
Abstract
Background:
Little has been reported in the literature regarding surgical treatment of posterior cruciate ligament (PCL) injuries in pediatric patients.
Purpose/Hypothesis:
The purpose was to evaluate presentation, injury pattern, outcomes, and complications of surgically managed PCL injuries in pediatric patients. It was hypothesized that pediatric patients would have good patient-reported outcomes and no significant radiographic changes or complications.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A literature search was performed using PubMed, Medline, EMBASE, Scopus, and Cochrane databases between 1975 and December 16, 2019. Search terms included “posterior cruciate ligament,” “peel-off injury,” “avulsion,” “PCL,” “pediatric,” “skeletally immature,” and “adolescent.” Included were studies on pediatric patients with PCL injuries managed operatively. Exclusion criteria included case reports, studies not reporting clinical results, reviews, abstract or conference papers, or papers not in the English language. Quality assessment was performed on all included studies using the MINORS (Methodological Index for Non-Randomized Studies) criteria.
Results:
Four articles comprising 43 knees in 42 patients met the criteria and were included. Motor vehicle accidents were the most common mechanism of injury (39.5%; n = 17/43), followed by sports-related injuries (35%; n = 15/43). All studies commented on tear pattern, with the following distribution: 42% (n = 18/43) midsubstance tears, 37% (n = 16/43) tibial avulsions, and 21% (n = 9/43) femoral avulsions. Overall, good patient-reported outcomes (Knee injury and Osteoarthritis Outcome Score and Pediatric International Knee Documentation Committee, Tegner, and Lysholm scores) and return to activity, as well as satisfactory posterior stability (KT-1000 arthrometer, posterior drawer test, and kneeling radiographs) and range of motion, were reported. There was no significant leg-length discrepancy or angular deformity reported. Arthrofibrosis was reported in 7% of postoperative knees and was the most commonly reported complication. Osteoarthritis was reported in 21% (n = 9/43) of knees. The average MINORS score was 7 (range, 6-8) for noncomparative studies and 10 for comparative studies.
Conclusion:
Good patient-reported outcomes and return to activity can be obtained using repair or reconstruction. This evidence was limited by the quality of the included studies and overall small sample size; however, this review serves as a baseline for futures studies on PCL repair/reconstruction in pediatric patients.
Posterior cruciate ligament (PCL) injuries are much less common than are anterior cruciate ligament (ACL) injuries. Because of the relatively uncommon nature of these injuries, the exact incidence is unknown. Fanelli 3 and Fanelli and Edson 4 reported an incidence as high as 38% (n = 85/222) in trauma patients with acute hemarthrosis of the knee. Motor vehicle accidents (MVAs) are the most common mechanism of injury, followed by sports-related injuries in the adult population. 22 Pediatric PCL injuries are even less common than are adult PCL injuries, with most reports in the literature limited to case reports. 1,6,7,9,14,15,19,26,29 The rare occurrence in patients with open physes is due in part to the fact that ligaments are stronger and more resilient than is epiphyseal bone in this population. 2,17
Nonsurgical management is favored in adults with isolated PCL injuries, especially those with grade 1 or 2 injuries. 18,24,25 However, there is concern regarding the long-term outcomes of the PCL-deficient knee. The understanding of the natural history of PCL injuries has advanced, leading to concern about the progression of osteoarthritis in those with persistent laxity. 21,24,25
To our knowledge, no study has organized the available literature to provide a comprehensive review on the treatment options, outcomes, and potential complications of PCL repair or reconstruction in pediatric patients. The primary purpose of the systematic review was to evaluate presentation, injury pattern, outcomes, and complications of surgically managed PCL injuries in pediatric patients. We hypothesized that pediatric patients would have (1) good patient-reported outcomes and (2) no significant radiographic changes or complications. This systematic review serves to summarize the literature on clinical results of different surgical techniques in the treatment of pediatric PCL ruptures. This review can serve as a precursor to prospective database-driven research in operatively treated pediatric PCL injuries.
