
Results
Translation and Cross-Cultural Adaptation
The iHOT-33 was successfully translated from the original version into the Thai version. During the translation process, none of the items or responses in the questionnaire required cultural adaptation.
Patient Characteristics and Generalizability
From August 2018 to September 2020, a total of 72 patients with hip disorders completed the TH-iHOT-33 questionnaire twice, 2 weeks apart. The demographic and clinical characteristics of study patients are shown in Table 2. In the first administration, the TH-iHOT-33 scores ranged from 13.6 to 95.3. The distribution of scores is shown in Table 3. In the second administration, 53 patients (73.6%) had a GPE scale ranging from –1 to +1. The TH-iHOT-33 scores of this group were used to assess test-retest reliability. Concerning the GPE scale, 3 patients (4.2%) scored less than –1, and 16 patients (22.2%) scored higher than +1.
Demographic and Clinical Characteristics (N = 72) a

a BMI, body mass index; FAI, femoroacetabular impingement.
Distribution of Scores, Floor Effects, and Ceiling Effects of the TH-iHOT-33 (N = 72) a
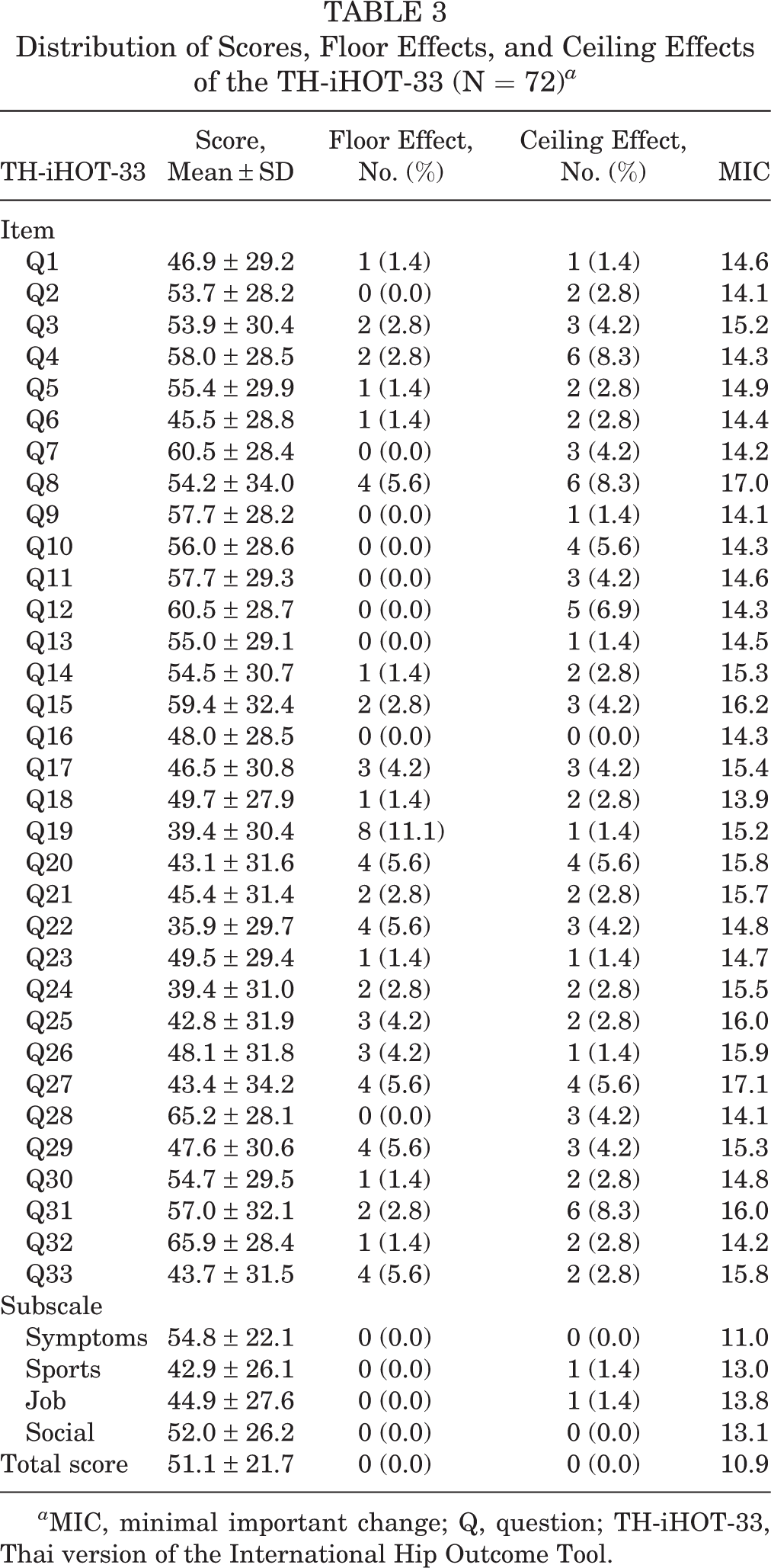
a MIC, minimal important change; Q, question; TH-iHOT-33, Thai version of the International Hip Outcome Tool.
