
Abstract
Background:
Evaluation of meniscal healing status after repair is important, as it allows the surgeon to inform patients whether they can increase their activities or return to sports.
Purpose:
To identify the healing rates after arthroscopic repair of meniscal tears via second-look arthroscopic evaluation.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Searches of PubMed, Embase, Scopus, and the Cochrane databases were conducted to identify relevant studies published before June 1, 2020. Studies were eligible for this meta-analysis if they provided data regarding healing status of the meniscus at second-look arthroscopy. Random-effects meta-analyses were generated to provide pooled meniscal healing estimates. We further performed subgroup analysis to investigate the healing rates of the meniscus under different situations.
Results:
A total of 41 studies with 1908 individuals were included in the study. The pooled analysis showed the complete healing rate was 74% (95% confidence interval [CI], 67%-80%), the partial healing rate was 10% (95% CI, 6%-16%), and the failure rate was 12% (95% CI, 10%-15%) for arthroscopic repair of meniscal tears via second-look arthroscopic evaluation. Sensitivity analysis demonstrated that no individual study affected the overall healing rate by >1%. Subgroup analysis found higher meniscal healing rates in patients with the following characteristics: age <40 years, male, body mass index <26, red-red tear location, tear in posterior horn, vertical tear, outside-in technique, repair concomitant with anterior cruciate ligament reconstruction, weight-restricted rehabilitation, and time interval from meniscal repair to second-look arthroscopy >12 months.
Conclusion:
In this systematic review, the complete healing rate was 74%, the partial healing rate was 10%, and the failure rate was 12% for arthroscopic repair of meniscal tears via second-look arthroscopic evaluation.
The meniscus protects the joint cartilage and plays an important role in joint stability through axial load distribution, shock absorption, and load bearing. The poor long-term outcomes after meniscectomy have been well documented. 6 The extent of resection relates to the degree of radiologic osteoarthritis, 19 whereas meniscal repair could lead to significantly less arthritis progression and subsequent knee arthroplasty compared with nonoperative management and partial meniscectomy. 10,50 As a result, it is important to preserve as much meniscal tissue as possible for patients with meniscal injury; in response, meniscal repair has become the optimal treatment for tears located at the vascular zone. 12
Evaluation of the meniscal healing status after repair is important, as it allows the surgeon to inform patients whether they can increase their activities or return to sports. 46 The main diagnostic methods for a repaired meniscus include second-look arthroscopy, magnetic resonance imaging (MRI), and clinical assessment. In theory, although subjective scores, physical examinations, or patient satisfaction surveys can reflect the healing of the repaired meniscus to a certain extent, they cannot reflect the actual healing status of menisci. Compared with clinical assessment, MRI has been proposed as a better alternative to evaluate the repaired meniscus. 4,16 However, MRI is less reliable in the postoperative evaluation of meniscal repair, as the scar at the repaired site frequently expresses a grade 3 signal that has been seen as evidence of an unhealed meniscus. 41 In second-look arthroscopy, the situation is directly viewed and evaluated, so the actual healing status after meniscal repair can be objectively judged. One study found that second-look arthroscopy was the most conclusive and accurate evaluating method for repaired meniscus compared with MRI and clinical assessment. 41 However, because second-look arthroscopy is invasive and has certain surgical risks, few patients would choose to undergo second-look arthroscopy. 4
Although multiple previous studies have evaluated clinical results following meniscal repair, less is known regarding meniscal healing rates at second-look arthroscopy. As a result, we conducted a systematic review and meta-analysis to identify the healing rates after arthroscopic repair of meniscal tears via second-look arthroscopic evaluation. It was hypothesized that patients with younger age, lower body mass index (BMI), and red-red tear location would have a higher meniscal healing rate.
Methods
This systematic review and meta-analysis was performed and reported according to the Meta-analysis Of Observational Studies in Epidemiology and the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklists. 42,62
Search Strategy and Study Eligibility
Two authors (W.D., X.L.) independently identified studies that reported on the healing status of the meniscus at second-look arthroscopy by systematically searching PubMed (1946 to February 1, 2021), Embase (1974 to June 1, 2020), Scopus (1966 to February 1, 2021), and the Cochrane Library database (2020; Issue 6). For the database searches, terms related to meniscal repair and meniscal suture were combined with those related to second-look arthroscopy without language restriction (full details of the search strategy are provided in Supplemental Table S1, available online). Studies were eligible for this review if they provided data regarding healing status of the meniscus at second-look arthroscopy. References of included studies were screened, and backward citation tracking was performed using Web of Science to identify articles not found in the original literature search. As studies with very small sample sizes are often case reports and do increase the risk of bias, these small sample studies with <5 patients were excluded from this meta-analysis. Studies performing repeat arthroscopy only in patients with persistent symptoms were also excluded. Disagreements on eligibility of full-text articles were resolved by consensus or by discussion with a third reviewer (Y.A.).
