
Abstract
Background:
The estimated cost per year of injuries in collegiate athletics has been reported to be billions of dollars in the United States. Injury prevention programs are often assessed only by their ability to reduce injuries, and there is little evidence of any potential reduction in associated health care costs.
Purpose:
To investigate changes in injury-related health care costs at a National Collegiate Athletic Association (NCAA) Division I university after the implementation of an injury prevention program.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 12 sports teams that used the injury prevention program (user group) and 16 teams that did not implement the program (nonuser group). The injury surveillance and prevention system (Sparta Science) utilized a commercially available force-plate system to assess kinematic variables, flag high-risk athletes, and guide individual conditioning programs. Data were obtained from 3 academic years before (2012-2014) and 2 academic years after (2015-2016) implementation of the Sparta Science system. The number of injuries and associated health care costs (surgery, clinic visits, imaging, and physical therapy) were compared between users and nonusers.
Results:
Total average annual injuries did not change significantly between users and nonusers after implementation of the program; however, users demonstrated a 23% reduction in clinic visits as compared with a 14% increase for nonusers (P = .049). Users demonstrated a 13% reduction in associated health care encounters, compared with a 13% increase for nonusers (P = .032). Overall health care costs changed significantly for both groups, with an observed 19% decrease ($2,456,154 to $1,978,799) for users and an 8% increase ($1,177,542 to $1,270,846) for nonusers (P < .01 for both). Costs related to associated health care encounters also decreased by 20% for users as compared with a 39% increase for nonusers (P = .027).
Conclusion:
This study demonstrated the ability to significantly reduce injury-related health care costs in NCAA Division I athletes via a comprehensive injury surveillance and prevention program utilizing force-plate technology. Given the substantial and appropriate focus on value of care delivery across the US health care system, we recommend the continued study of sports injury surveillance and prevention programs for reducing injury-related health care costs.
Collegiate sports injuries are prevalent and often associated with significant health care costs related to physician visits, imaging, hospitalizations, and surgical procedures. According to the National Collegiate Athletic Association (NCAA) injury surveillance program, high injury rates are found commonly across a wide spectrum of collegiate sports in the United States. Men’s college lacrosse players were found to sustain 5.3 injuries per 1000 athlete-exposures (AE) with an AE defined as participation in any official practice or competition. 12 Similar injury rates with differences between genders were observed among additional college sports. Male and female college athletes demonstrated respective injury rates of 8.0 versus 6.5 per 1000 AE in basketball, 4.7 versus 7.1 per 1000 AE in volleyball, and 8.1 versus 8.4 per 1000 AE in soccer. 1,27,37 In consideration of all NCAA collegiate sports, men’s football was found to have the highest competition injury rate, at 36.9 injuries per 1000 AE. 13
The high prevalence of youth sports injuries is a health care burden that causes a significant amount of annual health care expenditure. 5,18 According to a study of the Nationwide Inpatient Sample, over 10,000 youth in the United States are hospitalized annually because of sports injuries, and a majority of those hospitalized commonly undergo lower-extremity procedures. 35 Sports-related injuries in adolescents and high school students have been reported to account for over 400,000 annual emergency department (ED) visits in the United States, with an associated $605 million in hospital charges. 22,23 Youth and adolescent sports injuries in Florida alone accounted for over $87 million in ED care and $24 million in inpatient care annually. 30 Furthermore, the total cost of youth sports injuries is likely much higher, as these estimates do not include the costs associated with physical therapy (PT), bracing, or follow-up.
Studies across 25 NCAA men’s and women’s sports have demonstrated that many injuries are because of noncontact mechanisms and frequently localized to the lower extremity. For example, ankle sprains are observed frequently, with an incidence rate of 1.0 per 1000 AE, whereas hip and groin injuries, including adductor tears, have an incidence of 0.5 per 1000 AE. 11,20 Such lower-extremity injuries often result in a significant increase in medical attention and time lost from sport. 6,8,31 Kay et al 10 found that severe injuries resulting in at least 21 days of lost sports participation carried an incidence of 0.7 per 1000 AE, and were most commonly the result of lower-extremity sprains, strains, and fractures. As such, injury prevention programs focused on reducing lower-extremity injuries among athletes are especially important for reducing injury-related health care costs.