Methods
We performed this systematic review according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Studies were included if they included pediatric patients undergoing surgery for PCL rupture. Studies were excluded if they were case reports; did not report clinical results; were review articles, abstracts, or conference papers; were not written in the English language. Studies were not limited to isolated PCL injuries.
Information Sources
A search strategy was constructed to retrieve the most relevant yield on surgical outcomes for pediatric PCL ruptures. All searches were conducted between 1975 and December 16, 2019, using PubMed, Medline, EMBASE, Scopus, and Cochrane databases. A combination of keywords, including “truncation,” and indexing terms were used (when available) to combine the 2 concepts of the pediatric PCL rupture and specific surgical procedures, such as “posterior cruciate ligament,” “peel-off injury,” “avulsion,” “PCL,” “pediatric,” “skeletally immature,” and “adolescent.” No filters or limiters were applied. The results were de-duplicated using the Covidence software (Veritas Health Innovation Ltd) and to facilitate and manage the screening and extraction process. See the Appendix, which includes complete search strategies for all the databases (Appedndix 1).
Study Selection and Data Collection
A total of 1723 studies were filtered from all databases. First, all studies were transferred to covidence.org, and 3 authors were granted access to screen the articles (S.Y., N.R.S., M.J.S.). Then, duplicates were removed. This left 850 articles to be screened. Two authors screened abstracts of all articles independently (S.Y. and N.R.S.). Discrepancies between authors were resolved by the senior author (L.D.F.). A total of 49 articles were selected for full-text screening and again were independently screened by 2 authors. Of these, 4 articles were eligible to be included in the study (Figure 1).

STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) diagram of search strategy of this systematic review. PCL, posterior cruciate ligament.
Data Items and Quality Assessment
The extracted data included title of article, author name, name of journal, level of evidence, published year, number of patients, mean age (years), mean follow-up period (months), mechanism of injury, diagnosis, treatment, patient-reported outcomes, clinical outcomes, activity at follow-up, and complications. Descriptive statistics were used to summarize recorded variables. Finally, each study was reviewed according to the MINORS (Methodological Index for Non-Randomized Studies) criteria, which has been shown to be a reliable and valid assessment of reporting quality for comparative and noncomparative studies. A maximum score of 16 is possible for noncomparative studies; 24, for comparative studies. 27
Results
The systematic review search identified 850 potential studies for inclusion. Of these, 801 were excluded based on abstract and title review, leaving 49 for full-text screening. After full-text review, 4 studies 10,11,28,30 remained; the other 45 were excluded for the following reasons: 37 for wrong study design comprising case reports or technique articles; 3, wrong patient population; 2, wrong intervention (no PCL treatment described or performed); 1, full text unavailable (conference proceeding); 1, duplicate manuscript, and 1, not in English.
The included studies reported on a total of 43 surgically treated knees in 42 patients with a mean age of 13 years (range, 4-18 years) at a mean follow-up of 51 months (range, 8.2-144 months). MVAs were the most common mechanism of injury (39.5%; n = 17/43), followed by sports-related injuries (35%; n = 15/43). All studies commented on tear pattern, with the following distribution: 42% (n = 18/43) midsubstance tears, 37% (n = 16/43) tibial avulsions, and 21% (n = 9/43) femoral avulsions. Forty-nine percent (n = 21/43) of knees had isolated PCL tears. Three different surgical techniques were used: repair (44%; n = 19/43), physis-sparing reconstruction (14%; n = 6/43), and transphyseal reconstruction (42%; n = 18/43). Studies describing repair technique reported using it exclusively in cases of avulsion injuries (n = 19/19). Fifteen reconstructions were performed using autograft, while the remaining 9 were performed using allograft (Table 1).