Data Extraction
The following information was independently extracted from each article by 2 trained investigators (W.D., J.W.) using a standardized form: first author, year of publication, country, study design, number of participants, meniscal healing rate, patients’ demographics, tear characteristics, meniscal repair methods, adjuvant procedures, and postoperative factors. The primary outcome was meniscal healing rate. The definition of partial healing in the included studies was also extracted and is summarized in Supplemental Table S2 (available online). When studies involved the same population of patients, only the most comprehensive or recent publication was included, with the former taking precedence.
Quality Assessment
In observational studies, the investigator observes individuals without manipulation or intervention. This is in contrast to randomized controlled trials (RCTs), where investigators do intervene and look at the effects of the intervention on an outcome. As the methodologies of these study types are largely different, different quality assessment tools were used for them. The quality of the observational studies was assessed via a modified version of the Newcastle-Ottawa Scale. 61 This scale assesses quality in several domains: sample representativeness and size, comparability, ascertainment of meniscal healing status, and statistical quality; studies are judged to be at low risk or high risk of bias (scoring details are provided in Supplemental Table S3, available online). For RCTs, the Cochrane Risk of Bias tool was used to assess quality, 23 in which each trial is scored as high, low, or unclear risk of bias according to the following domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. All discrepancies were resolved by discussion between 2 reviewers (X.L., X.H.), with the adjudication of a third reviewer (Y.A.).
Data Synthesis
Estimates of meniscal healing rates were calculated by pooling the study-specific estimates with 95% confidence intervals (CIs) using random-effects meta-analyses that accounted for between-study heterogeneity. 11 Heterogeneity across studies was tested by using the I 2 statistic. The I 2 values of 25%, 50%, and 75% were considered to indicate low, moderate, and high heterogeneity, respectively. 22 The influence of individual studies on the overall healing rate was explored by serially excluding each study in a sensitivity analysis. We further performed subgroup analysis to investigate the influence of different factors on the healing rates after meniscal repairs. Based on the previous studies, 20,27,33,45,56,66,71 factors included in subgroup analysis were age, sex, BMI, histologic location of tear, anatomic location of tear, type of tear, side of meniscus, repair methods, repair devices, anterior cruciate ligament (ACL) reconstruction, ACL-insufficient knee, type of rehabilitation after surgery, time interval from meniscal repair to second-look arthroscopy, and study design. In addition, we performed additional analyses regarding healing rate with studies that included patients before and after the study period 2010 to account for the development of new rehabilitation protocols and operative techniques. To perform the subgroup analysis, we split the data of patients into subsets (eg, male and female patients) according to the different factors. Then, pooled analyses were conducted for the subsets of participants. We further investigated potential sources of heterogeneity via metaregression analysis, which attempts to relate differences in effect sizes to study characteristics. Factors examined were patients’ demographics (age, sex, BMI), tear characteristics (histologic location of tear, anatomic location of tear, type of tear, side of meniscus), meniscal repair methods, repair devices, adjuvant procedures (ACL reconstruction [ACLR], ACL-insufficient knee), and other factors (type of rehabilitation after surgery, time interval from meniscal repair to second-look arthroscopy, study design, and study period). Publication bias was assessed by using the Begg and Egger tests. 9,18 All analyses were performed using R Version 3.2.3 (R Foundation for Statistical Computing) and Stata Version 13.1 (StataCorp). Statistical tests were 2-sided and used a significance threshold of P < .05.
Results
Literature Search
In the initial search, we identified 1003 records. To this, we added 2 using reference mining. After examination of the titles and abstracts, there were 117 potentially eligible studies assessed for inclusion. After reviewing the full text, 41 studies were included in the meta-analysis. ∥ The study flow diagram, including the reasons for exclusion of studies, is shown in Figure 1.

Flowchart illustrating the literature search.
Study Characteristics and Quality
The study characteristics are presented in Table 1. These studies were published between 1991 and 2021. The sample size of the studies ranged from 5 to 140, with a total of 1908 individuals. The mean age of the patients ranged from 19 to 58 years. The mean BMI of the patients ranged from 23.6 to 27.1. There were 2 RCTs 5,28 and the remaining studies were observational studies. For the observational studies, 7 were judged to be at low risk of bias, 8,31,41,53,55,63,69 and 32 were judged to be at high risk of bias. ¶ The major weakness of the observational studies was the small sample size; in addition, most of the studies were from a single institution. For the RCTs, 1 was judged to be at low risk of bias, 28 whereas the other was assessed to be at high risk of bias. 5 Results of the quality assessment are provided in Supplemental Table S4 (available online).
Characteristics of the Included Studies a

a NR, not reported.