Various guidelines have reported that lower-extremity injuries may decrease with appropriate injury prevention training programs, which provide feedback about an athlete’s plyometrics, balance, and flexibility to improve functional performance and lower-extremity biomechanics. 7,21,24 Toward this effort, devices such as force plates, with the capability to measure and provide feedback about an athlete’s balance, dynamic postural stability, and jumping and landing forces, have been developed. 26,33,34 Injury prevention programs utilizing force plates have been shown to improve knee strength, flexion, and stability among female high school basketball players and improved loading rates and dynamic postural stability among college female volleyball players. 16,29 Force-plate injury prevention programs have also been shown to improve lower-extremity neuromuscular control, significantly reducing lower-extremity injuries among adolescent soccer and handball players. 36
Although the use of force-plate technology in injury prevention programs has been reported previously in the literature, studies have typically been limited to a single sport and sex and often focused on only a single type of injury or anatomic region (eg, lower-extremity injuries). 16,29,36 Moreover, there is a paucity of literature evaluating the impact of sports injury surveillance and prevention programs on associated health care costs. Therefore, the purpose of this study was to evaluate the implementation of an injury surveillance and prevention program across 28 men’s and women’s varsity sports at an NCAA Division I athletic program. We hypothesized a decrease in sports injuries, physician visits, and associated health care costs in those athletes utilizing the program.
Methods
Included were 28 varsity sports teams from a single NCAA Division I university. Each team was designated as a “user” or “nonuser” based on their utilization of the Sparta Science injury surveillance and prevention system; there were 12 teams in the user group and 16 teams in the nonuser group. Medical billing and injury data were obtained from 3 academic years before (2012-2014) and 2 academic years after (2015-2016) the implementation of the Sparta Science system. Injuries and associated health care costs (in 2012-2016 US dollars) were recorded for each sport within the user and nonuser groups before and after implementation of the injury prevention program, and the groups were compared with respect to clinic, surgical, PT, and imaging charges.
Force-Plate Protocol
The Sparta Science system utilizes a commercially available force-plate system with dedicated software to assess kinematic variables gathered from vertical jump via recognizing alterations in the resultant force-time curve. The data are used to identify athletes with a potentially higher injury risk and to guide athlete-specific strength and conditioning programs. Given the number of varsity sports and athletes under evaluation at our institution, 3 force plates were utilized. The force plates are positioned strategically directly within our strength and conditioning center for ease of access and implementation. All athletes underwent a preseason evaluation with variability in additional evaluations per sport. Additional evaluation also depended on the injury status of the particular athlete, with injured athletes receiving additional nonstandardized evaluation during their recovery. We are currently developing a more systematic approach; the further development of a comprehensive systematic protocol will likely be informed by sex-, sport-, and position-specific data.
During each evaluation, the athlete underwent practical assessment via vertical jump analysis of load, explode, and drive metrics. The first force measured was load, defined as the average eccentric rate of force; it occurs during the beginning of the jump and represents an athlete’s ability to generate force. Explode, the second force measured, was defined as the relative concentric force, occurring during the point of transition or the amortization phase and representing the athlete’s ability to explode during movements and transfer force well. Drive, defined as concentric relative impulse, was the third force measured; it represents an athlete’s ability to drive and finish movements smoothly. All 3 metrics contribute to defining a player’s particular profile or signature, the reliability and validity of which we continue to study. These metrics are utilized by our strength and conditioning experts in the implementation of targeted programs based on signature movement, injury prevention, and sports-specific skill development.
