
Abstract
Background:
Both nonoperative and operative treatments have been proposed to manage distal biceps brachii tendon avulsions. However, the advantages and disadvantages of these approaches have not been properly quantified.
Purpose:
To summarize the current literature on both nonoperative and operative approaches for distal biceps brachii tendon ruptures and to quantify results and limitations. The advantages and disadvantages of the different surgical strategies were investigated as well.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic literature search was performed in March 2020 using PubMed Central, Web of Science, Cochrane Library, MEDLINE, Iscrctn.com, clinicaltrials.gov, greylit.org, opengrey.eu, and Scopus literature databases. All human studies evaluating the clinical outcome of nonoperative treatment as well as different surgical techniques were included. The influence of the treatment approach was assessed in terms of the Disabilities of the Arm, Shoulder and Hand (DASH) score and the Mayo Elbow Performance Index; extension, flexion, supination, and pronation range of motion (ROM); and flexion and supination strength ratio between the injured and uninjured arms. Risk of bias and quality of evidence were assessed using the Cochrane guidelines.
Results:
Of 1275 studies, 53 studies (N = 1380 patients) matched the inclusion criteria. The results of the meta-analysis comparing operative versus nonoperative approaches for distal biceps tendon avulsion showed significant differences in favor of surgery in terms of DASH score (P = .02), Mayo Elbow Performance Index (P < .001), flexion strength (94.7% vs 83.0%, respectively; P < .001), and supination strength (89.2% vs 62.6%, respectively; P < .001). The surgical approach presented 10% heterotopic ossifications, 10% transient sensory nerve injuries, 1.6% transient motor nerve injuries, and a 0.1% rate of persistent motorial disorders. Comparison of the different surgical techniques showed similar results for the fixation methods, whereas the single-incision technique led to a better pronation ROM versus the double-incision approach (81.5° vs 76.1°, respectively; P = .01).
Conclusion:
The results of this meta-analysis showed the superiority of surgical management over the nonoperative approach for distal biceps tendon detachment, with superior flexion and supination strength and better patient-reported outcomes. The single-incision surgical approach demonstrated a slightly better pronation ROM compared with the double-incision approach, whereas all fixation methods led to similar outcomes.
Keywords
Distal biceps brachii tendon avulsions are a pathological entity with increasing incidence among the physically active population, with important functional consequences for patients. The incidence of these avulsions in the United States has doubled in recent decades, going from 1.2 cases per 100,000 inhabitants per year in 2002 to 2.5 cases per 100,000 inhabitants in 2010. 43,67 This type of injury is often seen in middle-aged men practicing heavy lifting sports or involved in physically demanding work but can also affect older and less active patients in their everyday life, given that the age of the involved patients ranges from 21 to 70 years. 6,19,56,59 The dominant arm is affected 86% of the time, and patients often have a history of a forced elbow flexion or forearm supination against a considerable resistance, resulting in an eccentric contraction of the biceps tendon. 6 Previous studies have suggested that aside from the acute trauma, a combination of local anatomic factors and tendon degeneration as well as extrinsic factors, such as tobacco smoking and steroid abuse, may be involved. 71
Regardless of the mechanism of failure of the distal biceps brachii tendon, different treatment approaches are available, and the management of these types of injuries is still debated. Both nonoperative and operative treatments are currently proposed as effective management strategies for distal biceps tendon rupture. 6,22 However, the advantages and disadvantages of these approaches have not been properly quantified. Moreover, among the surgical treatments, a debated subject is the choice between the single-incision technique and double-incision technique. 9,13,25 The ideal fixation method (transosseous suture, suture anchors, interference screws, or cortical buttons) has also been debated. In this light, the most suitable management of such lesions remains controversial.
The aim of this meta-analysis was to summarize the present literature and quantify the results and limitations of both nonoperative and operative approaches to address distal biceps brachii tendon lesions. The advantages and disadvantages of the different surgical strategies were investigated as well. The hypothesis was that surgical management would lead to better functional results but a higher rate of complications in comparison with nonoperative protocols.
