
Abstract
Background:
As a result of the high physical demand in sport, elite athletes are particularly prone to fifth metatarsal fractures. These injuries are typically managed surgically to avoid high rates of delayed union and allow for quicker return to play (RTP).
Purpose:
To review studies showing clinical and radiographic outcomes, RTP rates, and complication rates after different surgical treatment modalities for fifth metatarsal fractures exclusively in elite-level athletes.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic search was conducted within the PubMed, Scopus, and Cochrane databases from January 2000 to January 2020. Inclusion criteria consisted of clinical outcome studies after operative management of fifth metatarsal fractures in elite athletes. Exclusion criteria consisted of nonoperative management, high school or recreational-level athletic participation, nonclinical studies, expert opinions, and case series with <5 patients.
Results:
A total of 12 studies met inclusion and exclusion criteria, comprising 280 fifth metatarsal fractures treated surgically. Intramedullary screw fixation was the most common fixation construct (47.9%), and some form of intraoperative adjunctive treatment (calcaneal autograft, iliac crest bone graft, bone marrow aspirate concentrate, demineralized bone matrix) was used in 67% of cases. Radiographic union was achieved in 96.7% of fractures regardless of surgical construct used. The overall mean time to union was 9.19 weeks, with RTP at a mean of 11.15 weeks. The overall reported complication rate was 22.5%, with varying severity of complications. Refracture rates were comparable between the different surgical constructs used, and the overall refracture rate was 8.6%.
Conclusion:
Elite athletes appeared to have a high rate of union and reliably returned to the same level of competition after surgical management of fifth metatarsal fractures, irrespective of surgical construct used. Despite this, the overall complication rate was >20%. Specific recommendations for optimal surgical management could not be made based on the heterogeneity of the included studies.
Although the Jones fracture is the most commonly publicized fracture of the fifth metatarsal, the entire bone endures excessive loads during sport. 14,33,42 Acceleration maneuvers and the cumulative effect of bending moments applied to the fifth metatarsal during sport make it particularly vulnerable to injury. 1,13,33 Fifth metatarsal fractures can result in significant disability and can prevent athletic participation. 4,21 The tenuous vascular supply to the fifth metatarsal, specifically at the metadiaphyseal junction, makes these fractures susceptible to delayed healing and nonunion, which can also prolong return to sport. 5,6,37
Several classification systems are used to describe fractures of the fifth metatarsal. Sir Robert Jones first described the “Jones fracture” in a small case series of 4 patients, including himself, as fractures at the metadiaphyseal junction. 19 The Lawrence and Botte 23 classification system is commonly used and holds prognostic value based on fracture zonal distributions. Finally, Torg et al 44 described a classification scheme based on radiographic appearance as it pertains to fracture acuity.
In elite-level athletes, fifth metatarsal fractures at the metadiaphyseal region are often managed surgically to avoid high rates of delayed union or nonunion and allow for quicker return to play (RTP). 5,20,24,35,39 Intramedullary screw fixation is considered the gold standard; however, many different modes of fixation exist. Additionally, augmentation with bone grafting or modern orthobiologics is commonly used to further enhance healing. 9,16,18 –22 Despite good outcomes with surgical management, several potential complications exist, including refracture, nonunion, sural nerve injury, infection, failed fixation, complex regional pain syndrome, and the inability to return to the same level of play. 10,12,22,39,47
Numerous review articles have evaluated nonoperative versus operative management of proximal fifth metatarsal fractures in the general population. 7,39,48 Despite the overwhelming recommendation of surgical management of fifth metatarsal fractures in the athletic population, to our knowledge, no reviews exist that specifically evaluate the current literature as it pertains to operative management of fifth metatarsal fractures solely in elite-level athletes. This systematic review aimed to evaluate outcomes, rates of RTP, and complications after varying surgical treatment modalities for fifth metatarsal fractures in elite athletes.
Methods
Literature Search
A study protocol was developed and registered with the International Prospective Register of Systematic Reviews (PROSPERO, ID Number: CRD42020164648). A systematic search of the current literature was conducted within the PubMed, Scopus, and Cochrane databases using the standardized reporting of systematic reviews by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 31 The databases were searched from January 2000 to January 17, 2020. To identify potentially missed articles, the reference lists of all included articles were hand searched; however, no additional studies were identified.
Eligibility Criteria
All articles pertaining to fifth metatarsal fractures published between January 2000 and January 17, 2020, were eligible for inclusion. Inclusion criteria were as follows: (1) surgical management of fifth metatarsal fractures; (2) elite-level athletes evaluated (defined as collegiate, Olympic, or professional level); (3) clinical or radiographic outcomes reported. Exclusion criteria consisted of nonclinical studies, expert opinions (level 5 studies), case series with <3 patients studies that entailed fifth metatarsal base avulsion fractures, high school or recreational-level athletic participation, and studies that included only nonoperative management. If a study included a nonoperative cohort, this arm of the study was excluded; however, the operative cohort was included if it met the inclusion criteria and was either stratified or controlled for within the results.
