
Abstract
Background:
Avulsion fracture of the lesser tuberosity (AFLT) of the humerus has traditionally been treated with open reduction internal fixation using screw fixation. The clinical outcomes of arthroscopic repair with suture anchors remains unknown.
Hypothesis:
It was hypothesized that arthroscopic fixation with suture anchors would result in good clinical outcomes for the treatment of AFLT.
Study Design:
Case series; Level of evidence, 4.
Methods:
This study included 15 patients who underwent arthroscopic repair of AFLT of the humerus between January 2014 and October 2017. All patients had 3-dimensional computed tomography scans and magnetic resonance imaging to evaluate the avulsed fracture and concomitant injuries before surgery. The arthroscopic double-row and suture-bridge techniques were used based on the morphology of the avulsion fractures. Functional outcomes were assessed with range of motion, the visual analog scale (VAS) for pain, the Subjective Shoulder Value (SSV), the American Shoulder and Elbow Surgeons (ASES) score, and the University of California, Los Angeles (UCLA) shoulder score. The bear-hug test, liftoff test, and internal rotation resistance test at 90° abduction and external rotation (IRRT 90°) were used to evaluate subscapularis tendon integrity.
Results:
The mean follow-up time was 3.5 years (range, 3-5 years). Comminuted fractures with 1 large part and ≥1 small pieces were seen in 12 cases, partial tear of the supraspinatus in 2 cases, Bankart lesion in 2 cases, and superior labrum anterior to posterior injury in 2 cases. There was a statistically significant improvement from the baseline to the final follow-up in the VAS (from 6.9 ± 1.5 to 1.1 ± 1), SSV (from 30.7 ± 5.1 to 90.5 ± 11.6), ASES (from 28.5 ± 7.7 to 92.3 ± 4.5), and UCLA (from 29.5 ± 6.3 to 94.2 ± 8.3) scores (P < .001 for all). All patients showed full range of shoulder motion and bilateral symmetric strength on physical examination with the bear-hug test, liftoff test, and IRRT 90° test.
Conclusion:
The arthroscopic repair of AFLT resulted in excellent reduction and healing of the displaced fragment. At the final follow-up, clinical and functional results were good. Associated injuries occurred in 40% of patients but did not affect outcomes.
Avulsion fractures of lesser tuberosity (AFLT) usually occur in association with Neer 3- or 4-part fractures and fracture dislocations of the proximal end of the humerus. 15 Isolated AFLT is very rare and involves mostly younger patients. 15,17,20 It has been estimated that the incidence of isolated AFLT in adults is 0.46 per 100,000 population per year, with a median age of 43 years. 18
Nondisplaced AFLT can be managed conservatively with satisfactory results. 16,23 Displacement of the lesser tuberosity >5 mm or angulation >45 are acceptable surgical criteria. 14 However, most studies seem to indicate that any displacement of the lesser tuberosity is an indication for surgery. 3,16,18,23 Traditionally, open reduction internal fixation using screw fixation was the surgical treatment of choice for AFLT. 10,14,16,18,23 To our knowledge, only 3 studies (technique note and case report) about arthroscopic reduction and fixation for AFLT have been reported. 4,8,19 There is a paucity of information in the literature regarding the outcomes of arthroscopic fixation of AFLT.
The purpose of this study was to evaluate the characteristics of avulsion fragments and functional outcomes at the latest follow-up in a consecutive series of patients who received arthroscopic fixation. The hypothesis was that arthroscopic fixation with suture anchors could result in good clinical outcomes for the treatment of AFLT.
Methods
Study Population
This institutional review board–approved retrospective study included 15 patients who underwent arthroscopic repair of AFLT. All operations were performed by 3 experienced shoulder surgeons (L.L., G.C., and H.Y.) in our hospital between January 2014 and October 2017. Patients were identified by reviewing surgical records, and all identified patients were contacted and invited for a follow-up examination. There were no exclusion criteria.
Surgical Technique
Under general anesthesia, the patient was placed in the beach-chair position for the arthroscopic procedure. The techniques performed in this study were similar to those of previous reports.
2,8,19
Portals for the arthroscopic repair of AFLT have been described previously: the standard posterior portal, anterolateral portal, anterior portal, and anteroinferior portal.