Methods
Search Strategy and Article Selection
A systematic literature search was performed on March 10, 2020, using MEDLINE, Scopus, PubMed Central, Web of Science, the Cochrane Library, and gray literature databases (isrctn.org, clinicaltrials.gov, greylit.org, and opengrey.eu) using the following string: (distal biceps) AND (rupture OR tear OR avulsion OR detachment). All duplicates were removed, and then all records were checked for eligibility by title and abstract, with full-text reading evaluation when needed. Inclusion and exclusion criteria are reported in Table 1. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were used. 57 The article selection process was independently performed by 2 authors (M.C., D.S.), with disagreement solved by consensus or by the intervention of a third author (E.G.).
Study Inclusion and Exclusion Criteria

Data Extraction, Synthesis, and Measurement of Outcomes
Relevant data from the included articles were independently extracted by 2 authors from the full-text version or supplementary data (M.C., D.S.) using a previously structured table according to Cochrane guidelines. 36 Information on study method concerned the following: level of evidence, study design (power analysis, randomization technique, management of missing data, and protocol deviations), inclusion and exclusion criteria, mechanism of injury, physiotherapy protocol for nonoperative management, distal tendon fixation technique, distal tendon fixation method, time from injury to surgery, other associated surgical treatments, postsurgical rehabilitation, and follow-up length. Patient characteristics and clinical outcomes were also collected: patient sex, age, body mass index, activity level, and associated lesions; preinjury and postintervention clinical scores (Disabilities of the Arm, Shoulder and Hand [DASH] score, Mayo Elbow Performance Index); rate of retears and complications (heterotopic ossification [HO] and nerve injury); time to return to previous activities; evaluation of flexion, extension, supination, and pronation range of motion (ROM); and flexion and supination strength ratio with the uninjured arm. In the study by Klonz et al, 46 patients undergoing both anatomic and nonanatomic fixation were included. Because data to properly analyze nonanatomic fixations were scarce, we decided to include only patients undergoing anatomic surgical reattachment. Missing information was requested by contacting the corresponding authors of the articles in question.
Assessment of Risk of Bias and Quality of Evidence
Reviewers evaluated selected studies using the Downs and Black quality assessment checklist, 23 which can be used to evaluate both randomized and nonrandomized controlled trials (RCTs). The checklist consists of 27 questions, with a total possible score of 28 for randomized studies and 25 for nonrandomized studies. Downs and Black score ranges were given corresponding quality levels according to previous literature: excellent (26-28), good (20-25), fair (15-19), and poor (≤14). Only randomized studies could achieve a quality level of excellent according to the scoring method of the Downs and Black checklist. The overall quality of evidence for each outcome was graded according to the Grading of Recommendations Assessment, Development and Evaluation guidelines. 66
Statistical Analysis
Two different meta-analyses were performed to evaluate the effectiveness of the treatment of distal biceps brachii tendon avulsions: (1) a single-arm meta-analysis including the cohort studies and the separate arms of comparative trials and (2) a meta-analysis including only the comparative trials. Separate analyses were conducted to evaluate the most effective surgical techniques and fixation methods. The random effects model with Knapp-Hartung-Sidik-Jonkman adjustment was used. Results were expressed as raw means in the single-arm meta-analysis or as mean differences [MDs] in the comparative meta-analysis. A meta-analysis of proportions was performed to quantify the prevalence of nerve injuries and HO in patients undergoing surgical reattachment of the distal biceps brachii tendon. The statistical analysis was performed with the meta (V 4.9-7), dmetar (V 0.0.9000), and metafor (V 2.1-0) packages in RStudio (Version 1.2.5019; RStudio). 70 Heterogeneity was tested using the Cochrane Q statistic and I 2 metric 37 and was considered significant when I 2 > 25%. A P value of .05 was set as the level of significance. When data from the same study population were available at different follow-up points or in different studies, data from the last follow-up were selected. When means and standard deviations were not available from the full-text articles, they were estimated from median, range and sample size using the formula proposed by Hozo et al 39 or from median and P values following the Cochrane guidelines, 38 and sensitivity analyses excluding these studies were performed.
Results
Article Selection and Patient Characteristics
The PRISMA flowchart of the article selection procedure is presented in Figure 1. Of the 1275 records extracted, 843 were excluded because they did not assess the desired topic, and another 69 were excluded because of language issues or they did not assess the desired outcomes. A total of 53 studies were considered in the quantitative synthesis.
