
Abstract

This is a case report of a professional Australian rules football player from the Sydney Swans Football Club who experienced a long-term history of left knee pain and swelling and developed focal posterolateral knee pain. The player had a background of previous partial lateral meniscectomy and lateral compartment chondral loss. Over the course of the 2018 season, the player was treated with multiple modalities to maintain his function and capacity to play. Local anesthetic injection into the region of the fabella consistently resulted in complete resolution of pain. Fabellar excision in December 2018 resulted in full functional recovery and return to play by March 2019, as well as increased training tolerance, which continued throughout the 2019 and 2020 seasons. Global positioning system (GPS) measures of total running distance increased by 16% in 2019 (including training and matches). Furthermore, 2-year follow-up data indicated ongoing clinical stability with no games missed because of knee pain and GPS measures of total running distance increasing a further 35% in 2020 (Table 1). Over a 5-year period, this patient underwent 13 magnetic resonance imaging (MRI) scans but had not required any further investigation for >9 months after the fabellar excision, with complete absence of pain or swelling.
Available GPS Data of the Player’s Total Running Distance for Each Season, 2018-2020 a

a GPS, global positioning system; n/a, applicable (not measured).
To our knowledge, this is the only published case of fabellar excision resulting in full return to play in elite Australian Rules football. The case has important implications for the sport and exercise physician who is managing lateral knee osteoarthritis and posterolateral knee pain in the presence of an articulating fabella.
Background
The fabella is an accessory sesamoid bone, present in approximately 17% of the European population 15 and occurring more frequently in Asian populations. 11 It is usually present within the muscle fibers of the lateral head of the gastrocnemius. There is often an articulation with the posterior aspect of the lateral femoral condyle (LFC). 1 Biomechanically, it may have a role in providing pulley-like mechanical advantage to the knee flexors. 10,18 Increased contact pressures between the fabella and femur occur during forced knee extension, consistent with the usual presentation of localized posterolateral knee pain with full extension. 13 However, the fabella also forms part of the posterolateral corner of the knee and may reinforce this part of the knee via associated tensile structures (the fabellofemoral, oblique popliteal, and arcuate ligaments, as well as the lateral head of gastrocnemius tendon). The fabella would theoretically be under more strain with tibiofemoral varus and tibial internal rotation, which may also increase contact forces.
Diagnosis of “fabella syndrome” is often delayed because of its infrequent presentation. Ultrasound can help localize pain to this ossicle, whereas radiography and MRI allow an assessment of any associated pathology in surrounding tissues. Diagnostic perifabellar local anesthetic injection has been suggested to be helpful, 3 although it has not been formally assessed for accuracy. Published case reports have suggested that first line treatment of a painful fabella should involve activity modification, nonsteroidal anti-inflammatory drugs, and a trial of manual therapy. 12,22 Perifabellar local anesthetic and corticosteroid injection may be used for diagnostic and therapeutic purposes. 19 Surgical excision is described as definitive management when these options have failed, with both open and arthroscopically assisted techniques reported. 4,17
There are few published case reports in active participants demonstrating the effectiveness and safety of fabellar excision for the management of focal posterolateral knee pain consistent with symptomatic fabella syndrome. Case reports have described a range of other associated problems, including fracture, chondromalacia, fabellofemoral osteoarthritis, popliteal artery entrapment, dislocation, and snapping, as well as common peroneal nerve palsy. 3 –5 These have all been seen to resolve with fabellar excision.
The higher incidence of fabellas seen in patients with osteoarthritis raises the question of whether this structure is influenced by or influences chondral wear. 16 However, in patients with a fabella, “chondromalacia fabellae” is likely to be a more common cause of posterolateral knee pain, with osteoarthritis of the fabellofemoral articulation occurring in only 1% of cases. 6,9
The unique aspect of this case is the potential positive effects of fabellar excision on the underlying lateral compartment degenerative joint disease in an elite athlete.
Case History
Informed written consent was obtained for access to clinical information, radiological investigation, and clinical and surgical photographs. Approval was granted from the Sydney Swans Football Club.
A 183 cm--tall, right foot—dominant defender experienced chronic left knee lateral compartment issues with intermittent persistent pain and effusions. Knee alignment was neutral with a degree of tibial internal rotation leading to clinical appearance of “in-toeing” but no significant coronal plane malalignment. He had a long-term history of left knee lateral compartment issues stemming from a lateral meniscal tear in 2014 (Figures 1 and 2), requiring repair and subsequent partial meniscectomy in November 2015. After this, he developed an associated LFC chondral lesion that progressed to degenerative change of the lateral compartment. In November 2017, he underwent arthroscopy with chondroplasty of the femoral chondral lesion and removal of chondral debris.

Ultrasound of left knee popliteal fossa during corticosteroid injection, demonstrating the in-plane distal to proximal approach to injection of the fabella, which was the approach for all injections used prior to excision.