Statistical Analysis
Statistical analyses were performed via the chi-square test to compare changes in overall injury rates within the user and nonuser groups. Repeated-measures analysis of variance was used to compare change in overall health care costs within the study groups. The Fisher exact test was further utilized to compare the change in overall injury numbers, surgeries, clinic visits, imaging requests, and PT visits between the groups. The paired t test was used to compare the percentage change in associated health care encounters between the user and nonuser groups.
Results
Change in Injury Rates
Average total injuries decreased slightly by 1.12% from 179 per year to 177 for the user group, but this decrease did not prove significant (P = .77). For the nonuser group, average total injuries slightly increased by 11.01% from 109 to 121, but this increase was also not significant (P = .13) (Table 1). There was also no significant difference when comparing the change in injury rate between the 2 groups (P = .50) (Figure 1A). As such, the injury prevention program did not affect the overall rate of injury.
Annual Injuries and Associated Health Care Charges Before and After Program Implementation a

a Bolded P values indicate statistically significant difference from before to after implementation. M, men’s; W, women’s.
b In 2012-2016 US dollars.

Comparison of annual (A) number of injuries and (B) charges between users and nonusers. Post, postimplementation; Pre, preimplementation.
When examining associated health care encounters after implementation of the program, an overall decrease was observed in all categories except for PT visits within the user group. Specifically, there was a 29% decrease in surgeries, a 23% decrease in clinic visits, a 7% decrease in imaging requests, a 6% increase in PT visits, and a 13% decrease in combined health care encounters (Figure 2). In contrast, the nonuser group demonstrated a 3% reduction in surgeries, a 14% increase in clinic visits, no change in imaging requests, a 33% increase in PT courses, and a 13% increase in combined health care encounters. Although the change in surgical visits (P = .46), requested imaging (P = .81), and PT courses (P = .37) were not significantly different between the 2 groups, the change in clinic visits (P = .049) and combined health care encounters (P = .032) demonstrated statistical significance (Table 2).

Percentage change in health care claims and associated charges after program implementation.
Health Care Claims Before and After Program Implementation a

a Bold P values indicate statistically significant difference between groups.
Change in Health Care Costs
Average total health care costs related to injury changed significantly from before to after implementation for the user group (P < .01) (Table 1) and overall health care costs decreased by 19.44% from $2,456,154 to $1,978,799 (Figure 1B). For the nonuser group, the average total costs changed significantly pre- and postimplementation, with an increase of 7.92% from $1,177,542 to $1,270,846 (P < .01). When comparing the cost of associated health care encounters within the user group, there was a 45% reduction in surgery charges, 48% reduction in clinic charges, 1% decrease in imaging charges, 13% increase in PT-related charges, and a 19.6% reduction in combined health care encounter charges (Figure 2). Conversely, the nonuser group demonstrated a 33% increase in surgery charges, no change in clinic charges, an 83% increase in imaging charges, a 35% increase in PT-related charges, and a 39% increase in combined health care encounter charges. In direct comparison of the percentage change of associated health care charges, there was a statistically significant difference between the 2 groups (P = .027) (Table 3).