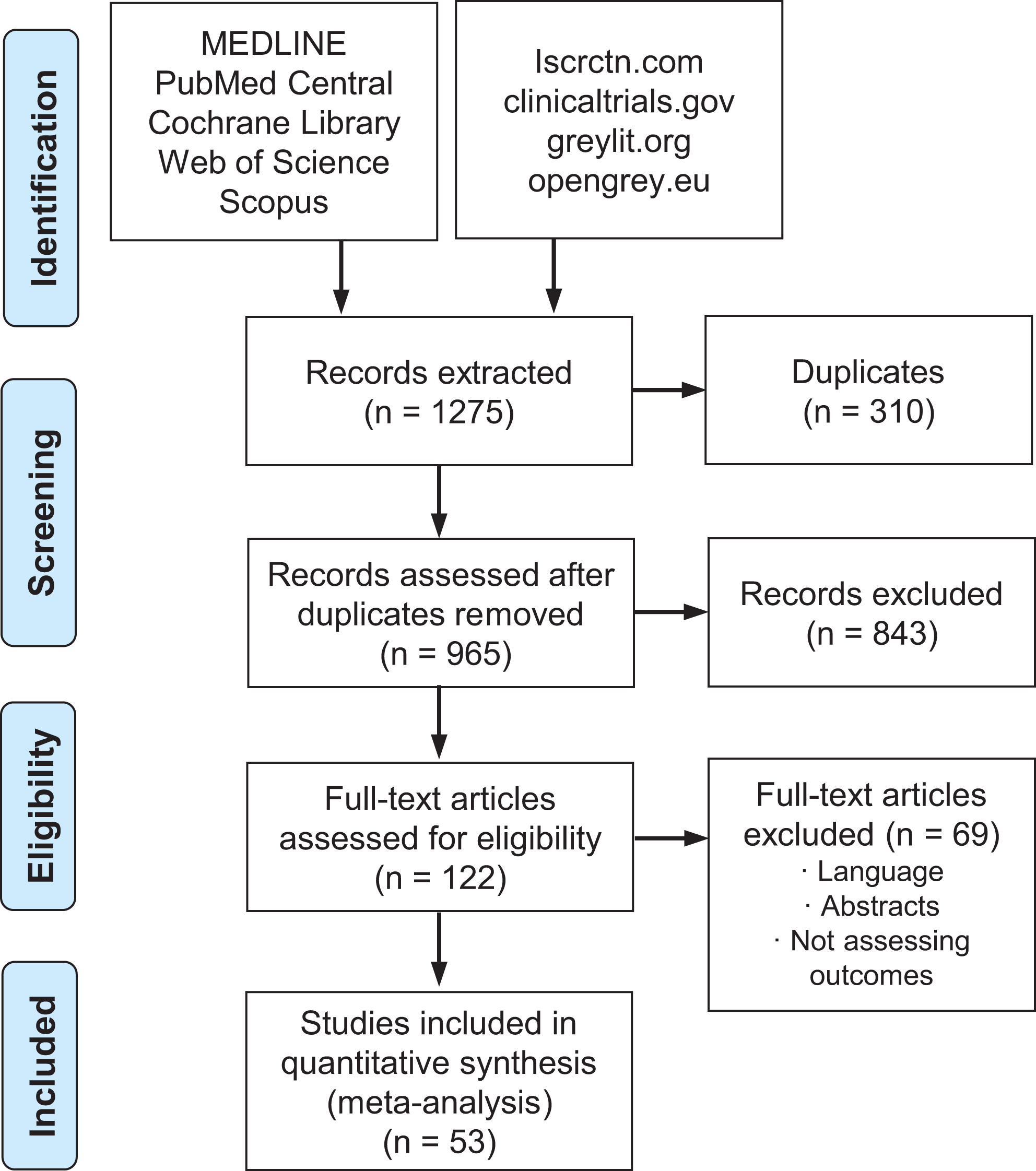
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the article selection process.
Of the included studies, 40 studies were level 4 retrospective case series, 12 studies were level 3 retrospective comparative cohort studies, and 1 study was an RCT. Of the included level 4 case series, 3 studies entailed nonoperative management, 24 studies used a single-incision surgical approach (8 cortical button, 15 suture anchor, 1 transosseous suture), and 13 studies used a double-incision approach (1 suture anchor, 12 transosseous suture). Of the 12 level 3 retrospective comparative cohort studies that were included, 15 study groups opted for a single-incision surgical approach (8 cortical button, 6 suture anchor, 1 transosseous suture), and 8 study groups preferred a double-incision approach (1 cortical button, 3 suture anchor, 4 transosseous suture). Finally, in the only RCT published, a comparison between fixation via a single-incision approach using suture anchors versus fixation via a double-incision approach using transosseous sutures was performed (Figure 2).