Some items of the iHOT-33 contained the option “I do not do this” or “This is not relevant to me.” These answers were considered missing values that could be omitted, and the total score was calculated from the remaining answers. 15 Missing values, as defined by this reason, were found in 313 (6.6%) of 4752 items. Twelve patients (16.7%) reported that they did not work, so they skipped the job-related concerns section. Two of those patients did not work as a result of their hip pathology, and the other 10 cited reasons other than hip pathology for why they were unemployed. Eight patients in this group were excluded from assessment of test-retest reliability of the job-related concerns subscale.
Validity
The Spearman rank correlation coefficients among the TH-iHOT-33, the Thai version of the HOOS, and the Thai version of the EQ-5D-5L are presented in Table 1. The TH-iHOT-33 had strong correlation with the HOOS total score and the EQ-5D-5L. Seven of the a priori hypotheses were tested, and 6 were confirmed (86.0%).
Reliability
A Cronbach alpha of 0.98 (95% CI, 0.97-0.99) demonstrated excellent internal consistency for the TH-iHOT-33. The Cronbach alpha for each subscale was also excellent, with a range from 0.91 to 0.95. The results of test-retest reliability measures are shown in Table 4. The ICC value for the TH-iHOT-33 was 0.83 (95% CI, 0.73-0.90), which indicated high test-retest reliability. The SEM was 5.1 points, and the SDCs at the individual and group levels were 14.2 and 1.9 points, respectively. The MIC of the TH-iHOT-33 was 10.9 points (Table 3). A Bland-Altman plot of the difference between the first and second administration of the TH-iHOT-33 is shown in Figure 1.
Test-Retest Reliability of the TH-iHOT-33 (n = 53) a

a ICC, intraclass correlation coefficient; SDCgrp, smallest detectable change at the group level; SDCind, smallest detectable change at the individual level; SEM, standard error of measurement; TH-iHOT-33, Thai version of the International Hip Outcome Tool.

Bland-Altman plot to evaluate the test-retest reliability of the Thai version of the International Hip Outcome Tool (TH-iHOT-33). The dashed green lines indicate 95% CI of mean of difference.
Floor and Ceiling Effects
There were no patients who scored the lowest or highest possible score of the TH-iHOT-33. Therefore, this questionnaire demonstrated no floor or ceiling effects. The floor and ceiling effects of each item and subscale were also evaluated (Table 3). Among the 33 questions, some floor and ceiling effects were identified, but none were seen in >15% of the participants.
Discussion
In this study, the TH-iHOT-33 was developed and the psychometric properties were assessed. The questionnaire was successfully translated into the Thai language using the international guidelines of the process of cross-cultural adaptation of self-report measures. The psychometric properties showed that the TH-iHOT-33 is a valid, internally consistent, and reliable measurement tool for evaluating young to middle-aged physically active Thai patients with hip disorders.
The iHOT-33 is a PRO measure that was developed for assessing the functional status and health-related QoL of young to middle-aged physically active patients with hip pathology. 15 The iHOT-33 shows good content validity because orthopaedic surgeons, physical therapists, and patients were involved in item generation during the initial phase of development. 15,31 In a systematic review that evaluated the clinimetric properties of 9 questionnaires for patients with hip and groin disability, the iHOT-33 was one of the recommended PROs for young to middle-aged adults with hip joint–related pain who were undergoing nonsurgical treatment or hip arthroscopy. 31 The International Hip-Related Pain Research Network recently stated that the HAGOS and iHOT questionnaires, the extended and short versions, are the most appropriate PRO measures in young and middle-aged active adults with hip-related pain. 9
International guidelines were followed to translate the original English-language version of the iHOT-33 into Thai, and no cultural adaptation was required for any part of the questionnaire. The target population in this study had selection criteria comparable to those of the target population used to develop and test the original version of the iHOT-33.