Data Extraction and Collection
An initial screening identified 328 studies. Two reviewers (A.C., E.P.B.) independently screened all titles and abstracts, and disagreements were resolved by a third reviewer (W.M.C.). After initial screening, 95 studies were identified for full-text review. Again, two reviewers (A.C., E.P.B.) independently screened all full-text articles, with a third author (W.M.C.) resolving any conflicts.
A total of 12 studies § were included after application of inclusion and exclusion criteria, as outlined in Figure 1. There were 11 level 4 studies and 1 level 3 study. No prospective cohorts or randomized controlled trials were identified for inclusion. Of the 12 studies included, 91.7% were published between 2010 and 2020. The largest study included 73 patients with 75 fifth metatarsal fractures. 27
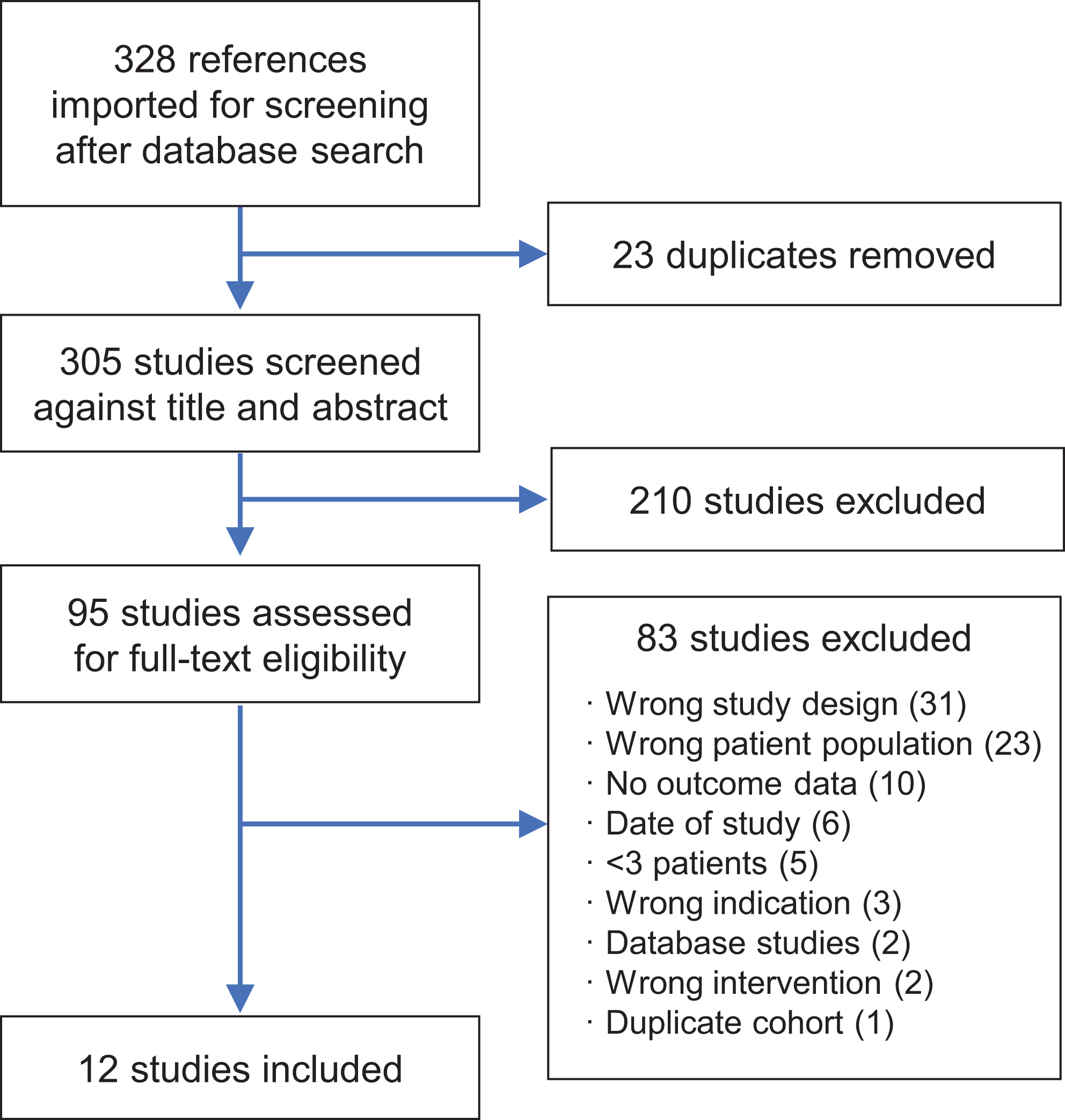
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The following variables were extracted from each study for analysis: study type, level of evidence, patient age, patient sex, sample size, type of sport, level of participation, follow-up duration, surgical intervention, intervention type, adjunctive therapies, fracture type, fracture acuity, rehabilitation course, weightbearing status, complications, clinical time to union, radiographic time to union, and time to RTP. Data were organized into a customized Excel spreadsheet (Microsoft) that was created at the onset of the review process. 15
Data Analysis
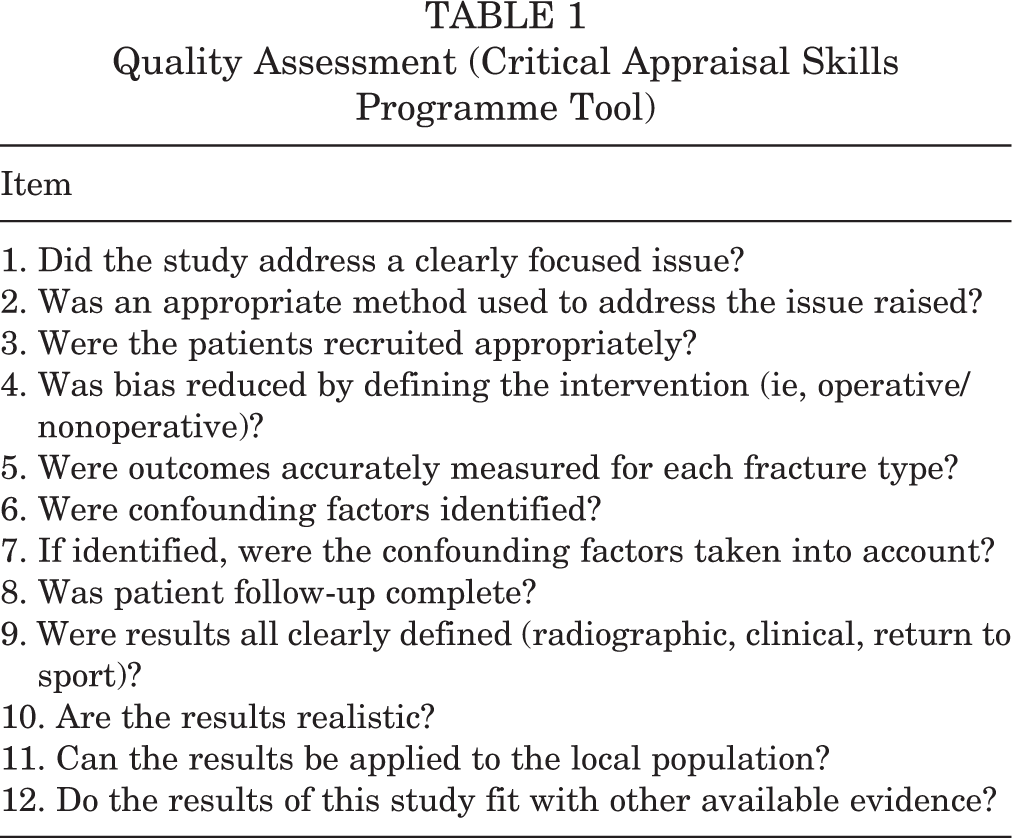