Summary of Included Studies on Pediatric PCL Injury a
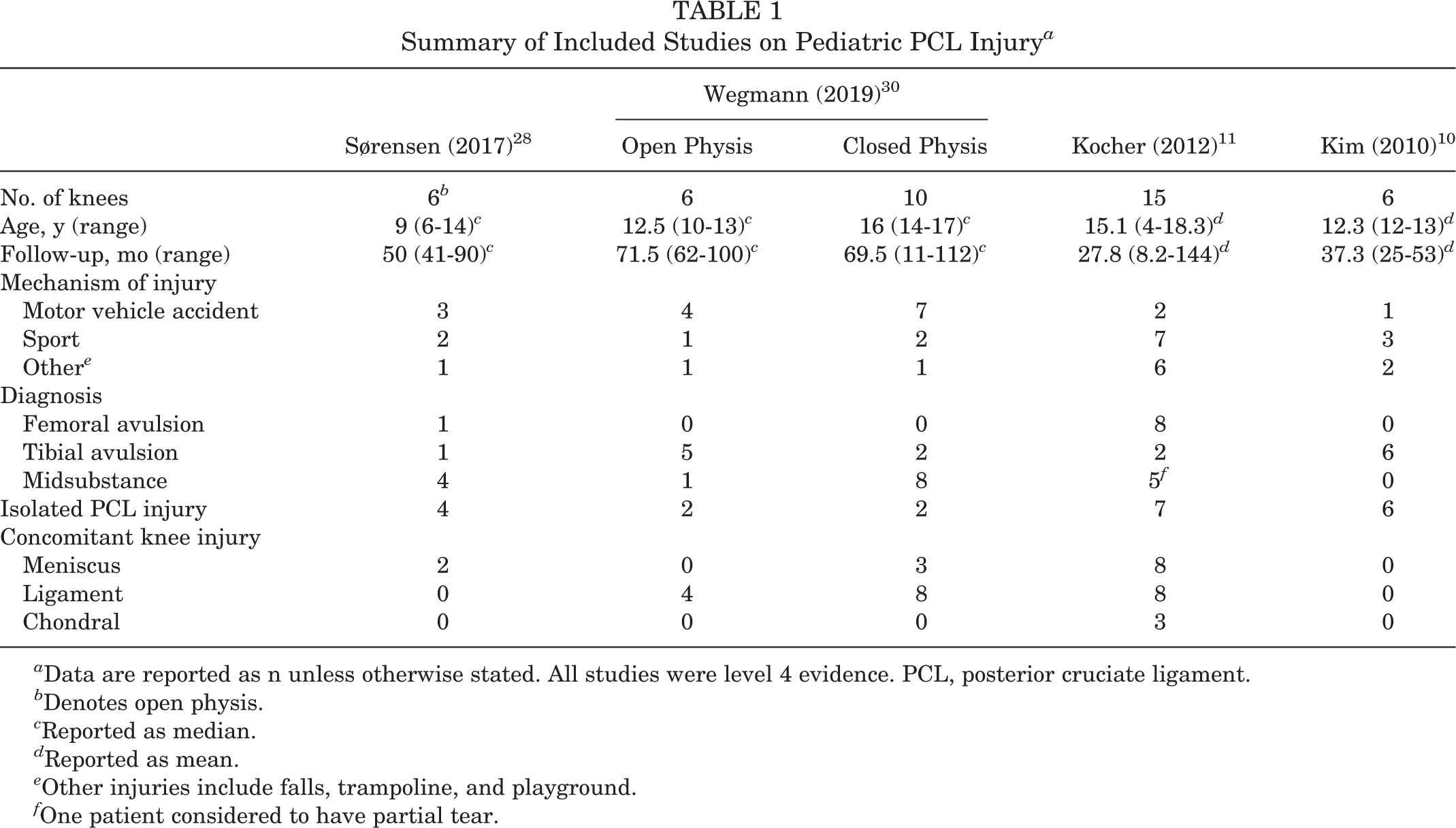
a Data are reported as n unless otherwise stated. All studies were level 4 evidence. PCL, posterior cruciate ligament.
b Denotes open physis.
c Reported as median.
d Reported as mean.
e Other injuries include falls, trampoline, and playground.
f One patient considered to have partial tear.