Included studies in the surgical group by level of evidence (LOE), technique, and fixation method.
Overall, 1380 patients were included in this meta-analysis: 213 in the nonoperative group and 1167 in the surgical group. Regarding the surgical approach, 708 patients underwent the single-incision technique and 459 patients had the double-incision technique. A total of 276 patients underwent fixation with cortical button, 449 patients with suture anchor, and 383 patients with transosseous suture technique. The mean age was 45.9 years (range, 18-79 years), the male to female ratio was 86:1, and the dominant side was affected in 675 individuals (49%). Patients were evaluated at a mean 32 months of follow-up (range, 3 months—30 years). No significant differences in baseline characteristics (Table 2) of the patients were found between the different treatment options in all included studies. Further details on the selected studies and patients are reported in Appendix Tables A1 and A2.
Baseline Characteristics of the Studies and Patients Included in the Analysis

Meta-analysis Outcomes: Operative vs Nonoperative
The results of the level 4 meta-analysis comparing patients of the 47 studies reporting on a surgical approach versus those of the 6 studies reporting on nonoperative management for distal biceps tendon avulsions showed significant differences in favor of the surgical approach in terms of postoperative DASH score (MD, 8.5; P = .02), Mayo Elbow Performance Index (MD, 7.3; P < .001), and supination (89.3% operative vs 62.7% nonoperative; MD, 26.6; P < .001) and flexion strength (94.7% operative vs 83.0% nonoperative; MD, 11.7; P < .001) ratio with the uninjured limb (Figure 3). No differences were noted in flexion ROM (MD, 12.4; P = .09) or extension ROM deficit at follow-up (MD, 3.4; P = .49). Finally, although no complications, aside from 1 case of significant loss of ROM, were reported for the nonoperative approach, patients in the surgery group sustained nerve injuries, of both motor and sensory nature, and cases of developed HO, sometimes with consequent radioulnar synostoses. In 10% of the patients, a transient sensory disorder was seen, mainly affecting the lateral antebrachial cutaneous nerve and the superficial branch of the radial nerve. This evolved into a persistent deficit in 15% of the cases (1.5% of all included patients). In addition, a transient motor disorder, mainly affecting the posterior interosseous nerve, anterior interosseous nerve, and median nerves, was seen in 1.6% of the surgically treated patients. This transient deficit evolved into a persistent disorder in only 1 case (7.6% of the cases and 0.1% of all included patients). Furthermore, 10% of the surgically managed patients had radiographic evidence of HO, which resulted in a radioulnar synostosis in 4.4% of the cases (0.4% of all the included patients).
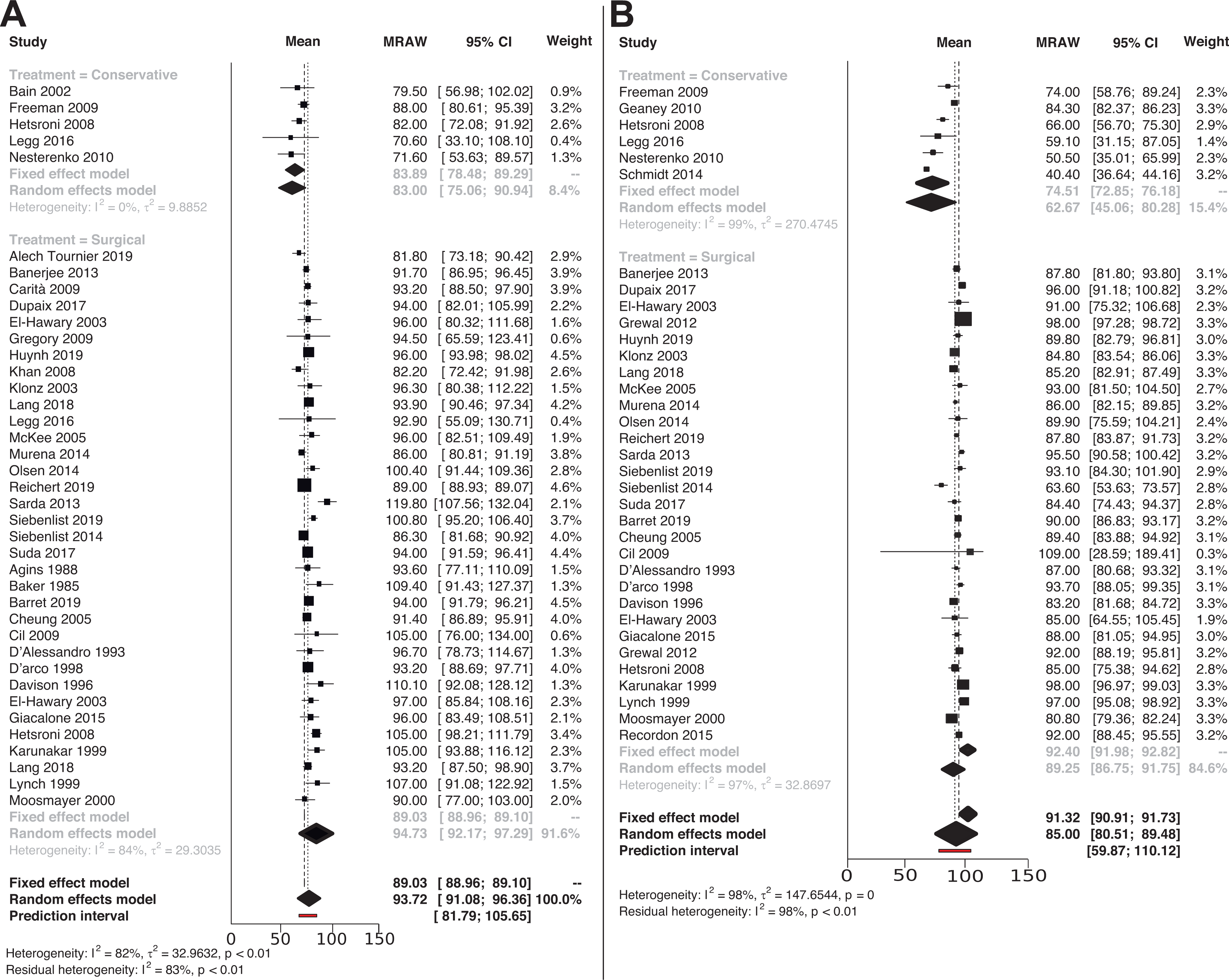
Forest plot for the analysis on (A) flexion strength and (B) supination strength. MRAW, raw mean.
Meta-analysis Outcomes: Single- vs Double-Incision Surgical Approaches
In the level 4 meta-analysis comparing single- and double-incision techniques for the fixation of distal biceps tendon avulsions, 33 studies reported the outcomes of a single-incision approach, whereas 21 studies entailed a double-incision technique. The results showed no differences in terms of DASH (MD, 1.0; P = .9) and Mayo Elbow Performance Index scores (MD, 2.2; P = .31). Regarding ROM evaluation, no differences were noted in flexion (MD, 3.1; P = .5), extension deficit (MD, 0.5; P = .63), and supination ROM (MD, 4.6°; P = .09). Significant differences were found in pronation ROM favoring the single-incision approach (81.5° single incision vs 76.1° double incision; MD, 5.3°; P = .01). The analysis of flexion and supination strength ratio against the uninjured limb did not show any significant difference (flexion strength: MD, 3.5%; P = .1; supination strength: MD, 1.1%; P = .64). The analysis of complication rates in terms of transient sensory nerve injuries (11% vs 5.1% in the single- vs double-incision group, respectively; P = .15) and HO (11% vs 9% in the single- vs double-incision group; P = .08) showed comparable results for both techniques. Given the small number of cases, further comparative meta-analysis was not possible regarding persistent sensory nerve injuries (2.3% vs 0.2% in the single- vs double-incision group), transient motor injuries (1.8% vs 1.2% in the single- vs double-incision group), persistent motor injuries (0.2% vs 0% in the single- vs double-incision group), and radioulnar synostosis (0.4% vs 1.7% in the single- vs double-incision group).