Bilateral knee lateral radiographs from 2015 with the enlarged fabella evident at the time on the left knee (arrow).
The athlete returned to full training and preseason games and first noticed the onset of focal posterolateral pain in February 2018. On clinical examination, there was mild effusion, with pain in full knee extension and deep flexion. Using point-of-care ultrasound, direct compression of the fabella against the LFC reproduced pain, which is consistent with the described features of fabella syndrome. 18 Lower limb neurological examination was unremarkable.
He continued to rehabilitate from the chondroplasty with increased running and training loads, as the pain was thought to be related to soft tissue overload. However, owing to continuing posterolateral knee pain, he underwent an ultrasound and computed tomography—guided corticosteroid and local anesthetic injection to the fabellofemoral articulation in March 2018 (Figure 1), which immediately resolved his pain.
His posterolateral knee pain was intermittent and at times impaired his ability to train or play. During a team training session in April 2018, 48 hours prior to a match, he had onset of significant pain and was unable to complete the session. Given the availability, accessibility, and sensitivity, MRI was chosen as the main and initial mode of imaging. He underwent an MRI scan, which demonstrated stable findings consistent with previous MRI scans on file (Figures 3 and 4). The athlete underwent a second ultrasound-guided corticosteroid injection to the fabella and surrounding soft tissues, which again provided immediate relief and lasted 2 weeks.

Magnetic resonance imaging scan of the left knee in September 2015 demonstrating original left femoral condyle chondral injury. The green line indicates the associated region of subchondral bone edema.

Extension of bone marrow edema visualized at the end of the season in August 2017 on sagittal and coronal magnetic resonance imaging scans.
This response conflicted with his MRI scan and radiologist’s report in April 2018 (Figure 5), which disagreed that the findings supported a diagnosis of fabella syndrome, due to the absence of T2 signal hyperintensity within the fabella. However, although bone marrow edema correlates strongly with the presence of pain in knee osteoarthritis, 7 it is not described as a typical feature in symptomatic fabella syndrome. 6,17

Magnetic resonance imaging scan in April 2018, 1 month after the increase in posterolateral left knee pain.
By June 2018, the corresponding LFC showed a large region of bone marrow edema (Figure 6), likely extending from the femoral condylar chondral lesion (initially suspected to be a subchondral fracture). Interestingly, the edema extended most of the way toward the fabella despite an absence of edema within the fabella itself.

Magnetic resonance imaging scan in June 2018 showing recurrent bone marrow edema of the lateral femoral condyle extending more posteriorly on sagittal and axial views. Red dots on the images indicate width and length of the fabella (highlighting tool used by the radiologist).
The patient underwent regular hyaluronic acid viscosupplementation injections into the knee joint in February and April 2018, which seemed to control his general knee pain and effusions but had no specific effect on his posterolateral knee pain. His knee pain and swelling fluctuated through the second half of the year, and he was commenced on a 6-week course of subcutaneous pentosan polysulfate sodium (PPS) in June when his LFC bone marrow edema was seen to be markedly worse. The rationale for the use of PPS was to increase perfusion to subchondral bone as a mild heparinoid. 8
Toward the end of the season, the athlete required weekly local anesthetic injections by the club physician into the fabella prior to matches to be able to compete. At the end of the 2018 season, after a period of 4 weeks rest, he underwent repeat MRI, demonstrating some reduction in the intensity of the bone marrow edema (Figure 7). Arthroscopy with chondroplasty and fabellar excision were undertaken in December 2018 (Figure 8). For direct excision, a longitudinal incision was performed over the palpated fabella. The biceps femoris tendon and common peroneal nerve were both identified, and the common peroneal nerve was mobilized and protected throughout the procedure. The lateral head of the gastrocnemius muscle was incised directly over the enlarged fabella, which was then excised with minimal tissue margins to preserve the tendon. Arthroscopic findings included International Cartilage Regeneration & Joint Preservation Society grade 2 change on the posterior lateral tibial plateau and grade 3 change on the anterolateral femoral condyle. There were grade 2 changes on both the fabella and the femoral articulating surfaces. Fibrocartilaginous ingrowth was noted in the base of the LFC chondral lesion, and limited chondroplasty was performed to stabilize the margins of the lesion.

Magnetic resonance imaging scan from November 2018 showing some reduction in the intensity and size of bone marrow edema.

Intraoperative photograph showing excised fabella via a direct open approach. Note the protected common peroneal nerve.
The athlete had an uncomplicated postoperative recovery and rehabilitation, with return to full training by March 2019 and full competition by April 2019. After the excision, he did not experience any pain or effusions and did not require any oral or injectable medications, all while tolerating increased playing and training loads. After completing 9 rounds of competition, 8 months postoperatively, he sustained a left hamstring muscle strain injury, resulting in his missing 4 matches. Postoperative left knee MRI scans performed in May 2019 and September 2020 are shown in Figures 9 and 10, respectively.