2,8
The double-row and suture-bridge techniques were used based on different morphology of avulsion fractures. The 5 most important considerations for the procedure were as follows: An arthroscopic suprapectoral tenodesis was performed for patients with a subluxated or dislocated long head of the biceps tendon (LHBT) to provide better visualization of the subscapularis footprint. For the cases without subluxated or dislocated LHBT, the LHBT was preserved. If the LHBT was intact, it was noted that anchor sutures should avoid accidental tenodesis of the LHBT, which may be incorporated during the medial to lateral suture passage. For chronic cases, complete mobilization of the retracted subscapularis tendon was necessary to pull the avulsion fractures back to the lesser tuberosity. The bony defect on the humerus was debrided to make a bleeding bone bed to optimize the area’s healing potential. Adequate debridement of the scar tissue surrounding the avulsed fragment was also performed. For the medial row, suture anchor sites were drilled in a standard fashion, and the suture anchors were inserted through the anterior portal and malleted into place at the medial border of the bone bed on the humerus (Figure 1A and 1B). One or 2 suture anchors (3.5-mm TwinFix or 4.5-mm TwinFixPEEK; Smith & Nephew) double-loaded with No. 2 braided, nonabsorbable sutures (Smith & Nephew) were used, depending on the size of the bony defect, using horizontal mattress sutures through the inferior and superior aspects of the bone-tendon junction, which could be cinched down to the humerus at the lesser tuberosity (Figure 1C). For lateral anchor sites, 2 areas just lateral to the bone bed were used to create a superior and inferior footprints for suture anchor fixation. If the LHBT was intact, lateral anchors could be placed between the groove of the LHBT and the lateral margin of the bone bed. Because the comminuted soft cancellous bone within the lesser tuberosity might not be strong enough to hold the anchors, subsequent lateral-row fixation was achieved on the bicipital groove, which was an excellent point for anchor placement. Either the 4.5-mm Footprint PK (Smith & Nephew) or the Pushlock (Arthrex) was used as the lateral-row anchors, depending on the number of sutures and the surgeon’s preference. By internal rotation of the arm, the lateral-row anchors could be easily secured with appropriate tension. The finished repair demonstrated the avulsed fragment positioned securely in an anatomic position (Figure 1D). Lesser tuberosity fixation was the first step before the repair of simultaneous rotator cuff injuries, as iatrogenic swelling and fluid extravasation could compromise the subcoracoid space. Anchor placement and suture passage through the capsule for Bankart lesions were performed first and knotted after fixation of the AFLT.

Arthroscopic fixation of avulsion fracture of the lesser tuberosity of the left shoulder viewed from the lateral portal. (A) The lesser tuberosity avulsion fracture as well as the avulsion bed were shown. (B) Suture anchors were placed as medial row anchors. (C) Sutures were placed through the subscapularis tendon-bone junction. (D) Lateral row anchors were placed with tension.
Postoperative Rehabilitation
A sling was used to protect the patient’s arm for 6 weeks. On the third day after surgery, pendulum and self-assisted circumduction exercises were initiated. There were strict limitations to passive external rotation at <45° and abduction at <90°, and there was no active internal rotation for at least 6 weeks, after which these motions were progressively increased. By 10 weeks, patients had progressed to full active and passive range of motion (ROM), gradual strengthening, and stretching exercises.
Clinical Assessment
Preoperative parameters, including ROM, visual analog scale (VAS) for pain, Subjective Shoulder Value (SSV), American Shoulder and Elbow Surgeons (ASES) score, and University of California, Los Angeles (UCLA) shoulder score, were extracted from preoperative notes. Concomitant shoulder lesions and intraoperative treatment of these lesions were also noted. Before surgery, all patients had undergone a clinical examination, standard radiographs of the shoulder, 3-dimensional computed tomography (3D CT) scan, and magnetic resonance imaging (MRI); 3D CT scans were performed immediately and 3 months postoperatively. All patients underwent standardized follow-ups at 2 weeks, 3 months, 6 months,12 months, and 24 months postoperatively.
The latest follow-up assessment included a structured interview and a detailed physical examination by an independent shoulder surgeon (J.X.). Every patient provided the VAS, SSV, ASES, and UCLA scores. The physical examination included the bear-hug test, Jobe test, the liftoff test, internal rotation resistance test at 90° abduction and external rotation (IRRT 90° test), and ROM assessment.