The quality of each article was determined using the Critical Appraisal Skills Programme (CASP) tool. This tool was used previously for a similar study. 39 The CASP tool is designed to assess the quality of a study by using 12 “yes/no” questions, with higher quality studies having more questions with a “yes” response (Table 1). We used this tool to evaluate the available literature regarding the study question. Data were analyzed descriptively through SPSS Statistics (Version 24; IBM Corp) by using frequencies and proportions for categorical variables.
Quality Assessment (Critical Appraisal Skills Programme Tool)
Results
Study Characteristics
The characteristics of the 12 included studies are summarized in Table 2. A total of 278 elite athletes (mean age, 22.3 ± 2.78 years) with 280 fifth metatarsal fractures were included. Male athletes comprised 96.3% of the subjects in the 11 studies that reported patient sex. Based on the Torg classification system and study descriptors, 52.2% of fractures were interpreted as stress fractures (type 2 or 3) and 36.3% were described as acute fractures without prodromal symptoms (type 1). Another 2.9% of fractures were symptomatic nonunions that failed initial nonoperative management before surgeon referral, and 8.6% were refractures previously treated with surgical fixation. Soccer and football athletes comprised 59.3% and 16.2% of the cohort, respectively. The mean follow-up period was 47.2 months across the 7 studies that reported this information.