The results of the level 3 meta-analysis, which included only the 6 comparative studies, showed no difference in terms of DASH score (MD, 0.08; P = .6), extension deficit ROM (MD, 0.04; P = .4), and flexion ROM (MD, 0.62; P = .09). Moreover, no differences were seen in the complication rates.
Meta-analysis Outcomes: Surgical Fixation Methods
The level 4 meta-analysis comparing 3 fixation methods for distal biceps tendon avulsion included patients in 18 studies who had surgical fixation with a cortical button, patients in 22 studies who received suture anchors, and patients in 22 studies who received transosseous sutures. The results showed no differences in terms of DASH score (P = .6) and Mayo Elbow Performance Index score (P = .56). Looking at postoperative ROM, we found no significant differences in flexion (P = .5), supination (P = .4), and extension deficit (P = .99), whereas fixation via suture anchors and cortical buttons achieved the best results in terms of pronation ROM (P = .03). Evaluation of the strength ratio with the uninjured limb did not show any significant difference in flexion strength (P = .66) and supination strength (P = .94). The analysis of complication rates showed comparable results for all 3 fixation methods.
The results of the level 3 meta-analysis, which included only the 6 comparative studies, showed no differences in DASH score (P = .36) and extension deficit (P = .97), flexion (P = .33), pronation (P = .51), and supination ROM (P = .74).
Risk of Bias and Quality of Evidence
The risk of bias of the overall analysis was rated “poor” in 29 of the included studies, “fair” in 20 studies, and “good” in 4 studies. In particular, the inclusion of only 1 RCT underlined the limitations of the studies performed to date.
The level of evidence was rated “low” for the DASH score, the evaluation of supination and flexion ROM, and the assessment of supination and flexion strength. The quality of evidence was rated "very low" for the Mayo Elbow Performance Index, pronation ROM and extension deficit evaluations, and the analysis of complication rates. In particular, no level of evidence was downgraded for publication bias or indirectness. Regarding imprecision, there was a downgrade of 1 level for Mayo Elbow Performance Index and for extension deficit. Finally, there was a downgrade of 1 level because of inconsistency for pronation ROM and complication rate analysis.
Discussion
The main finding of this meta-analysis was that the surgical management of a distal biceps tendon avulsion led to significantly better subjective and objective results compared with nonoperative treatment in terms of evaluation of patient-reported outcome measures as well as flexion and supination strength tests. Nevertheless, when clinicians and patients consider surgical rather than nonoperative management of this type of lesion, different aspects need to be considered.
A loss of strength and function inevitably comes alongside nonoperative management, and patients should consider whether they can cope with this loss in their everyday activity level. In this light, for a properly informed decision, it is paramount to quantify this loss. To this aim, the results of this meta-analysis highlighted several interesting findings.
A significant difference favoring operative management was documented not only in terms of a strength evaluation, as could be expected, but also in terms of how patients subjectively perceived the function of their limb. In fact, both the Mayo Elbow Performance Index and the DASH analysis showed statistically significant differences in favor of the surgical approach. The latter reached 8.5 points in favor of surgery, in line with what is considered the minimal clinically important difference (MCID). Still, this finding has to be interpreted with caution because the MCID was intended to be applied to changes in treatment outcome for a single patient rather than group differences. Nonetheless, a difference between groups that almost reaches the MCID should be noted when advising a patient on the choice of one treatment over another. On a functional level, the nonoperative approach led to an almost 20% loss in flexion strength and 40% loss in supination strength, which were significantly lower compared with results obtained after surgery. Accordingly, nonoperative treatment should be recommended mainly to older patients with low demands or to those patients not requiring complete supination strength in their everyday activities.
As well as functional level and the ability to cope with a perceivable deficit, another crucial aspect should be considered when deciding the most suitable treatment option for each patient: the risk of adverse events. This meta-analysis offered important insights on this matter. No complications were reported in the nonoperative group, with the exception of 1 case of significant loss of ROM. In contrast, the operative group was affected by the risks that inevitably accompany a surgical procedure. In 10% of the cases included in the surgical group, transient sensory disorders were noted, mainly affecting the lateral antebrachial cutaneous nerve and the superficial branch of the radial nerve. These evolved into a persistent sensory deficit in 15% of the cases, for a total of 1.5% of all included patients. Transient motor disorders were reported in 1.6% of all surgically treated patients, mainly affecting the posterior interosseous nerve, anterior interosseous nerve, and median nerves; and persistent deficits were rare, being documented in only 0.1% of all included patients.