Overall Meniscal Healing Rate After Repair
Meta-analytic pooling of the complete healing rates of meniscal repairs reported by the 41 studies yielded a summary rate of 74% (1335/1839 knees; 95% CI, 67%-80%), with significant evidence of between-study heterogeneity (I 2 = 88%) (Figure 2). Sensitivity analysis, in which the meta-analysis was serially repeated after exclusion of each study, demonstrated that no individual study affected the overall healing rates by >1% (Supplemental Table S5, available online). In addition, pooling of the partial healing rates of meniscal repairs was 10% (255/1839 knees; 95% CI, 6%-16%; I 2 = 92%) (Figure 3), and failure rate was 12% (249/1839 knees; 95% CI, 10%-15%; I 2 = 62%) (Figure 4).
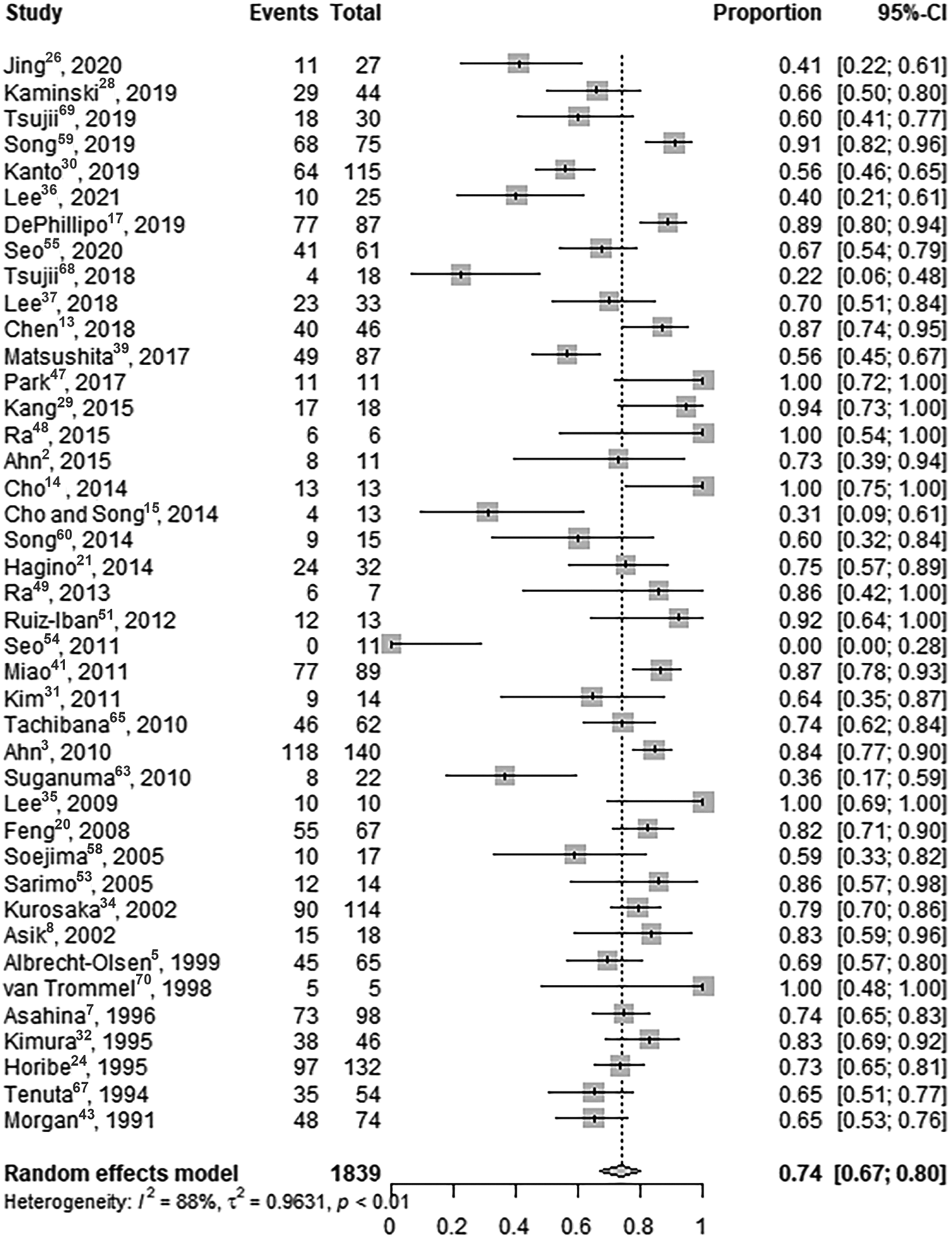
Forest plot of overall complete meniscal healing rate of repaired meniscal tears by second-look arthroscopic evaluation.

Forest plot of overall partial meniscal healing rate of repaired meniscal tears by second-look arthroscopic evaluation.

Forest plot of overall failure rate of repaired meniscal tears by second-look arthroscopic evaluation.
Subgroup Analysis
Table 2 details the complete healing rate, partial healing rate, and failure rate of meniscal repairs under different situations.