Characteristics of the Included Studies a
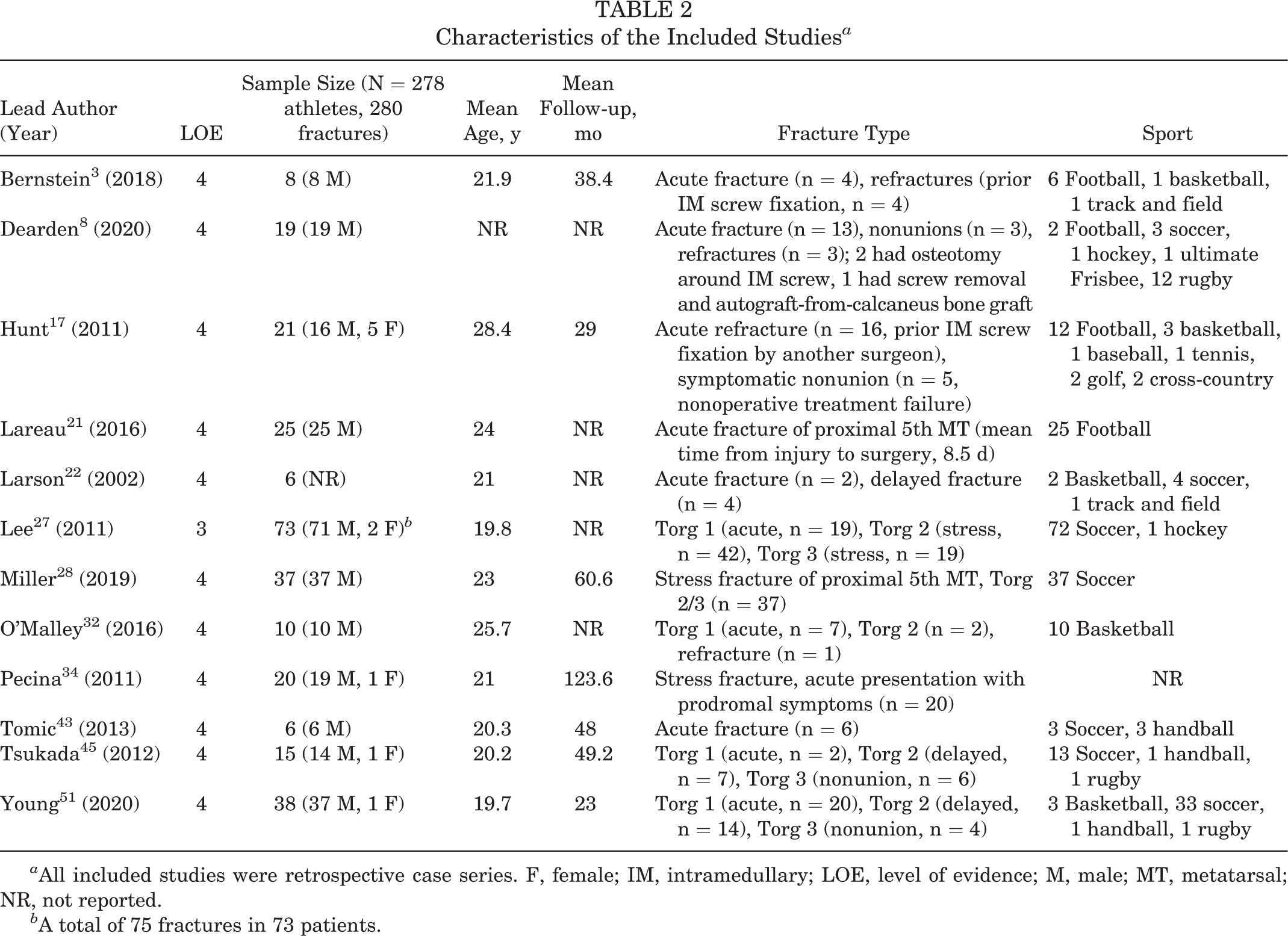
a All included studies were retrospective case series. F, female; IM, intramedullary; LOE, level of evidence; M, male; MT, metatarsal; NR, not reported.
b A total of 75 fractures in 73 patients.
Surgical Interventions and Adjunctive Therapy
Intramedullary screw fixation was the most common method of fixation reported (134/280; 47.9%). Implant types included solid stainless steel screws, cannulated screws, and cannulated titanium cancellous screws. Screw sizes ranged from 4.0 to 6.5 mm, including both fully threaded and partially threaded. Modified tension band wiring was the second most common method of fracture fixation (75/280; 26.8%), although it was used in only 1 study. 27 Other methods of fixation included open reduction and plantar plate fixation (46/280; 16.4%), fifth metatarsal biplanar rotational osteotomy (19/280; 6.8%), and external fixation with an Ilizarov mini fixator (6/280; 2.1%) (Table 3).
Some form of intraoperative adjunctive treatment was used in 67.1% of cases (188/280). Ipsilateral calcaneal autograft was the most common source of bone graft, 3,8,17,27,28,51 followed by iliac crest bone autograft, proximal tibial autograft, and distal tibial autograft. 18,21,22,32,45 Various techniques for bone grafting were used, from minimally invasive subperiosteal injections to open inlay procedures. Only 2 of the included studies 34,43 did not use any form of adjunctive bone grafting, accounting for 26 athletes. Additionally, perioperative vitamin D assessment and supplementation were conducted in only 3 studies. 3,32,51 Bone stimulators were used postoperatively in 3 studies as well. 21,28,32 A summary of the adjunctive therapies used is outlined in Table 3.