Other common adverse events were identified radiologically, with evidence of HO reported in 10% of the surgically treated patients. This may lead to ROM limitations, although the evolution of a radioulnar synostosis, causing notable pronosupination limitation, was documented in only 0.4% of the patients. Overall, surgical refixation of a detached distal biceps tendon can be considered safe, as the rate of significant adverse events is quite low. 4 Still, when managing older patients, especially those with challenging lesions with a severely retracted tendon, clinicians should weigh these risks against the expected benefits of an operative procedure to decide whether surgical advantages may exceed the disadvantages or nonoperative treatment is more suitable.
The findings of this meta-analysis pertain specifically to the anatomic reattachment of the distal biceps tendon. 12,50,55 A nonanatomic reinsertion with a brachialis tenodesis has been proposed especially in patients with considerable delay between injury and diagnosis and, most important, when an associated rupture of the lacertus fibrosus is found. This procedure is often performed given the considerable retraction of the tendon and the concomitant disruption of the cubital fossa by scar tissue. Nevertheless, results may be suboptimal, whereas complete restoration of the original strength and ROM can be obtained only via anatomic fixation. 59
Anatomic refixation of the distal biceps tendon can be pursued via 2 surgical techniques: the single-incision technique, originally developed by Dobbie 22 in 1941, or the double-incision technique, initially described by Boyd and Anderson in 1961 9 and later modified by Morrey et al 59 in 1985. The results of the meta-analysis comparing the 2 techniques failed to reveal any difference in terms of patient-reported outcome measures and strength evaluation, thus implying that both approaches are similarly effective in restoring the function of the injured limb. However, a statistical difference in favor of the single-incision technique was documented in the pronation ROM analysis. This finding may be explained by the fact that the dissection of the supinator muscle required by the double-incision approach could result in higher postoperative fibrosis of the muscle itself with consequent lower pronation ROM. Still, the documented difference was limited to a few degrees, which is a questionable limitation in terms of clinically meaningful difference, and was likely not a problem for most patients. In addition, the meta-analysis considering postoperative complications could not point out any significant difference in terms of treatment-related adverse events.
These positive findings confirmed the effectiveness of the modifications applied to the original techniques. In fact, the single-incision approach was historically associated with nerve injuries, but because recent developments in fixation devices limited the need for extensive dissection of the cubital fossa, the rate of permanent and transient nerve injuries is now low. 47 Similarly, the double-incision approach was linked to a large number of HO cases and the risk of consequent radioulnar synostoses. However, these issues were overcome by the modification of the original double-incision technique proposed in 1985 by Morrey et al 59 through the introduction of a muscle-splitting approach. This consisted of a posterior exposure through the extensor carpi ulnaris and the supinator muscle, thus avoiding the need for subperiosteal exposure of the ulna and leading to the low HO rate documented by this literature analysis.
Finally, regarding the debate over the best fixation method, the safety and clinical outcomes of the different devices have been analyzed in several biomechanical studies. Previous evidence pointed out that the cortical button presents superior pullout strength in comparison with the other fixation methods. 44,53 The report by Greenberg et al 30 evidenced that the pullout strength of the cortical button was 3 times greater than that of the transosseous suture and 2 times greater than that of suture anchors. However, this biomechanical superiority did not translate into a clinical difference because the human elbow can generate an eccentric force only up to 200 N, which is below the failure cutoff for all fixation devices (EndoButton, 439.62 N; suture anchor, 381.92 N; bone tunnel, 310.71 N). 30 In fact, no differences could be found in the outcomes evaluated in this meta-analysis with the exception of pronation ROM (in favor of suture anchors and cortical buttons). However, this finding was driven by the surgical approach, as the majority of procedures performed through a single incision used suture anchors and cortical buttons as fixation methods whereas most of the studies that entailed the double-incision technique used transosseous sutures for fixation (Figure 2).