Repair Technique
Three of the reviewed papers described the repair technique. One study performed open reduction and screw fixation for displaced avulsion injuries. In cases with open physis, fluoroscopy was used to verify extraphyseal positioning. 30 All other repairs were performed arthroscopically. Sutures were passed through the PCL and through bone tunnels ultimately tied over a button or cortical bone bridge. 10,11 In the case of tibia peel-off injuries, the authors described the use of anterior medial, posteromedial, and posterolateral accessory portals. The posteromedial portal was the primary viewing portal, and the posterolateral and medial portals were used as working portals for suture passage/management. A transphyseal drill technique was used to place bone tunnels and pass sutures over a cortical bone bridge. 11
Reconstruction Technique
Arthroscopy-assisted reconstruction techniques similar to those used in adult patients were described in 4 studies. One study commented on physis-sparing techniques, especially with regard to tibial bone tunnel placement. 28 One study performed transphyseal drilling and commented on steep tunnel drilling with a minimal aiming angle of 60°, which would minimize injury to the physis by creating a small cross-sectional area of the tunnel at the level of the physis. 30 A variety of grafts were used, including hamstring tendon, quadriceps tendon, and bone–patellar tendon–bone autografts. 28,30 The described allograft options consisted of Achilles tendon with bone block and maternal hamstring tendon allograft. 11 Lastly, 1 study performed PCL repairs in setting of avulsion injuries. 10
Outcome Measures
All studies reported on laxity, with 2 using KT-1000 arthrometer measurements, 10,28 2 using posterior drawer clinical examination, 10,11 and 1 using kneeling radiographs to compare side-to-side differences. 30 The aggregated KT-1000 arthrometer measured a mean 2.65-mm side-to-side difference (range, 0.7-6 mm) at a mean follow-up of 43.65 months (range, 25-90 months). 10,28 Kocher et al 11 grouped patients into International Knee Documentation Committee (IKDC) knee grades. One knee was in group A (0-2 mm), 10 were in group B (3-5 mm), 2 were in grade C (6-10 mm), and the grades of 2 were not reported. All were noted to have a “firm endpoint.” All studies reported on postoperative patient-reported outcome measures, with the Lysholm and Pediatric IKDC (Pedi-IKDC) scores being the most commonly reported. Three studies reported Lysholm scores with an aggregated mean score of 85.15 at a mean follow-up of 51.5 months (range, 11-144 months). 