Age
All but 1 study 49 reported the age of the patients. When the patients were aged <40 years, the complete healing rate was 75% (1231/1664 knees; 95% CI, 69%-81%; I 2 = 84%), the partial healing rate was 9% (206/1664 knees; 95% CI, 5%-14%; I 2 = 90%), and the failure rate was 13% (227/1664 knees; 95% CI, 10%-16%; I 2 = 63%). When patients were ≥40 years, the complete healing rate was 63% (102/181 knees; 95% CI, 34%-85%; I 2 = 90%), the partial healing rate was 20% (56/181 knees; 95% CI, 6%-49%; I 2 =90%), and the failure rate was 8% (23/181 knees; 95% CI, 3%-18%; I 2 = 59%).
Association Between Factors and Meniscal Healing Rate a
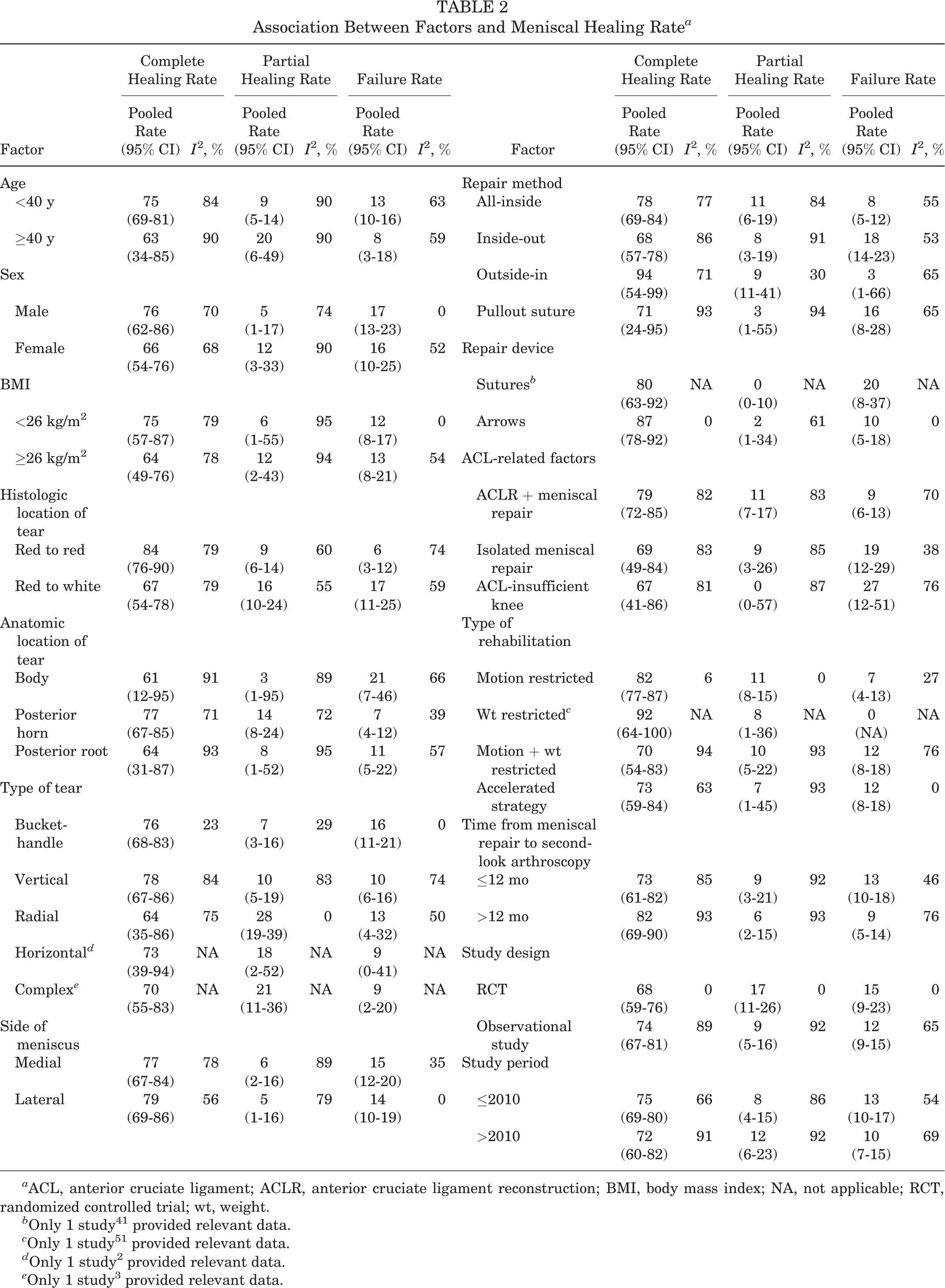
a ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; NA, not applicable; RCT, randomized controlled trial; wt, weight.
b Only 1 study 41 provided relevant data.
c Only 1 study 51 provided relevant data.
d Only 1 study 2 provided relevant data.
e Only 1 study 3 provided relevant data.