Intervention and Adjunctive Treatment a

a DBM, demineralized bone matrix; IM, intramedullary; MT, metatarsal; ORIF, open reduction internal fixation.
b IM screw, 134/280; tension band, 75/280; plantar plate, 46/280; fifth MT osteotomy, 19/280; external fixation, 6/280.
c 188/280 (67.1%) of athletes had intraoperative adjunctive therapy at time of surgery.
Postoperative Protocol
All 12 studies reported on postoperative protocols. A total of 11 studies described an initial period of nonweightbearing postoperatively ranging from 0 to 42 days with a mean of 19 days. One study allowed for immediate partial weightbearing on postoperative day 1, with “progressive weightbearing” if the patient remained clinically asymptomatic. 43 Postoperative rehabilitation protocols are summarized in Table 4.
Postoperative Rehabilitation Protocol a

a CAM, controlled ankle movement; CT, computed tomography; IM, intramedullary; MT, metatarsal; NWB, nonweightbearing; ORIF, open reduction internal fixation; ROM, range of motion; WB, weightbearing.
Outcomes Evaluated
The most common outcome measures evaluated were the presence of radiographic union, time to union, and return to sport. Union, defined as complete bony healing on radiographs or computed tomography (CT) imaging, was achieved in 269 of 280 treated fifth metatarsal fractures (96.7%). Of the 12 studies, 6 used only plain radiographs; the other 6 used either strictly CT or a combination of radiographic and CT imaging based on individualized clinical assessment. Among the 7 studies that reported time to union data, the mean time to union was 9.19 weeks (range, 5.1-30.3 weeks). Among the 11 studies that reported RTP data, the mean time to return was 11.15 weeks (range, 3-40 weeks). In all 12 studies, only 2 athletes were explicitly described as unable to return to the same level of competition. A summary of outcome measures reported in each study is provided in Table 5.
Outcome Measures (Radiographic Union and Return to Play) a
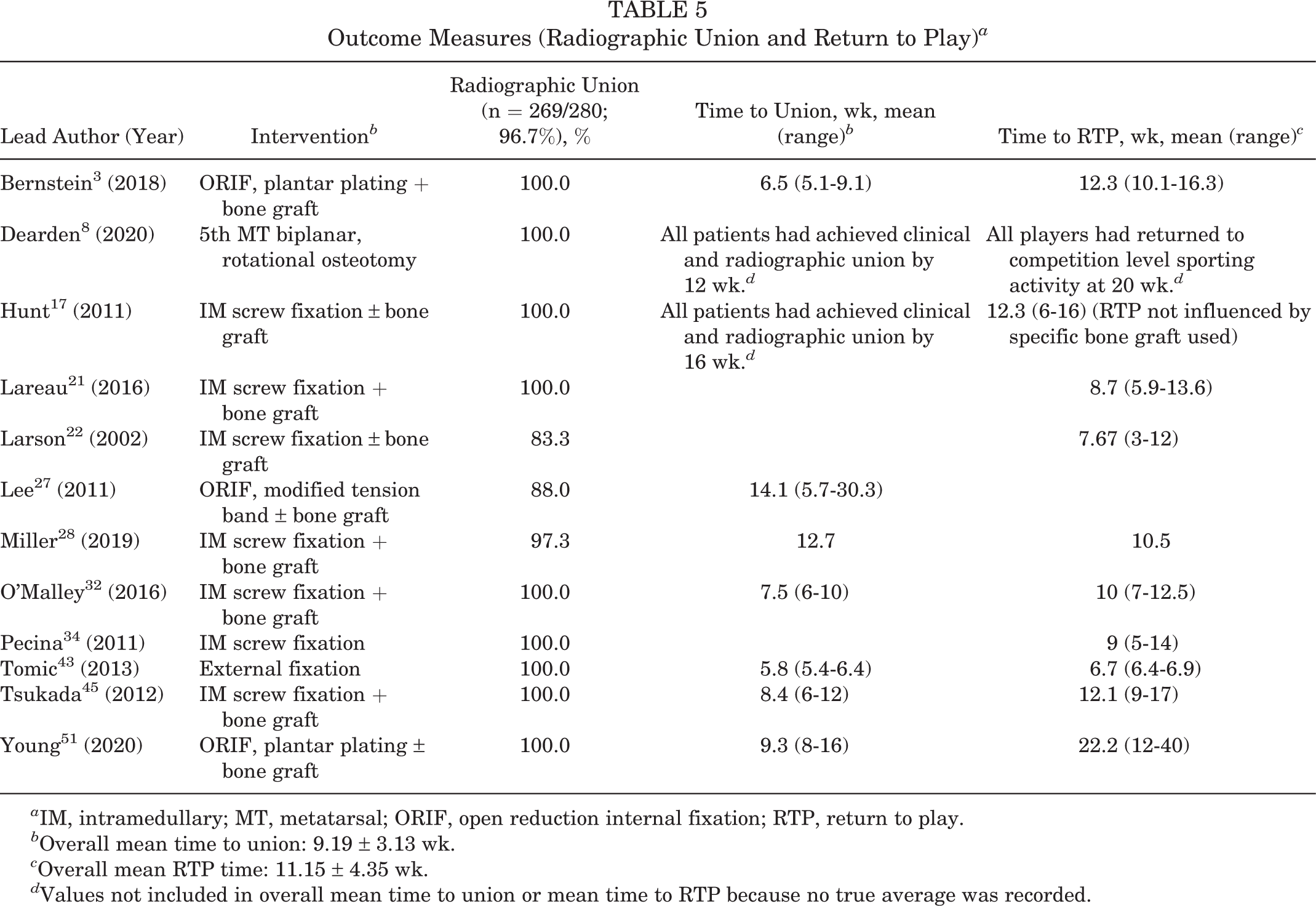
a IM, intramedullary; MT, metatarsal; ORIF, open reduction internal fixation; RTP, return to play.