The available literature presented several limitations that were inevitably reflected in this meta-analysis. We identified only 1 published RCT comparing single- vs double-incision techniques; the majority of the literature entailed low-quality studies with a high risk of bias and low to very low evidence. In this light, future research efforts should be focused on RCTs that compare the different approaches, operative versus nonoperative, as well as the different surgical techniques and fixation methods, in order to provide higher quality evidence and minimize the risk of bias. Other surgical options are available, including the use of interference screws and combined fixation devices, which showed promising findings but could not be analyzed because of the small number of reported cases. In addition, rehabilitation protocols were very heterogeneous, going from immediate mobilization with no brace to 6 weeks of restraint in a 90° cast. Moreover, when comparing the reported results, it is important to consider a possible patient selection bias toward different approaches (especially when nonoperative treatment is considered). Finally, the patients’ activity level was not evaluated properly, thus undermining the ability to categorize patients on the basis of their desired limb function.
Nonetheless, the large pool of patients included was homogeneous in terms of age, sex, and time to treatment, which strengthens the results, allowing this meta-analysis to provide an effective and comprehensive overview of the subject. Although further high-level studies should be conducted, the results of this meta-analysis quantified strengths and limitations of the current literature, underlined areas for future research, and offered important elements to guide surgeons and patients in determining the most suitable treatment of distal biceps tendon ruptures.
Conclusion
The results of this meta-analysis documented the superiority of surgical management over a nonoperative approach for distal biceps tendon detachment, with superior flexion and supination strength and better perceived function. The single-incision surgical approach demonstrated a slightly better pronation ROM compared with the double-incision technique, whereas all fixation methods led to similar outcomes. However, the overall low quality of the literature suggests the need for higher level studies to better assess the most suitable strategy to manage distal biceps tendon avulsions.
Footnotes
Final revision submitted May 1, 2021; accepted May 13, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.C. has received grants from Medacta International, Johnson & Johnson, Lima, Zimmer Biomet, and Oped. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Characteristics of the Studies and Patients Included in the Nonoperative Treatment Group a

| Lead Author (Year) | Study Type; LOE | N | Management | Technique | Age, y | Sex | Time to Treatment | Affected Side | Time Immobilized | Follow-up, mo | Postoperative Management | Complications |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Freeman (2009) 26 | Retrospective CS; 4 | 18 | Nonoperative | None | 50 | 16 M 2 F |
None | NR | NR | 59 | Active and passive ROM exercises and strengthening program as tolerated. | 1 significant loss of ROM |
| Geaney (2010) 28 | Retrospective CC; 3 | 10 | Nonoperative, button | Single incision | 48 | 10 M | 2 wk | 4 D 6 ND |
NR | 48 | ROM and strengthening exercises for 2-4 wk. | NR |
| Hetsroni (2008) 35 | Retrospective CC; 3 | 22 | Nonoperative, TO | Single incision | 47 | 22 M | 6 d | NR | 3 wk at 90° | 24 | 90° flexed splint for 2-3 wk. Passive ROM exercises then performed. At 6 wk, active ROM exercises performed. Strengthening commenced at 10-12 wk. In nonoperative group, passive ROM up to 4 wk, then active ROM exercises from 4 to 8 wk. Strengthening allowed at 8 wk postoperatively. | 1 persistent median nerve disorder, 1 HO, 1 transient PIN disorder |
| Legg (2016) 51 | Retrospective CC; 3 | 50 | Nonoperative, button | Single incision | 48 | 40 M | NR | NR | 1 wk at 90° | 32 | 90° flexion backslab cast for 1 wk, after which ROM exercises performed up to 6 wk. Light lifting allowed at 3 mo, and unrestricted weightbearing permitted at 6 mo. | 14 HOs, 2 transient PIN disorders, 8 transient LABCN disorders and loss of extension |
| Nesterenko (2010) 61 | Retrospective CS; 4 | 10 | Nonoperative | None | 48 | 10 M | NR | 5 D 5 ND |
NR | 3 | NR | NR |
| Schmidt (2014) 69 | Retrospective CS; 4 | 22 | Nonoperative | None | 49 | 22 M | NR | 11 D 11 ND |
NR | 1.2 | NR | NR |
a CC, comparative cohort; CS, case series; D, dominant; F, female; LABCN, lateral antebrachial cutaneous nerve; HO, heterotopic ossification; LOE, level of evidence; M, male; ND, nondominant; NR, not reported; PIN, posterior interosseous nerve; ROM, range of motion; TO, transosseous.