Sex
A total of 8 studies 7,15,29,30,37,39,41,65 reported the relationship between sex and meniscal healing rate. In the male patients, the complete healing rate was 76% (168/227 knees; 95% CI, 62%-86%; I 2 = 70%), the partial healing rate was 5% (20/227 knees; 95% CI, 1%-17%; I 2 = 74%), and the failure rate was 17% (39/227 knees; 95% CI, 13%-23%; I 2 = 0%). In the female patients, the complete healing rate was 66% (179/282 knees; 95% CI, 54%-76%; I 2 = 68%), the partial healing rate was 12% (51/282 knees; 95% CI, 3%-33%; I 2 = 90%), and the failure rate was 16% (52/282 knees; 95% CI, 10%-25%; I 2 = 52%).
Body Mass Index
A total of 7 studies 17,28,31,36,37,55,69 reported the BMI of the patients. When the BMI was ≥26, the complete healing rate was 64% (177/260 knees; 95% CI, 49%-76%; I 2 = 78%), the partial healing rate was 12% (47/260 knees; 95% CI, 2%-43%; I 2 = 94%), and the failure rate was 13% (36/260 knees; 95% CI, 8%-21%; I 2 = 54%). When the BMI was <26, the complete healing rate was 75% (136/178 knees; 95% CI, 57%-87%; I 2 = 79%), the partial healing rate was 6% (21/178 knees; 95% CI, 1%-55%; I 2 = 95%), and the failure rate was 12% (21/178 knees; 95% CI, 8%-17%; I 2 = 0%).
Histologic Location of Tear
A total of 15 studies # reported the relationship between tear histologic location and meniscal healing rate. When the tear was located in red-red, the complete healing rate was 84% (448/557 knees; 95% CI, 76%-90%; I 2 = 79%), the partial healing rate was 9% (59/557 knees; 95% CI, 6%-14%; I 2 = 60%), and the failure rate was 6% (50/557 knees; 95% CI, 3%-12%; I 2 = 74%). When the tear was located in red-white, the complete healing rate was 67% (219/345 knees; 95% CI, 54%-78%; I 2 = 79%), the partial healing rate was 16% (61/345 knees; 95% CI, 10%-24%; I 2 = 55%), and the failure rate was 17% (65/345 knees; 95% CI, 11%-25%; I 2 = 59%). None of the studies reported the healing rate when the tear was located in white-white.
Anatomic Location of Tear
A total of 16 studies** reported the relationship between the anatomic location of the tear and meniscal healing rate. When the tear was located in the body of the meniscus, the complete healing rate was 61% (38/56 knees; 95% CI, 12%-95%; I 2 = 91%), the partial healing rate was 3% (7/56 knees; 95% CI, 1%-95%; I 2 = 89%), and the failure rate was 21% (11/56 knees; 95% CI, 7%-46%; I 2 = 66%). When the tear was located in the posterior horn, the complete healing rate was 77% (258/328 knees; 95% CI, 67%-85%; I 2 = 71%), the partial healing rate was 14% (47/328 knees; 95% CI, 8%-24%; I 2 = 72%), and the failure rate was 7% (23/328 knees; 95% CI, 4%-12%; I 2 = 39%). When the tear was located in the posterior root, the complete healing rate was 64% (150/226 knees; 95% CI, 31%-87%; I 2 = 93%), the partial healing rate was 8% (45/226 knees; 95% CI, 1%-52%; I 2 = 95%), and the failure rate was 11% (31/226 knees; 95% CI, 5%-22%; I 2 = 57%).
Type of Tear
A total of 18 studies †† reported the relationship between type of tear and meniscal healing rate. When the tear type was bucket-handle, the complete healing rate was 76% (157/206 knees; 95% CI, 68%-83%; I 2 = 23%), the partial healing rate was 7% (17/206 knees; 95% CI, 3%-16%; I 2 = 29%), and the failure rate was 16% (32/206 knees; 95% CI, 11%-21%; I 2 = 0%). When the tear type was vertical, the complete healing rate was 78% (411/531 knees; 95% CI, 67%-86%; I 2 = 84%), the partial healing rate was 10% (64/531 knees; 95% CI, 5%-19%; I 2 = 83%), and the failure rate was 10% (56/531 knees; 95% CI, 6%-16%; I 2 = 74%). When the tear type was radial, the complete healing rate was 64% (42/75 knees; 95% CI, 35%-86%; I 2 = 75%), the partial healing rate was 28% (21/75 knees; 95% CI, 19%-39%; I 2 = 0%), and the failure rate was 13% (12/75 knees; 95% CI, 4%-32%; I 2 = 50%). Only 1 study reported the healing rate of horizontal tears. 2 When the tear type was a horizontal tear, the complete healing rate was 73% (8/11 knees; 95% CI, 39%-94%), the partial healing rate was 18% (2/11 knees; 95% CI, 2%-52%), and the failure rate was 9% (1/11 knees; 95% CI, 0%-41%) after repair. Only 1 study reported the healing rate of complex tears. 3 When the tear type was a complex tear, the complete healing rate was 70% (33/47 knees; 95% CI, 55%-83%), the partial healing rate was 21% (10/47 knees; 95% CI, 11%-36%), and the failure rate was 9% (4/47 knees; 95% CI, 2%-20%) after repair.