b Overall mean time to union: 9.19 ± 3.13 wk.
c Overall mean RTP time: 11.15 ± 4.35 wk.
d Values not included in overall mean time to union or mean time to RTP because no true average was recorded.
Complications
A collective 22.5% complication rate was reported across all 12 studies. However, the severity of complications ranged widely. Among all studies, 24 patients experienced a refracture (8.6%). Despite significant variability in the definition of delayed union and nonunion between studies, the combined reported rate of delayed union and nonunion was 6.8% (19/280). Other less commonly reported complications included transient sensory neuropraxias of the sural nerve, superficial skin complications, stress fractures at the screw tip, synostosis of the fourth and fifth metatarsals, and hardware irritation leading to removal of hardware. The complication profile of included studies is provided in Table 6.
Operative Complications a

a IM, intramedullary; MT, metatarsal; ORIF, open reduction internal fixation; PO Abx, oral antibiotics; RTP, return to play.
b Overall complications: transient sensory neurapraxia, n = 3 (1.1% of all cases, 6.5% among plantar plating cases); stress fracture at tip of screw, n = 2 (1.5% among IM screw fixation cases); superficial skin complications, n = 4 (1.4% of all cases); delayed union or nonunion, n = 19 (6.8% of all cases, varying definitions of delayed union and nonunion); refracture, n = 24 (8.6%); synostosis, n = 1 (5.2% among osteotomy cases); hardware prominence, n = 3 (1.1% of all cases); hardware removal following union, n = 9 (3.2% of all cases, 19.6% among plantar plating cases).
Study Quality Assessment
The mean number of “yes” responses on the CASP was 8.42 (range, 6-10) among the studies included. Each study addressed a clearly focused issue with clearly defined, realistic results that fit with other available evidence. As well, the intervention was defined and surgical technique outlined in each included study. The outcome of any fracture could have numerous confounding variables, but these were rarely addressed. Follow-up was highly variable between studies, with 4 of 12 studies (33%) failing to state the mean follow-up duration.
Discussion
High-level athletes represent an exclusive patient population with unique treatment goals and adequate accessibility to resources that may optimize their care. Elite athletes are at particularly high risk for developing fifth metatarsal fracture because of their high activity level and repetitive stresses. This review highlights that the vast majority of elite athletes achieve radiographic union (96.7%) with an overall time to union around 9 weeks, an average RTP time around 11 weeks, and a near 99.9% return to preinjury level of competition after operative management of fifth metatarsal fractures.
Consistent with current literature, intramedullary screw fixation was the most common fixation method used across all studies (47.9%). Previous studies report conflicting data regarding the outcomes of intramedullary screw fixation in athletes. DeLee et al 9 and Porter et al 36 reported a 100% union rate with early return to sport after intramedullary screw fixation. In contrast, Larson et al 22 reported a 40% failure rate with intramedullary screw fixation in their patient cohort, with all but 1 failure occurring in elite athletes. Wright et al 47 reported on 6 refractures in athletes after intramedullary screw fixation, and Hunt and Anderson 17 treated 16 patients who were referred for revision after refracture around a prior intramedullary screw. The current study found a combined 98.5% union rate and a 9.7% refracture rate with the use of intramedullary screw fixation in elite athletes. The screw type and size varied among studies as did the use of adjunctive therapies, which must be considered when interpreting these results. However, much research has been conducted on the biomechanical profile of screw fixation, with no current recommendation regarding optimal screw characteristics, including size, threads, or cannulated versus solid. 12,22,47 Achieving adequate medullary fill while avoiding distal cortical abutment is the most commonly recommended and practiced technique.