(A) Postoperative magnetic resonance imaging (MRI) scans in May 2019 demonstrating further reduction in bone marrow edema despite greater training and playing loads. Note the absence of the fabella. (B) Postoperative MRI scans in September 2020 demonstrating near-complete resolution of bone marrow edema.

EOS (EOS Imaging) scan measurements demonstrating increased left tibial torsion and marked rotational asymmetry.
Discussion
Fabellofemoral chondromalacia may have been a significant problem for this athlete with a background of lateral compartment chondral loss. The fabella articulating facet and posterior femoral condyle demonstrated features of mild chondral wear on excision. Based on available literature, this issue could have been treated conservatively as “chondromalacia fabellae,” using a combination of activity modification, manual therapy, and proprioceptive therapy. 5,9,22 However, there has been a documented lack of complete resolution in a number of cases. 20 In our experience, the threshold for surgical intervention tends to be lower in professional athletes, who are more likely to choose surgery when there is a higher chance of complete resolution. Although unknown, we theorize that the effectiveness of fabella excision was related to elimination of both compressive overload, as well as localized inflammation of the fabellofemoral joint. The effectiveness of this procedure for such clinically concordant fabellofemoral pain would appear analogous to distal clavicle resection for acromioclavicular joint osteoarthritis or osteolysis, which has a high success rate. 21
It is possible that the lateral compartment degeneration was the underlying cause for the fabellar chondral wear. The fabellofemoral articulation is considered the fourth compartment of the knee. 2 Theoretically, the inflammatory pathology in early knee osteoarthritis will affect all communicating chondral surfaces. Inflammatory cells, mediators, and degradative enzymes may degrade chondral surfaces indiscriminately throughout the knee joint.
Pathomechanics are likely to have contributed to this problem. This athlete had a significant degree of left tibial internal rotation (measured at 34° on EOS scans; EOS Imaging) (Figure 10), although neutral in the coronal plane. Although this alignment imaging was not obtained until after the surgery, his alignment could theoretically have led to increased strain on posterolateral structures, which are required for dynamic control of the more mobile lateral meniscus. The increased fabellar size may have been an adaptive developmental change that eventually led to increased contact forces and pain.
One limitation of this case study is the difficulty in clearly attributing the symptomatic improvement to the surgical excision of the fabella. A number of interventions were undertaken during the course of his management, including activity modification; viscosupplementation; PPS injections; localized fabellar corticosteroid injections; game-day local anesthetic injections; and, of course, the associated chondroplasty (although minimal) at the time of surgery. This chondroplasty alone could be argued to be the reason for his chondral ingrowth and symptomatic improvement. However, the athlete underwent arthroscopic chondroplasty 1 year earlier in a very similar procedure but without fabellectomy. He had a similar rest period of 10 weeks away from running loads. Clearly, his knee pain and function were significantly better after the more recent surgery involving minimal arthroscopic chondroplasty, open fabellectomy, and 10 weeks of rest from running.