Statistical Analysis
Continuous data are presented as means, ranges, and standard deviations. When the distribution of data was normal, paired t tests were used to compare pre- and postoperative variables. All statistical analyses were performed with SPSS software (Version 21.0; IBM), and P < .05 was considered significant.
Results
Patient Characteristics and Arthroscopic Findings
The characteristics of patients and arthroscopic findings are shown in Table 1. There were 2 patients with a dislocation, 2 with a rotator cuff tear, and 2 with superior labrum anterior to posterior (SLAP) lesions. For every patient, 2 anchors were used in the medial row as well as in the lateral row. The mean length of the surgery was 104 minutes (range, 75-129 minutes). The mean time to the latest follow-up was 3.5 years (range, 3-5 years).
Demographic Details, Arthroscopic Findings, and Concomitant Procedures a

a Data are reported as No. unless otherwise indicated. BMI, body mass index. LHBT, long head of biceps tendon; SLAP, superior labrum anterior to posterior.
Eight fractures were caused by contact sports injuries. Three fractures were sustained in a fall during biking, 1 while riding a motorcycle, and 3 patients were injured in a fall downstairs. No patient had an associated axillary nerve or brachial plexus injury. There were 6 patients who presented with chronic injuries (mean, 10 months; range, 3-35 months), and the other 9 patients underwent surgery between 7 days and 3 months from injury with a mean of 1 month.
Preoperative Radiographic Findings
All avulsed fragments were displaced medially and inferiorly confirmed by 3D CT scans. Eleven cases showed avulsed fragments rotated more than 90° on the axial scan. Twelve cases showed comminuted fractures with 1 large part and 1 or more small pieces. All of the patients demonstrated displacement of the major fragment over 10 mm. The sizes of the main fragments were as follows: length, 15-23 mm; width, 12-18 mm; and thickness 5-10 mm. Preoperative MRI showed that partial tear of the supraspinatus was found in 2 cases. The Bankart lesion was found in 2 cases and SLAP injury in 2 cases. Representative images of the avulsion fractures are shown in Figure 2.

Preoperative imaging. (A) The radiograph showing that the cortex of the lesser tuberosity was discontinuous. (B) The bony avulsion of the lesser tuberosity as seen on the 3D CT. (C) MRI in the axial plane showing the avulsed fracture. (D) MRI in the sagittal plane showing partial tear of supraspinatus. MRI, magnetic resonance imaging; 3D CT, 3-dimensional computed tomography.
Functional Outcomes
At the final follow-up, all patients completed the evaluation of shoulder scores and went back to their preinjury occupation, with no limitations in recreational activities, at 5 to 10 months postoperatively. There was a statistically significant improvement in VAS, SSV, ASES, and UCLA scores from the baseline to the final follow-up (Table 2). There was no significant difference between the injured and uninjured side. All patients showed full range of shoulder motion and bilateral symmetric strength on physical examination, with negative bear-hug, liftoff, and IRRT 90° tests. No major complications, such as permanent iatrogenic neurovascular, hematoma, and infection, were found in this series.
Clinical Outcomes Preoperatively and at Final Follow-up a

a All outcome measures were significantly different from preoperatively to the final follow-up (P < .05). ASES, American Shoulder and Elbow Surgeons; Preop, preoperative; ROM, range of motion; SSV, Subjective Shoulder Value; UCLA, University of California, Los Angeles; VAS, visual analog scale.
Postoperative 3D CT
All of the study patients showed bony union at the 3-month follow-up, and thus, no further CT scan was needed. Representative images are shown in Figure 3.