Compression plating and tension band wiring allow for direct visualization of the fracture, counter the tensile forces of the lateral and plantar aspect of the fifth metatarsal, provide torsional control, and avoid disruption of the blood supply as the primary nutrient artery to the fifth metatarsal enters from the dorsomedial aspect. 30,51 The present study found comparable rates of refracture for plantar plating (8.7%; 4/46 fractures) compared with reported refracture rates with intramedullary screw fixation. Additionally, Young et al 51 reported a 23.7% rate of hardware removal in a cohort of 38 patients after plantar plating, in which 2 patients reported hardware prominence and 7 preferred plate removal. Lee et al 27 treated 75 patients who had fifth metatarsal fractures by using lateral tension band fixation and achieved 88% radiographic union with a mean time to union of 14.1 weeks. Those investigators used inlay bone graft for 1 patient who experienced a nonunion classified as Torg type 3; otherwise no additional adjunctive treatment was used. The investigators reported an overall refracture rate of 8%. 27
Another alternative fixation strategy is external fixation. Tomic et al 43 reported a case series of 6 elite athletes treated with mini-Ilizarov external fixation. Those authors suggested that external fixation allowed for adjustable distraction and compression at the fracture site, provided biplanar stabilization, and did not disrupt the anatomic integrity of the metatarsal. Tomic et al reported a 100% union rate in their cohort; the mean clinical time to healing was 4.1 weeks, and there was evidence of radiographic consolidation at the fracture site at 5.8 weeks. Return to full athletic activity was reported at an average of 6.7 weeks, with 100% RTP. These findings are substantially better than other documented healing rates and average RTP included in this review. Due to the small sample size of their study population, this may represent type II error, and further adequately powered studies should be conducted to determine the validity of this treatment modality.
Substantial literature has evaluated foot morphological characteristics and their role in altering risk profiles for fifth metatarsal fractures. 14,16,26,36 Studies have found that metatarsus adductus and hindfoot varus may predispose athletes to fifth metatarsal fractures and affect the rate of healing. 38,49,50 Pecina et al 34 performed a computerized pedobarographic analysis on 20 athletes treated for fifth metatarsal fractures and found midfoot varus present in 90% of athletes, causing increased peak pressures on the lateral foot. Lee et al 25 found a correlation between fifth metatarsal curvature and lateral deviation angle with a higher risk of fracture. Dearden et al 8 described an operative technique that addressed fifth metatarsal bony morphology with promising preliminary results, including 100% union rate within 12 weeks of surgery and a 100% rate of RTP before 20 weeks. The authors used a biplanar rotational osteotomy to correct fifth metatarsal curvature with the goal of offloading the proximal fifth metatarsal. Fixation of the osteotomy site requires 2 cortical screws and no additional proximal fixation. 8 Although further research is needed, this method may prove useful when there is concern for intramedullary screw cortical abutment or anatomic variants of the fifth metatarsal, or in the revision setting.
Despite various modes of fixation used, the present study found a large percentage of athletes who went on to radiographic union (96.7%). Diagnosing delayed union and nonunion was challenging, because author definitions varied significantly. Lee et al 27 defined nonunion as no visible radiographic signs of healing by 3 months postoperative, Miller et al 28 defined nonunion as a persistent radiographic fracture line present at 6 months, and Larson et al 22 used a cutoff of 48 weeks to define nonunion. Traditionally, surgeons advocate for evidence of radiographic healing before clearing an athlete for return to sport. 12 In the present review, Miller et al 28 was the only study that reported a mean RTP time (10.5 weeks) that was earlier than the reported mean time to union (12.7 weeks). The subset of patients diagnosed with a delayed union were found to have significantly earlier RTP times (8.6 weeks) compared to the subset of patients who achieved union as expected (11.2 weeks; P = .028). This did not always affect the level of performance, as 1 player who developed a persistent nonunion was pain-free and continued playing professional soccer for several years postoperatively. Watson et al 46 also challenged the traditional nonoperative course of lengthy immobilization and prolonged rehabilitation before RTP. Their cohort of patients consisted of 25 collegiate athletes with proximal fifth metatarsal fractures treated operatively with intramedullary screw fixation who returned to play at an average of 3.6 weeks after surgery based on clinical progression of symptoms as a guide for RTP. Union was achieved in all athletes, and only 1 patient sustained a refracture (4%). Another reported risk factor for nonunion is lateral and plantar gapping at the fracture site. Lee et al 27 highlighted a significant difference between time to union when stratified by a plantar fracture gap >1 mm (<1 mm gap, mean 72.36 days; >1 mm gap, mean 129 days). Those authors recommended an additional plantar bone grafting procedure for Torg type 3 fractures when a plantar gap >1 mm exists.