Construct validity of the TH-iHOT-33 was determined by comparing it with the HOOS and the EQ-5D-5L. The HOOS was developed to determine outcomes in patients who had hip disability with or without osteoarthritis. 20 The HOOS also demonstrated good psychometric properties that can be used to evaluate patients undergoing hip arthroscopy. 11 The HOOS was used to assess the construct validity of the Dutch version of the iHOT-33. 32 The EQ-5D-5L is a generic self-report questionnaire that consists of 5 questions and 5 levels of answers. The EQ-5D questionnaire was used to validate the German, Chinese, and Dutch versions of the iHOT-33. 1,12,32 In this study, 6 (86%) of the 7 predefined hypotheses were confirmed. This is higher than the minimum requirement (75%) described in the COSMIN checklist, 16 which indicates that the TH-iHOT-33 has good construct validity. Our results revealed that the TH-iHOT-33 has high correlation with the HOOS total score, the HOOS symptoms subscale, the HOOS pain subscale, and the EQ-5D-5L. 18
The TH-iHOT-33 showed excellent internal consistency, with a Cronbach alpha of 0.98. A very high Cronbach alpha (>0.95) suggests likely redundancy of 1 or more items and is usually found in questionnaires with a large number of items. 29 The Cronbach alpha values of the iHOT-33 in different languages were also high, with a range within 0.90 to 0.99. 1,12,15,26,32 In addition, the TH-iHOT-33 had high test-retest reliability, with an ICC value of 0.83. This value was higher than that of the original version 15 but lower than in other languages in which the iHOT-33 has been translated. 1,12,26,32 The SEM of the TH-iHOT-33 was 5.1 points. The SEM and SDC values of the TH-iHOT-33 in the present study were comparable to those reported by Kemp et al 11 and Hinman et al. 8
Our analysis revealed that the TH-iHOT-33 had no floor or ceiling effects overall, and each item of the TH-iHOT-33 had a floor or ceiling effect ranging from 0% to <15%. These findings may be the result of the questionnaire’s design, which uses a slash to mark lines. The floor and ceiling effects may be different if a Likert scale was used instead. Tijssen et al 32 validated the Dutch version of the iHOT-33 and found a floor effect in 1 question and a ceiling effect in 2 questions. The MIC of the TH-iHOT-33 was 10.9 points, which was calculated according to the method described by Norman et al. 21 This method was used in other studies 11,32 that translated the iHOT-33. The group-level SDC of the TH-iHOT-33 was 1.9 points, and this value was less than the MIC value. The individual-level SDC was 14.2 points, which was greater than the MIC. These findings suggest that the TH-iHOT-33 is useful for group comparisons but should be used with caution when monitoring the outcomes of a patient over time. 29
Despite the good results concerning the validity and reliability of the TH-iHOT-33 that we observed in this study, there are some study limitations to describe. First, most of the patients who participated in this study had an activity level of 4 on a modified Tegner activity scale, which is the level of recreational sports. Competitive athletes would be expected to have different demands and perspectives relative to their hip problems, and this factor could influence floor and ceiling effects in the TH-iHOT-33 questionnaire. In addition, the calculated MIC values in this study were based on a distribution-based approach. 21 However, there is no recommendation in the COSMIN checklist regarding the estimation of the MIC. 16 Longitudinal studies would help evaluate the responsiveness of this questionnaire by comparing changes between preoperative and different postoperative time points in patients who undergo hip surgery.
Conclusion
The TH-iHOT-33 is a valid and reliable instrument for assessing the functional status and health-related QoL of young to middle-aged physically active Thai adults with hip disorders.
Footnotes
Acknowledgment
The authors gratefully acknowledge the original authors of the iHOT-33 for granting permission to translate the English version into Thai and Wacharapol Tepa and Narumol Sudjai for data collection and statistical analysis.
Final revision submitted April 21, 2021; accepted June 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by a research grant (R016132035) from the Faculty of Medicine, Siriraj Hospital, Mahidol University. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Siriraj Hospital Institutional Review Board, No. 339/2561(EC4).