10,11,30 Two studies reported Pedi-IKDC scores with an aggregated mean score of 80 at a mean follow-up of 56.3 months (range, 11-144 months). 11,30 Two studies reported on return to activity with 83.3% (n = 10/12) of patients returning to their prior level of activity 10,28 (Table 2).
Summary of Outcomes of Pediatric PCL Injuries a
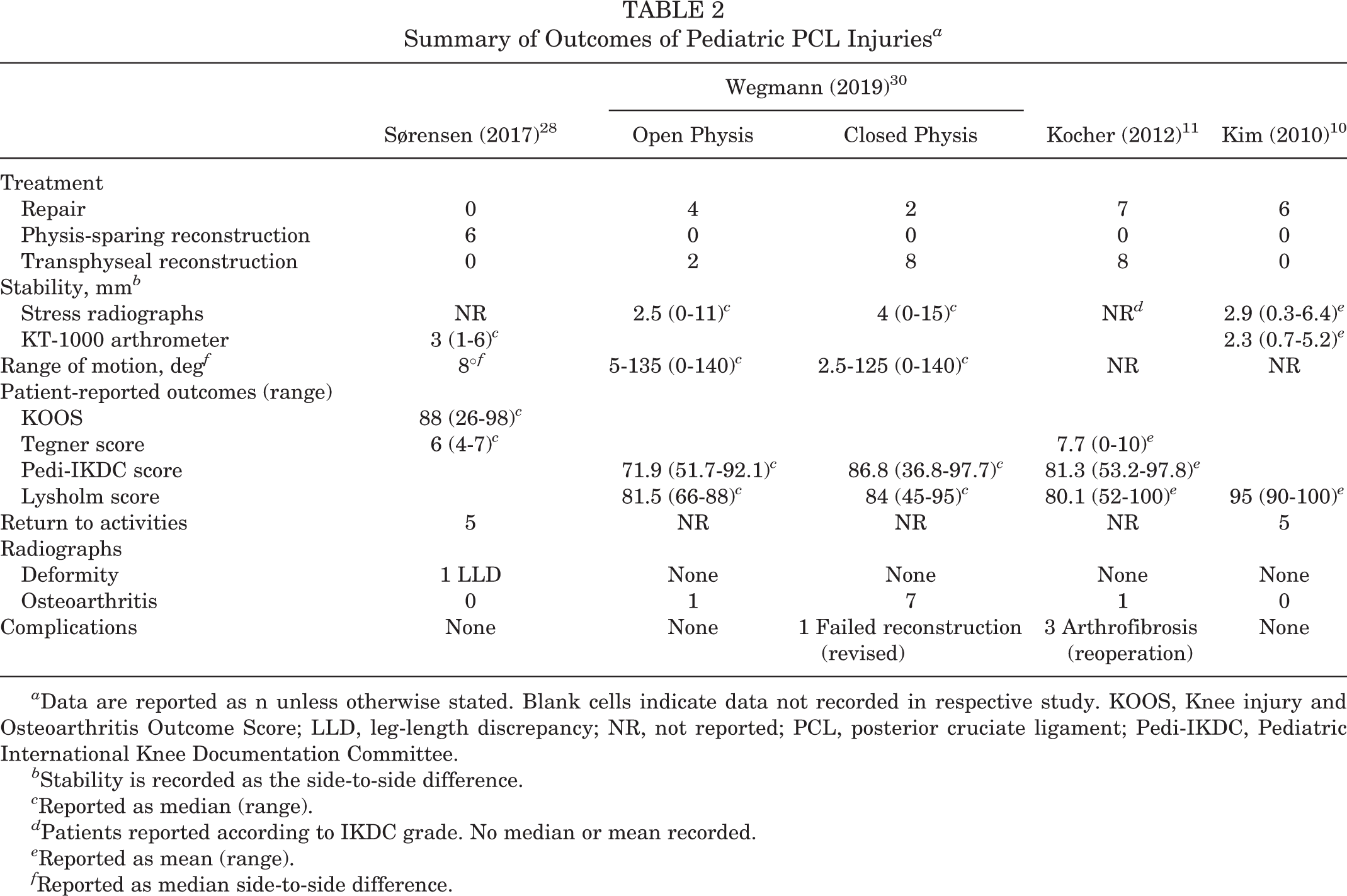
a Data are reported as n unless otherwise stated. Blank cells indicate data not recorded in respective study. KOOS, Knee injury and Osteoarthritis Outcome Score; LLD, leg-length discrepancy; NR, not reported; PCL, posterior cruciate ligament; Pedi-IKDC, Pediatric International Knee Documentation Committee.
b Stability is recorded as the side-to-side difference.
c Reported as median (range).
d Patients reported according to IKDC grade. No median or mean recorded.
e Reported as mean (range).
f Reported as median side-to-side difference.
Radiographic Outcomes
All studies commented on radiographic outcomes. Radiographs were used to measure leg-length discrepancies (LLDs) or angular deformity in 4 studies. There was only 1 documented clinically relevant LLD (>15 mm); however, this was present preoperatively and persisted postoperatively. 28 There were no other clinical or radiographic LLDs or angular deformity reported postoperatively. 10,11,28,30 Nine (21%) of 43 knees were noted to have osteoarthritis at final follow-up. 10,11,28,30
Complications
Two studies reported no complications. 10,28 Kocher et al 11 reported arthrofibrosis in 3 (7%) knees, 2 of whom underwent manipulation under anesthesia and 1 of whom underwent lysis of adhesions with manipulation. Wegmann et al 30 reported 1 knee experienced graft failure at a “later course” and subsequently underwent revision PCL reconstruction with bone–patellar tendon–bone autograft.
Quality Assessment
The mean MINORS score for noncomparative studies was 7 (range, 6-8). There was 1 comparative study with a MINORS score of 10 (Table 3). The most common items on the MINORS score that resulted in point deductions were prospective collection of data and prospective calculation of the study size. Further point deductions were noted for an endpoint appropriate to the aim of the study, a follow-up period appropriate to the aim of the study, and an unbiased assessment of the study endpoint.