It is important that surgeons caring for high-level athletes understand management options for refractures, especially given the relatively high rate of occurrence in this population (8.6%). The present review included 4 studies that treated refractures in their initial population. 3,8,17,32 Plantar plating, intramedullary screw fixation, and fifth metatarsal osteotomy were all used in this setting. When exchange intramedullary screw fixation was performed, often the size or length of the screw was altered, and various types of adjunctive therapies were applied. The delivery of the adjunctive therapy varied from injection into the subperiosteal space to open inlay procedures. Hunt and Anderson 17 treated 21 athletes with either refracture (n = 16) or nonunion (n = 5) after failed nonoperative management with intramedullary screw and various adjunctive treatments. The investigators used calcaneal autograft (n = 4), iliac crest bone marrow aspirate (n = 7), demineralized bone matrix (n = 1), iliac crest bone graft with demineralized bone matrix (n = 7), distal tibial autograft with demineralized bone matrix (n = 1), and no bone graft (n = 1) in their patient cohort. They reported a 100% union rate at 4-month follow-up and found no significant difference in RTP rates between the different types of adjunctive therapies used. Understanding management options in the revision setting is important when treating elite athletes, because they experience complications and reinjuries at a higher rate than the normal population.
Adjunctive therapy was commonly used among studies. Intraoperative adjunctive therapy with bone grafting or orthobiologics was used in 67.1% of athletes treated. Only 2 studies included in this review did not use adjunctive treatments. It has become common practice to use bone marrow aspirate concentrate for sports-related fractures in elite-level athletes; however, to our knowledge, no randomized controlled comparative studies have been published on this topic. 29 No clear advantage of using bone graft could be definitively determined in this review due to the heterogeneity of its use. 21,28,32
Literature has been published regarding the use of bone stimulators for lower extremity stress fractures in athletes. Benazzo et al 2 reported an 88% union rate (22/25) for lower extremity stress fractures in athletes at an average of 52 days using an alternating electrical field without operative management. Streit et al 41 performed a small randomized controlled trial involving 8 delayed unions or nonunions of the fifth metatarsal that were treated with active versus inactive pulsed electromagnetic fields (PEMF). The average time to complete radiographic union was 8.9 weeks for the active PEMF group compared with 14.7 weeks for the inactive PEMF group. 41 The effects of bone stimulators on outcomes when used as an adjunct to surgery in elite-level athletes remains largely unknown, and there is no definitive evidence to recommend routine use postoperatively based on this systematic review.
Vitamin D insufficiency in athletes is more common than previously recognized. Vitamin D testing and supplementation of vitamin D were mentioned in only 3 of the included studies. 3,32,51 Fishman et al 11 examined vitamin D levels in professional NBA players and found that nearly 80% of players were either deficient (<20 ng/mL) or insufficient (20-32 ng/mL). Shimasaki et al 40 reported that soccer players with 25(OH)D3 serum levels <20 ng/mL were nearly 3 times as likely to develop a fifth metatarsal stress fracture compared with players who had serum levels >20 ng/mL. We suggest that all high-level athletes treated for fifth metatarsal fracture have vitamin D levels checked and subsequently supplemented at the time of treatment if found to be inadequate. Despite the small amount of existing literature supporting the use of these adjunctive treatments, their low risk profile combined with the potential for improving healing rates may justify their routine use in the treatment of elite athletes.
Several limitations should be considered when interpreting the results of the present review. The search terms used to conduct the literature search could have removed relevant articles inadvertently. A majority of studies included were level 4 observational studies; thus, there is potential risk for biased results. Each included study had inherent flaws and weaknesses that are unavoidable but must be recognized in this review. We attempted to limit selection bias by including studies specifically evaluating elite athletes; however, even within the elite athlete population, there is substantial variation between sports in regard to loading and exertional forces during performance. Selecting only elite athletes limits the generalizability of these results to the general population. Additionally, fracture type and chronicity of fractures varied substantially throughout the review, making direct comparisons difficult. The rate of nonunion was difficult to interpret because there was not a universal definition used in all studies. Because of the limitations listed, the results presented in this systematic review are purely descriptive. Statistical comparative analyses were not performed for this review given the significant heterogeneity of data. Unfortunately, no definitive statements on the optimal treatment protocol can be made based on the results of this study.
Conclusion
Surgical management of fifth metatarsal fractures in elite athletes can be challenging given the physical demands of sport and the desire for quick return to participation combined with an increased risk of nonunion. The goal of this systematic review was to explore surgical outcomes for the management of fifth metatarsal fractures exclusively in the elite athlete population. Surgical constructs used varied greatly between studies; however, outcomes appeared to be similar. Due to the heterogeneity between studies, specific recommendations for optimal surgical treatment of fifth metatarsal fractures in elite athletes are difficult to make. Higher level investigations are required to further evaluate different techniques in order to optimize patient outcomes.
Footnotes
Final revision submitted March 27, 2021; accepted May 3, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.B.G. has received education payments from Medical Device Business Services and Peerless Surgical. W.M.C. has received hospitality payments from Medical Device Business Services. C.E.G. has received research support from Wright Medical; education payments from Arthrex and Peerless Surgical; consulting fees from Medshape; and hospitality payments from Exactech, Integra LifeSciences, Sonoma Orthopedics, and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.