Percentage Change in Health Care Charges Before and After Program Implementation a
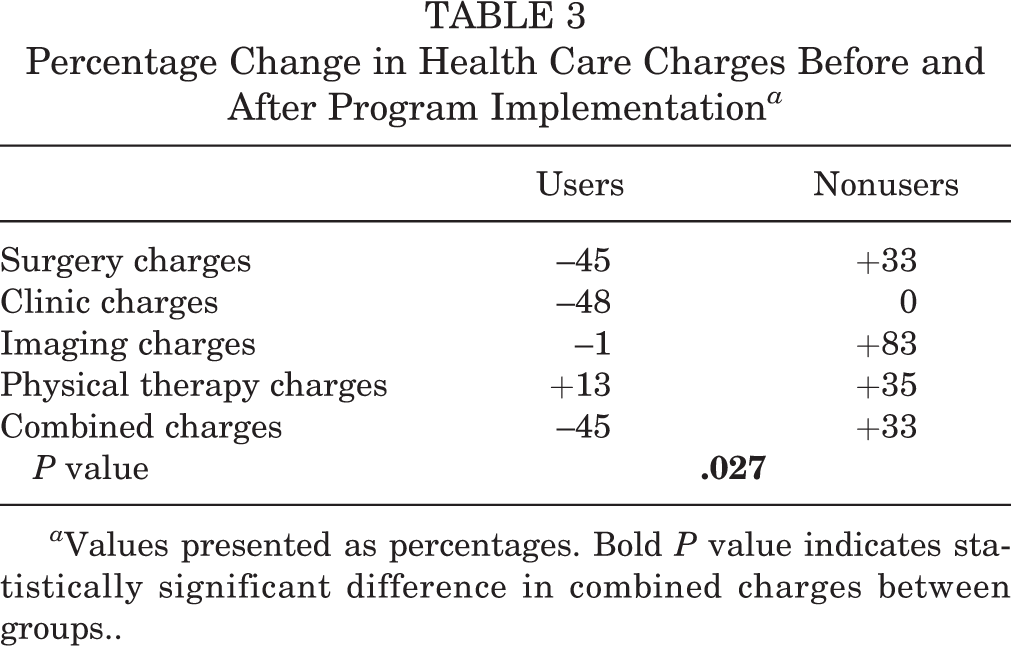
a Values presented as percentages. Bold P value indicates statistically significant difference in combined charges between groups..
Discussion
Sports injuries among collegiate athletes are common, often resulting in significant incurred medical costs for health care systems. In this study, we demonstrated a reduction in associated health care encounters and costs with systematic implementation of an injury surveillance and prevention program at an NCAA Division I university. Although there was no significant difference in the number of annual injuries after implementation of the program, users demonstrated a 13% reduction in combined annual associated health care encounters as compared with a 13% increase for nonusers. Specifically, users demonstrated a 29% reduction in required surgeries as compared with a slight 3% reduction for nonusers. Users also demonstrated a 23% reduction in clinic visits as compared with a 14% increase by nonusers—a difference of 37% between the 2 groups. Similarly, the quantity of imaging ordered decreased by 7% for users while nonusers demonstrated no change. Although the number of PT courses increased for both groups of athletes, nonusers experienced a 27% greater increase in the number of PT visits as compared with users. This suggests decrease in the severity of injury among athletes utilizing the force-plate technology system after implementation of the injury prevention program.
In our utilization of force-plate technology for injury surveillance and prevention, we also demonstrated a significant reduction in associated health care costs. After program implementation, the user group experienced a 45% reduction in total surgical charges as compared with the nonuser group, who experienced a 33% increase in surgical charges. Moreover, charges resulting from clinic visits decreased by 48% as compared with the nonuser group. Differences among imaging costs were also notable, as demonstrated by a 1% reduction of image-related charges among the user group and an 83% increase in the nonuser group. Although both athlete groups demonstrated an increase in PT-related charges, nonusers experienced a 22% greater increase in PT charges as compared with users (35% versus 13%).
Various prevention strategies have been implemented in the United States in an effort to prevent sports injuries and reduce health care costs. For example, the Fédération Internationale de Football Association 11+ and 11+ kids injury prevention program has demonstrated reduced noncontact injuries among pediatric and college soccer players, with an associated 50% reduction in health care costs. 2,28,32 Rule changes, such as the removal of body-checking from youth ice hockey, have also been shown to significantly decrease the incidence of injuries and to lower health care costs. 15 Other interventions, such as the Knee Injury Prevention Program and the Prevent Injury and Enhance Performance strategy, have also been shown to reduce the risk of noncontact lower-extremity injury and anterior cruciate ligament tears among young athletes. 9 In addition, several injury prevention programs focused on improving balance, flexibility, strength, and neuromuscular control through warm-up exercises have been developed. One such intervention, focused on improving lower-extremity strength and stability, was found to be effective in reducing health care costs among male soccer players. However, the program failed to demonstrate a decreased rate of injury. 14 Another intervention, focused on improving neuromuscular training among youth soccer players, significantly reduced injury rates and health care costs, including general orthopaedic, sports medicine, and ED visits. 19 Although these programs have demonstrated a reduction in injuries and health care costs for a few select sports, a broader and more comprehensive injury prevention and surveillance program is needed to effectively decrease costs across a greater variety of sports.