Side of Meniscus
A total of 13 studies ‡‡ reported the relationship between the side of the meniscus and meniscal healing rate. When the tear was located in the medial meniscus, the complete healing rate was 77% (401/552 knees; 95% CI, 67%-84%; I 2 = 78%), the partial healing rate was 6% (60/523 knees; 95% CI, 2%-16%; I 2 = 89%), and the failure rate was 15% (85/523 knees; 95% CI, 12%-20%; I 2 = 35%). When the tear was located in the lateral meniscus, the complete healing rate was 79% (209/272 knees; 95% CI, 69%-86%; I 2 = 56%), the partial healing rate was 5% (24/247 knees; 95% CI, 1%-16%; I 2 = 79%), and the failure rate was 14% (35/247 knees; 95% CI, 10%-19%; I 2 = 0%).
Repair Methods
A total of 37 studies §§ reported the relationship between repair methods and meniscal healing rate. When the repair method was all-inside, the complete healing rate was 78% (506/658 knees; 95% CI, 69%-84%; I 2 = 77%), the partial healing rate was 11% (92/658 knees; 95% CI, 6%-19%; I 2 = 84%), and the failure rate was 8% (60/658 knees; 95% CI, 5%-12%; I 2 = 55%). When the repair method was inside-out, the complete healing rate was 68% (467/652 knees; 95% CI, 57%-78%; I 2 = 86%), the partial healing rate was 8% (74/652 knees; 95% CI, 3%-19%; I 2 = 91%), and the failure rate was 18% (111/652 knees; 95% CI, 14%-23%; I 2 = 53%). When repair method was outside-in, the complete healing rate was 94% (76/103 knees; 95% CI, 54%-99%; I 2 = 71%), the partial healing rate was 9% (15/103 knees; 95% CI, 11%-41%; I 2 = 30%), and the failure rate was 3% (12/103 knees; 95% CI, 1%-66%; I 2 = 65%). When repair method was pullout suture, the complete healing rate was 71% (80/121 knees; 95% CI, 24%-95%; I 2 = 93%), the partial healing rate was 3% (20/121 knees; 95% CI, 1%-55%; I 2 = 94%), and the failure rate was 16% (21/121 knees; 95% CI, 8%-28%; I 2 = 65%).
Repair Devices
Three studies 5,41,53 reported the relationship between repair devices and meniscal healing rates. When the devices were sutures, the complete healing rate was 80% (28/35 knees; 95% CI, 63%-92%), the partial healing rate was 0% (0/35 knees; 95% CI, 0%-10%), and the failure rate was 20% (7/35 knees; 95% CI, 8%-37%). When the devices were arrows, the complete healing rate was 87% (78/90 knees; 95% CI, 78%-92%; I 2 = 0%), the partial healing rate was 2% (3/90 knees; 95% CI, 1%-34%; I 2 = 61%), and the failure rate was 10% (9/90 knees; 95% CI, 5%-18%; I 2 = 0%).
Meniscal Repair With ACLR
A total of 18 studies ∥∥ with 1020 knees reported the healing status of meniscal repair when combined with ACLR. When meniscal repair was combined with ACLR, the complete healing rate was 79% (771/1020 knees; 95% CI, 72%-85%; I 2 = 82%), the partial healing rate was 11% (135/1020 knees; 95% CI, 7%-17%; I 2 = 83%), and the failure rate was 9% (114/1020 knees; 95% CI, 6%-13%; I 2 = 70%).
Healing Rate in Patients With Isolated Meniscal Repair
A total of 13 studies ¶¶ reported the healing status of isolated meniscal repair. Among the 206 knees that underwent isolated meniscal repair, the complete healing rate was 69% (124/206 knees; 95% CI, 49%-84%; I 2 = 83%), the partial healing rate was 9% (38/206 knees; 95% CI, 3%-26%; I 2 = 85%), and the failure rate was 19% (44/206 knees; 95% CI, 12%-29%; I 2 = 38%).
Meniscal Repair in ACL-Insufficient Knees
A total of 4 studies 5,17,32,43 with 155 knees reported the healing rate of meniscal suture in the ACL-insufficient knee. In the ACL-insufficient knee, the complete healing rate of the meniscus was 67% (117/155 knees; 95% CI, 41%-86%; I 2 = 81%), the partial healing rate was 0% (7/155 knees; 95% CI, 0%-57%; I 2 = 87%), and the failure rate was 27% (31/155 knees; 95% CI, 12%-51%; I 2 = 76%).