Summary of MINORS Criteria a

a MINORS, Methodological Index for Non-Randomized Studies; criteria: 1 = clearly stated aim; 2 = inclusion of consecutive patients; 3 = prospective collection of data; 4 = endpoint appropriate to the aim of the study; 5 = unbiased assessment of the study endpoint; 6 = follow-up period appropriate to the aim of the study; 7 = loss to follow-up <5%; 8 = prospective calculation of study size; 9 = adequate control group; 10 = contemporary control group; 11 = baseline equivalent of groups; 12 = adequate statistical analysis. Dashes indicate not applicable.
b Comparative study.
Discussion
The principal findings of this study demonstrated overall good functional and clinical outcomes using operative management of PCL repair or reconstruction in pediatric patients. Documented repair and reconstruction techniques did not lead to LLDs or angular deformity of the lower extremity. However, concerns still exist with regard to tibial tunnel placement. Lastly, there is a risk of secondary osteoarthritis after PCL surgeries. This finding has also been demonstrated in the adult population. It is not clear whether or not operative management affects progression of osteoarthritis in the PCL-injured pediatric knee.
Treatment recommendations are lacking in pediatric patients, and guidance appears to be based on adult literature, as well as extrapolating recommendations for ACL avulsion injuries in the skeletally immature patient. 11 Currently, surgical management of PCL injuries in skeletally immature patients is based on the location of the injury, with repair favored in avulsion injuries and reconstruction in midsubstance tears. 1,9 –11,14,19,26,28 –30 Both transphyseal and physis-sparing techniques exist, with each posing theoretical risks to lower extremity growth or long-term graft integrity, respectively. 28,30 Repair techniques consist of reduction and fixation using either a screw or suture. 10,11,30
Injuries to the PCL requiring surgical interventions are rare in pediatric patients, and available studies are limited by small sample size or single case reports. Twenty-two (51%) of the 43 knees included in this review were evaluated with concomitant injuries. MVAs (39.5%) were the most common mechanism of injury, followed closely by sports-related injuries (35%). These findings are in line with previously documented findings in the adult literature. 3,4,22 Knee injuries in pediatric patients typically differ from those of their adult counterparts in that they result in fracture or physeal injuries because of the strength of the ligament compared with the bone or physis. 20 However, injury location was variable throughout the included reports (42% midsubstance, 37% tibial avulsions, and 21% femoral avulsions). 10,11,28,30 Sørensen et al 28 and Wegmann et al 30 specifically identified knees with open physes. Combined, there were 12 knees considered to have open physes; 5 (41.7%) sustained midsubstance tears, while the remaining 7 (58.3%) sustained avulsion injuries. Based on the included studies, there does not appear to be a clear association between age and injury location in those patients who require operative intervention; however, further work needs to be done.
Good postoperative patient-reported outcomes scores were demonstrated in all studies. No preoperative scores were reported; therefore, commenting on the effect of surgical management is beyond the scope of this review. The pooled Lysholm (85.15), Pedi-IKDC (80), and Tegner (6) scores were similar to previously documented scores in adult patients. 5 In their study of the management of PCL injuries in pediatric knees, Kocher et al 11 reviewed the outcomes of 11 patients managed using nonoperative treatment. Six (55%) of these knees sustained isolated PCL injuries, while the remaining 5 (45%) had concomitant injuries. The mean Pedi-IKDC (81.3), Tegner (7.7), and Lysholm (80.1) scores reported by nonoperatively treated knees were comparable to the pooled scores of the present study.