Given the paucity of literature on this topic and our findings and results, we offer the following algorithm for clinicians who are presented with a patient who has posterolateral knee pain with clinical suspicion for fabella syndrome: Perform a clinical and (if available) concurrent sonographic examination to determine whether there is focal tenderness over the fabella and whether this is correlated exactly with its location. Obtain MRI scans to assess the presence of any bone marrow edema in the fabella or adjacent femoral condyle. Commence optimal conservative management including avoidance of exacerbating activities (where possible), manual therapy (gentle mediolateral and inferior mobilization of the fabella with lateral gastrocnemius myofascial release) and strengthening of the hamstrings and calves, use of orthoses and footwear optimization, taping strategies, and the use of oral and topical analgesic and anti-inflammatory medications. Consider ultrasound-guided local anesthetic and corticosteroid injection, with care to avoid the common peroneal nerve. Immediately reassess tenderness and relevant pain provocation tests (eg, passive knee extension). Consider further injections if the benefit obtained is not sustained. Escalate to surgical excision if nonoperative treatment fails.
The long-term outcomes of fabellar excision are not well documented in professional athletes. This patient has been counseled regularly and carefully regarding the long-term implications of his continued career in a high-impact sport on his anatomically altered knee. Pre- and postoperative knee flexor strength, as assessed objectively via the NordBord hamstring testing system (Vald Performance), has suggested that while symptomatic preoperatively and for a variable period postoperatively, lasting up to 8 to 12 months, an athlete with fabella syndrome may have a significant side-to-side difference in knee flexor strength, in turn predisposing the athlete to hamstring injury. Indeed, we documented an asymmetry from 0.5% lower on the left side in preseason March 2018 to 17.5% lower on the left side in preseason March 2019 (4 months postoperatively), preceding the hamstring muscle strain that occurred 8 months postoperatively. In season 2020, hamstring strength symmetry appeared to be restored (Table 2). For context, it should be noted that longitudinal studies have found that hamstring injuries are the most frequent and prevalent injury in the Australian Football League. 14 The long-term effects of this surgery on the progression of lateral compartment degenerative joint disease are unknown, but interval postoperative imaging (Figure 9) and assessment during 2-year follow-up did not suggest any significant radiographic or clinical progression since the procedure; indeed, the opposite was appreciated, with stabilization and improvement of the lateral compartment chondropathy.
Hamstring Strength as Measured Via NordBord Testing a
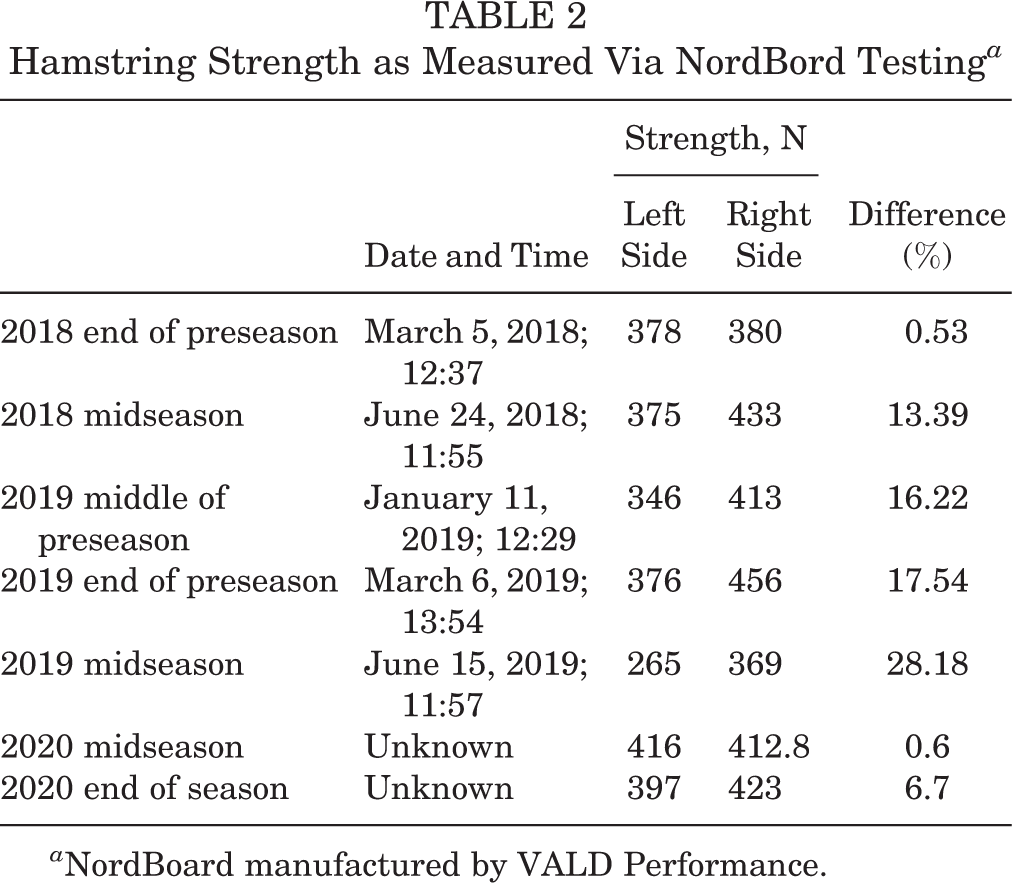
a NordBoard manufactured by VALD Performance.
Conclusion
This case report offers a diagnostic and treatment algorithm suggesting optimal nonsurgical and surgical treatment options and highlights the effectiveness of fabellar excision in an elite athlete with underlying lateral compartment degenerative change to facilitate continuation of performance at an elite level. It addresses considerations in knee-flexor hamstring strength pre- and postoperatively for the clinician, and, most significantly, the study suggests possible longer-term positive effects on the lateral compartment chondral surfaces and, in turn, on symptoms and function, both of which are important considerations in career longevity for elite athletes and their longer-term health.
Footnotes
Acknowledgment
The authors acknowledge the following for their assistance: Sydney Swans Football Club, Mr Zak Jones, Mr Matthew Cameron, Mr Tim Needham, Mr Rob Spurrs, Mr Matt McCutcheon, Dr Phil Lucas, PRP Diagnostic Imaging Moore Park, St Kilda Football Club, Dr Tim Barbour, Mr Daniel Hoffman, and Mr Marcus Krygger.
Final revision submitted January 29, 2021; accepted February 24, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.F. is a paid associate editor for The Orthopaedic Journal of Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.