Type of Rehabilitation After Surgery
A total of 32 studies ## reported the relationship between meniscal healing rate and type of rehabilitation after surgery. When the rehabilitation protocol was motion restricted, the complete healing rate of the meniscus was 82% (210/255 knees; 95% CI, 77%-87%; I 2 = 6%), the partial healing rate was 11% (28/255 knees; 95% CI, 8%-15%; I 2 = 0%), and the failure rate was 7% (17/255 knees; 95% CI, 4%-13%; I 2 = 27%). When the rehabilitation protocol was weight restricted, the complete healing rate was 92% (12/13 knees; 95% CI, 64%-100%), the partial healing rate was 8% (1/13 knees; 95% CI, 1%-36%), and none of the patients in the weight-restricted group had failed meniscal healing at the time of writing. When the rehabilitation protocol was dual restricted (motion and weight restricted), the complete healing rate of the meniscus was 70% (602/853 knees; 95% CI, 54%-83%; I 2 = 94%), the partial healing rate was 10% (131/853 knees; 95% CI, 5%-22%; I 2 = 93%), and the failure rate was 12% (120/853 knees; 95% CI, 8%-18%; I 2 = 76%). When the rehabilitation protocol was an accelerated strategy (both motion and weight were not restricted), the complete healing rate was 73% (138/182 knees; 95% CI, 59%-84%; I 2 = 63%), the partial healing rate was 7% (22/182 knees; 95% CI, 1%-45%; I 2 = 93%), and the failure rate was 12% (22/182 knees; 95% CI, 8%-18%; I 2 = 0%).
Time From Meniscal Repair to Second-Look Arthroscopy
A total of 35 studies a reported the patient’s time interval from meniscal repair to second-look arthroscopy. When the time interval was at most 12 months, the complete healing rate was 73% (487/662 knees; 95% CI, 61%-82%; I 2 = 85%), the partial healing rate was 9% (88/662 knees; 95% CI, 3%-21%; I 2 = 92%), and the failure rate was 13% (87/662 knees; 95% CI, 10%-18%; I 2 = 46%). When the time interval was >12 months, the complete healing rate was 79% (690/925 knees; 95% CI, 67%-87%; I 2 = 91%), the partial healing rate was 7% (111/925 knees; 95% CI, 3%-16%; I 2 = 93%), and the failure rate was 10% (124/925 knees; 95% CI, 7%-15%; I 2 = 72%).
Study Design
There were 2 clinical trials 5,28 and 39 observational studies reporting the meniscal healing status after repair. When the study design was trial, the complete healing rate was 68% (74/109 knees; 95% CI, 59%-76%; I 2 = 0%), the partial healing rate was 17% (19/109 knees; 95% CI, 11%-26%; I 2 = 0%), and the failure rate was 15% (16/109 knees; 95% CI, 9%-23%; I 2 = 0%). When the study design was observational, the complete healing rate was 74% (1261/1730 knees; 95% CI, 67%-81%; I 2 = 89%), the partial healing rate was 9% (236/1730 knees; 95% CI, 5%-16%; I 2 = 92%), and the failure rate was 12% (233/1730 knees; 95% CI, 9%-15%; I 2 = 65%).
Study Period
Among the 41 included studies, when the study period was before or equal to 2010, the complete healing rate was 75% (705/938 knees; 95% CI, 69%-80%; I 2 = 66%), the partial healing rate was 8% (109/938 knees; 95% CI, 4%-15%; I 2 = 86%), and the failure rate was 13% (124/938 knees; 95% CI, 10%-17%; I 2 = 54%). When the study period was after 2010, the complete healing rate was 72% (630/901 knees; 95% CI, 60%-82%; I 2 = 91%), the partial healing rate was 12% (146/901 knees; 95% CI, 6%-23%; I 2 = 92%), and the failure rate was 10% (125/901 knees; 95% CI, 7%-15%; I 2 = 69%).
Metaregression Analysis
In univariate metaregression analysis, the meniscal healing rate was higher in studies with patients aged <40 years than studies with patients aged ≥40 years (P = .029), tears located in red-red were associated with a higher meniscal healing rate than tears located in red-white (P = .026), and the meniscal healing rate was higher in studies with meniscus repaired during ACLR than studies with isolated meniscal repair (P = .029) (Table 3). We did not perform the multivariate metaregression, as there were only 3 studies 7,39,41 containing these 3 factors at the same time.
Univariate Meta-Regression for Complete Healing Rate at Second-Look Arthroscopy a

a ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; RCT, randomized controlled trial; wt, weight.