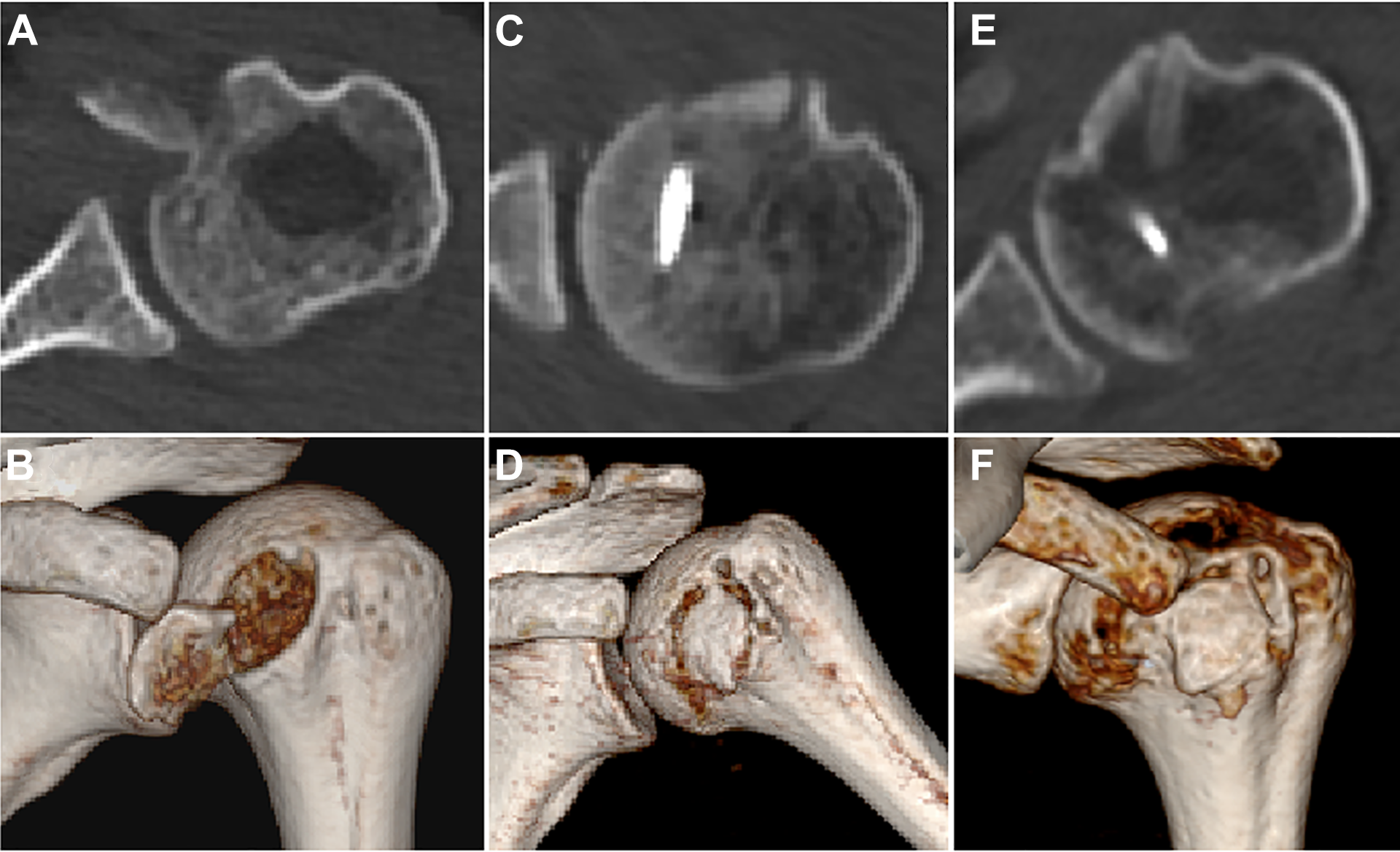
Avulsion fracture of lesser tuberosity was assessed by 3D CT pre- and postoperatively. (A and B) Preoperative 3D CT showed the displaced and angulated avulsion fracture. (C and D) Immediately postoperative 3D CT showed that anatomic reduction was achieved. (E and F) Three-month postoperative 3D CT showed that fracture union was achieved. 3D CT, 3-dimensional computed tomography.
Discussion
Our results showed that arthroscopic repair of AFLT resulted in excellent reduction and healing and provided good to excellent functional outcomes.
Small bony avulsion fragments of lesser tuberosity may not be easily apparent on radiographs, which may cause prolonged delays in definitive treatment. 7,18 To our knowledge, no other radiographic views should be obtained to avoid these fractures. CT and MRI are sensitive enough to avoid missing this fracture. In the present study, there were 6 patients presenting with chronic injuries (a duration of more than 3 months). All of these 6 patients demonstrated pain and/or weakness with attempted internal rotation of the shoulder, confirmed by the positive bear-hug, liftoff, and IRRT 90° tests. These physical examination findings are consistent with previous reports in the literature of similar injuries. 13,14,16,19 For each of our cases, MRI was used to confirm the presumptive diagnosis of subscapularis tear, which was made based on the medical history and physical examination. When an avulsion fragment was detected on MRI, bony fractures were further investigated by 3D CT, which could provide more detailed information about the features of the avulsed fragments. To our knowledge, most previous studies did not evaluate AFLT with CT scan images. The morphology of avulsed fragments in our study showed that most of the fragments were comminuted with 1 large part and 1 or more small/tiny pieces. This feature of the bony fracture should be managed with caution during operation.