Currently, no treatment guidelines or algorithms exist for the treatment of PCL injuries in pediatric patients. 11 Adult PCL injuries have historically been managed nonoperatively, but emerging long-term follow-up studies have demonstrated an increased risk of osteoarthritis. 21,24,25 This progression is concerning in pediatric patients because of the limited number of treatment options for osteoarthritis in this patient population. Wegmann et al 30 reported on 16 surgically treated PCL injuries; 50% (n = 8/16) of the knees had varying grades of osteoarthritis on radiographic follow-up. Osteoarthritis was documented in 21% (n = 9/43) of the knees included in the present review. 10,11,28,30
One of the principal concerns in the surgical management of ligament injuries in pediatric knees is injury to the physis that can result in LLDs or angular deformity. Transphyseal and physis-sparing techniques for repairing or reconstructing PCL injuries in skeletally immature patients have been reported. ‡ Previous work on ACL reconstruction in skeletally immature patients has increased the understanding of the risks associated with the repair and reconstruction strategy. One rabbit model demonstrated that disruption of ≥7% of the cross-sectional area of the distal femoral physis caused substantial growth disturbance. 16 The physeal volume is known to increase with age, and via magnetic resonance imaging modeling, it has been shown that the percentage of physeal disruption from a given reamer size was less in the older children studied. 8 Kocher et al 12 reported on 59 skeletally immature patients with a mean chronological age of 14.7 years (range, 11.6-16.9 years), classified as Tanner stage 3, who underwent transphyseal ACL reconstruction using soft tissue autograft. No angular deformity was noted on radiographic measurement, and no LLD was measured clinically. This is consistent with previously published reports. 13 Bone plugs across the physis, large tunnels (>12 mm), and hardware crossing the physis are all factors that have been associated with angular deformity or LLDs in ACL reconstruction. 12 Wegmann et al 30 specifically evaluated growth disturbance after surgical treatment of PCL injuries in pediatric patients. Avulsions that were amenable to repair were treated using epiphyseal screw fixation; otherwise, reconstruction was performed using the transphyseal technique. The authors specifically commented on a steep drilling angle (minimum 60°) for the tibial tunnel in order to minimize injury to the physis. This steep angle would create a small cross-sectional area at the level of the physis. Six patients (6 knees) were considered skeletally immature; 4 of 6 were treated using epiphyseal screw fixation, while the remaining 2 patients were treated using reconstruction. In this group, no growth disturbances were measured on radiographic follow-up (median, 71.5 months). Furthermore, they evaluated a group of patients with “closing” or closed physes with a median age of 16 years. Eight of the 10 knees were treated using transphyseal reconstruction, and none demonstrated growth disturbances at a median follow-up of 69.5 months. However, radiographs did demonstrate signs of osteoarthritis in 7 knees. 30 The findings pertaining to angular deformity and LLDs have been supported by previous case reports and other reports included in this review. 1,10,11,23,28 The physis-sparing technique aims to avoid physeal injury by drilling tunnels away from the physis. However, reconstructing the PCL in skeletally immature patients requires placing the tibial tunnel distal to the physis. The tunnel will migrate distally with continued growth. Theoretically, this can lead to graft elongation and therefore concern for laxity or failure over time. This was not demonstrated in the included study using this as the primary technique 28 or in the previous documented case series. 23
There were several limitations to our study. First, this systematic review included entirely level 4 evidence with no prospective studies and small sample sizes. Second, the surgically treated patients were heterogenous in terms of concomitant injuries. These concomitant injuries can skew the reported outcomes, making it difficult to draw conclusions regarding the management of PCL injuries. We acknowledge that there are significant quality limitations based on MINORS criteria assessment. Many of these are related to study design and lack of prospective data, as well as heterogeneity in injury patterns. This is due in part to the rare nature of these injuries, specific patient population, and lack of multicenter studies.
Conclusion
PCL injuries in pediatric patients are infrequent and often occur with concomitant injuries. This is the first systematic review addressing the outcomes of operative management of pediatric PCL injuries. Successful repair and reconstruction can be obtained with acceptable risk to open physes. Good patient-reported outcomes and return to activity can be obtained using repair or reconstruction. Osteoarthritis was present in 21% of knees included in this study. While the results presented reflect the outcomes of lower-quality studies, this paper can still serve as a starting point for patient guidance and future research. The presentation of these radiographic changes early in life can have a negative effect on future activity, and patients should be made aware of this potential risk.
Footnotes
Notes
Final revision submitted February 14, 2021; accepted March 4, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.S. has received nonconsulting fees from Arthrex and consulting fees from Arthrex, DePuy/Medical Device Business Services, and DJO. L.D.F. has received consulting fees from Zimmer Biomet and hospitality payments from MTS. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.