When considering ED and physician visits, surgeries, and hospital admissions, pediatric sports injuries directly result in over $10 billion in annual health care costs. 4 The regional costs of sports injuries can also significantly affect the health care system. According to an orthopaedic practice covering regional high school sports programs, 2.4% of all athletes are referred to orthopaedic surgeons for further treatment, with an average cost of $44,240 for each visit, including any subsequent surgical treatment. 17
Given these new injury prevention strategies and appropriate cost considerations, recent programs have incorporated modern force-plate technology to evaluate an athlete’s balance, dynamic stability, and force generation more accurately with the aggregation of objective data. Such injury prevention programs have demonstrated efficacy in improving knee strength and stability among high school basketball players, dynamic postural stability among college female volleyball players, and neuromuscular control among adolescent soccer players. 16,29,36 Buckley et al 3 also demonstrated that force-plate technology could be used to determine differences in gait initiation among NCAA Division I athletes. In addition, force plates have been utilized to evaluate baseball hitting mechanics among male collegiate baseball players. 25
This study has several limitations. The long-term effects of this particular injury prevention program were not assessed and therefore remain unknown. In addition, the sport-specific effect of this injury prevention program was not evaluated. Indirect costs, such as those incurred owing to time lost from participation, were not included in this study. There was limited standardization of injury reporting across all sports, so injuries were classified via anatomic region without specifics as to type of injury. Therefore, the specific injury data are unable to be analyzed in a homogeneous way aside from generalized categories. Furthermore, the implementation of a force-plate system requires startup capital that varies based on the particular systems utilized and the length of the negotiated contract, as certain systems may be purchased or leased from the manufacturer for a determined period of time. The cost of the force-plate system utilized in this study was covered via a philanthropic gift to our athletic department so it did not affect our overall cost analysis.
The inclusion of football in the overall user charge analysis may appear to provide a larger contribution of effect, which we have attempted to account for in our reporting of percentage change data, where football is weighted as the second largest percentage change in the user group. We feel the inclusion of football in the overall analysis remains critical, given the influence of this sport on any injury prevention and cost reduction evaluation. In addition, this retrospective evaluation may include a degree of selection bias in that the participation of specific teams was determined before the knowledge and implementation of our study design and analysis. Finally, the 5-year study period may be restricted in power, with the inclusion of additional years and data points providing a more robust evaluation. Therefore, future studies should attempt to evaluate the longer-term outcomes of college-wide injury prevention programs with respect to changes in the types of injuries and associated health care costs. Additional study may also evaluate the effectiveness of force-plate injury surveillance and prevention programs among other cohorts of athletes, such as professional or high school athletes.
Conclusion
This is the first study to demonstrate the ability to significantly reduce injury-related health care costs in NCAA Division I athletics via a comprehensive injury surveillance and prevention program utilizing force-plate technology. Given the substantial and appropriate focus on value of care delivery across the US health care system, we recommend the implementation and continued study of sports injury surveillance and prevention programs as a means of reducing injury-related health care costs.
Footnotes
Final revision submitted January 8, 2021; accepted February 23, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.L.P. has received grant supports and education payments from Arthrex. D.P.T. has received grant support from Arthrex and education payments from Arthrex, Peerless Surgical, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Pennsylvania institutional review board (protocol No. 826557).