Publication Bias
The Egger and Begg tests were performed to investigate publication bias. The Egger test indicated no evidence of publication bias (P = .09). Similarly, in the Begg test, there was no evidence of substantial publication bias (P = .27) (Supplemental Figure S1, available online).
Discussion
In our study, the pooled analysis showed that the complete healing rate was 74%, the partial healing rate was 10%, and the failure rate was 12% for arthroscopic repair of meniscal tears via second-look arthroscopic evaluation. Sensitivity analysis demonstrated that no individual study affected the overall healing rate by >1%. Subgroup analysis found higher meniscal healing rates in age <40 years, male, BMI <26, red-red tear location, tear in posterior horn, vertical tear, outside-in technique, repair concomitant with ACLR, weight-restricted rehabilitation, and time interval from meniscal repair to second-look arthroscopy >12 months groups.
A previous study has reported that medial meniscal repairs were significantly more likely to fail than were lateral repairs, when diagnosed via clinical assessment. 38 However, in our study, a similar healing rate was detected between the medial and lateral meniscus. In addition, one of the interesting findings of our study was that compared with healing rates in the bucket-handle tear group, the complete and partial healing rates were higher in the vertical tear group. This difference may be caused by the longer tears and less repair stability of bucket-handle tears. In several studies, horizontal and radial tears have been compared with root tears of the medial meniscus posterior horn in that typical degenerative tears in both share an increased incidence and severity of cartilage degeneration. 64 In our study, the complete healing rate of horizontal tear was 73%, radial tear was 64%, and root tear was 64%. Meniscus protects the articular cartilage from high-contact pressures. This action is dependent on the longitudinal orientation of the intrameniscal circumferential fibers and results in the generation of hoop tension in the meniscus as a vertical load is applied. 1 Regarding the integrity of circumferential fibers in meniscal tears, horizontal tears may be in a better situation than radial and root tears.
The relationship of the ACL and meniscus has been well studied. 40 There are a growing number of studies showing that meniscal tears repaired at the time of ACLR may have an improved healing rate over those repaired in isolation. 52,57 The mechanism behind this phenomenon is still uncertain; in addition, no meta-analysis or systematic review has confirmed it. 44 It has been theorized that the effect is created by augmentation of the repair from the intra-articular release of peptides, growth factors, and mesenchymal pluripotent stem cells from the bone marrow when drilling reconstruction tunnels. 25 In our study, when combined with ACLR, the complete healing rate of the meniscal repair was higher than that of isolated meniscal repair (79% vs 69%).
Current postoperative rehabilitation protocols after meniscal repair vary widely. No consensus exists with regard to the optimal amount of weightbearing, range of motion, or speed at which the patient progresses through the rehabilitation phases. Previous studies have suggested early range of motion and immediate postoperative weightbearing appear to have no detrimental effect on the chances for clinical success after meniscal repair. 46 In our study, when the rehabilitation protocol was weight restricted, the complete healing rate was 92%, which was higher than that for the motion restricted (82%), dual restricted (70%), and accelerated strategy groups (73%). However, this should be interpreted with caution because the rate of the weight-restricted group was only from 1 study. 51
The study had several key strengths. In this study, we used a detailed and robust search strategy that spanned multiple databases and was without language restriction. A detailed assessment of methodological quality of the included studies was performed. We systematically explored for sources of heterogeneity using several study-level characteristics and tested for evidence of effect modification. It should be noted that we chose to focus on healing status at second-look arthroscopy as the main indicator of outcomes after meniscal repair, which have been limitations of previous systematic reviews by use of clinical assessment and MRI. Our results remained robust in sensitivity analysis; in addition, formal testing demonstrated no evidence of publication bias.
This study had several limitations. First, although all studies in this review were appraised for methodological quality, no participants were excluded based on methodological quality as per recommendations of the Cochrane review. 23 The inclusion of lower-quality studies in this meta-analysis may have affected the results of this study. Second, a substantial amount of the heterogeneity among the studies remained unexplained by the variables examined. Unexamined factors, such as the cause of injury, may contribute to the meniscal failure rate. Third, although 41 studies representing 1908 patients were included, several results were based on 1 to 10 studies; as a result, type II statistical error due to an underpowered analysis might have occurred.
Conclusion
In this systematic review, the complete healing rate was 74%, the partial healing rate was 10%, and the failure rate was 12% for arthroscopic repair of meniscal tears via second-look arthroscopic evaluation.
Supplemental Material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211038289.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211038289 - Second-Look Arthroscopic Evaluation of Healing Rates After Arthroscopic Repair of Meniscal Tears: A Systematic Review and Meta-analysis
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211038289 for Second-Look Arthroscopic Evaluation of Healing Rates After Arthroscopic Repair of Meniscal Tears: A Systematic Review and Meta-analysis by Wenli Dai, Xi Leng, Jian Wang, Xiaoqing Hu and Yingfang Ao in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted March 31, 2021; accepted May 19, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.