Large and displaced fragments might be visible on plain radiographs, which usually were found in acute cases. For acute cases, both MRI and 3D CT scan were used to evaluate the affected shoulder. MRI remained one of the study choices because of its ability to concurrently assess the rotator cuff and other soft tissues, such as the labrum and the LHBT. There were 2 patients presented with partial supraspinatus tear, 2 with Bankart lesions, and 2 with SLAP lesions. The use of both MRI and 3D CT scan can provide the surgeons with more precise evaluation and more optimal treatment options before surgery.
Traditionally, open reduction internal fixation using screw fixation was the surgical treatment of choice for AFLT, and outcomes after surgical treatment are generally very good. 14,16,18,23 Excision of the lesser tuberosity also exists as a treatment option. 1,11,21 The arthroscopic repair of subscapularis tendon tears or isolated subscapularis avulsion injuries has been reported and is well-established. 5,12,22 A systematic review focusing on repairs of lesser tuberosity avulsion injuries in adolescents demonstrated good outcomes after both open and arthroscopic repairs, with no statistical difference between the 2 techniques in terms of clinical results. 24 Because the number of patients and studies was limited in this review, and different outcome measures were used in the literature, more studies are needed. Arthroscopic repair is potentially minimally invasive and can provide better cosmesis. More importantly, concomitant injuries could be found and repaired arthroscopically, such as rotator cuff tear and labral injury. About half of the additional injuries were found during operation in the study. Another benefit of arthroscopic techniques over open reduction internal fixation is that in the technique used in our study, there is no need to penetrate the avulsion fragment, which could possibly cause fragmentation and loss of fixation. One of the disadvantages of arthroscopic techniques is that the cost of suture anchors is much higher compared with screw fixation. Another disadvantage might be that it is technically more difficult.
The arthroscopic techniques reported in the literature were basically similar, although different fixation and suture methods existed, such as the single-row/double- row and knotless/knotted techniques. 4,8,19 In this study, 3 surgeons performed arthroscopic repair using the suture bridge or the double-row method to fix the avulsed fractures, depending on the specific features of the fracture and surgeon’s preference. Because this type of avulsion fracture was rare and cases were limited, we could not compare whether different arthroscopic techniques would lead to different results. Bony excision could be performed if the extremely small fragments could not be reduced arthroscopically and the main part of the avulsed fragment could be reduced anatomically. Care should be taken not to advance the subscapularis tendon, which could potentially alter its biomechanics.
The typical mechanism of injury is an abduction external rotation trauma to the shoulder. 6,9 With the arm in this position, the subscapularis muscle forcefully contracts to resist, leading to an avulsion of the lesser tuberosity. 19 Most of our patients were unable to describe the exact details of the deforming force because of the rapid sequence of energy transfer during the injury; thus, it was difficult to elicit a definite history of the exact mechanism of injury on direct questioning. Our findings were similar with those of a previous study, as these fractures were mostly caused by higher energy falls, such as a fall down stairs or during sports, such as cycling and horse riding. 18
There are several limitations in this study. (1) There was a lack of MRI evaluations at the latest follow-up. Although all patients resumed normal life and demonstrated negative bear-hug, liftoff, and IRRT 90° tests, additional MRIs could have helped us evaluate the subscapularis tendon and other soft tissue conditions. (2) Different arthroscopic techniques (double-row and suture bridge) were used in this study, and considering different morphology of avulsion fractures, it is reasonable to fix the avulsed fragments with different techniques. (3) No objective measure of internal rotation strength was performed. (4) The long-term functional outcome after arthroscopic repair remains unknown and needs further follow-up study.
Conclusion
The arthroscopic repair of AFLT resulted in excellent reduction and healing of the displaced fragment. At the final follow-up, the clinical and functional results were good. Associated injuries occurred in 40% of patients but did not affect the outcome.
Footnotes
Final revision submitted February 28, 2021; accepted March 19, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Peking University Third Hospital (ID: 2013125).