
Abstract
Background:
Medial patellofemoral ligament (MPFL) reconstruction, MPFL repair, and nonoperative treatment are important treatments for patients with patellar dislocation. However, it is unclear which treatment leads to better outcomes.
Purpose:
To determine the efficacy and safety of the 3 treatments in the treatment of patellar dislocation and compare the effect of MPFL reconstruction with MPFL repair, MPFL reconstruction with nonoperative treatment, and MPFL repair with nonoperative treatment.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
The PubMed, Web of Science, Cochrane Library, Embase, CNKI (China National Knowledge Infrastructure), and Wanfang databases were searched from inception to December 2020. Included were clinical studies that described the efficacy and safety of 2 of the 3 treatments, studies directly comparing the clinical effects of the 2 operative techniques, or studies comparing the effects of reconstruction or repair with nonoperative treatment. Two reviewers independently extracted data and assessed the quality of the included studies with the Cochrane risk-of-bias tools. The outcomes evaluated were postoperative redislocation rate, revision rate, complications, and Kujala score. We used traditional direct pairwise meta-analysis as well as network meta-analysis for comprehensive efficacy of all 3 treatment measures.
Results:
Twelve studies were included: 5 compared MPFL reconstruction with MPFL repair, 2 compared MPFL reconstruction with nonoperative treatment, and 5 compared MPFL repair with nonoperative treatment. The risk of bias was serious in 4, moderate in 4 and low in 4 articles. MPFL reconstruction led to significantly reduced redislocation and improved Kujala scores compared with MPFL repair and nonoperative treatment. MPFL repair led to reduced redislocation rates compared with nonoperative treatment but did not show an obvious benefit in primary dislocations. There was no significant difference among the 3 treatments in terms of revision rate and incidence of complications, although we found that treatment-related complications were least likely to occur in nonoperative treatment.
Conclusion:
The results of this review indicate that MPFL reconstruction decreases recurrent dislocation compared with MPFL repair or nonoperative treatment, but it has a higher possibility of complications. MPFL repair resulted in less postoperative redislocation than nonoperative treatment but did not show an obvious benefit in primary dislocation.
Keywords
The incidence of patellar dislocation is about 42 in 100,000 and is more common in girls between the ages of 10 and 17 years. 20,25 For the first time, patients with patellar instability have a tendency to develop recurrent patellar dislocation, and this is especially so in young patients. 17 Whether it is primary patellar dislocation or recurrent patellar dislocation, risk factors include acute traumatic episode, bony malalignment, and anatomic pathology. Dislocators with high risk factors are suitable for the surgical treatment of medial patellofemoral ligament (MPFL), which plays an important role in restraining the patella. 18,54 Patellar dislocation is always accompanied by structural abnormality or even tears of MPFL. 17 Therefore, the restoration of anatomic structure by MPFL is very important for the treatment of patellar dislocation. In addition, nonoperative treatment can accelerate the anatomic and functional recovery of impaired MPFL.
Treatments that have been described for patellar dislocation include MPFL reconstruction, MPFL repair, medial retinacular reefing, other associated bone correction surgery, soft tissue procedures, and nonoperative treatment. 39 Currently, MPFL reconstruction, MPFL repair, and nonoperative treatment are popular techniques. MPFL repair is considered technically less demanding with a lower risk of morbidity and could significantly reduce the redislocation rate and facilitate activity levels back to their preinjury states. 3,6,10,31 Similarly, MPFL reconstruction is also an effective surgical technique. 21,29,32,36 Our previous report showed that MPFL reconstruction was safe and effective in patients of all ages, without marked predisposing anatomic abnormalities and moderate/severe osteochondral lesions. 22 To date, some studies have compared the efficacy of MPFL reconstruction versus MPFL repair for patellar dislocation, 7,13,15,40,51 MPFL reconstruction versus nonoperative treatment, 5,56 and MPFL repair versus nonoperative treatment. 3,9,12,26,38 However, which technique performs best is still controversial.
We conducted this review to investigate the efficacy of MPFL reconstruction, MPFL repair, and nonoperative treatment for the treatment of patellar dislocation under the current evidence and to compare the efficacy of the treatments. Our hypothesis was that MPFL reconstruction has significant advantages in preventing postoperative redislocation and improving postoperative knee function among the 3 treatments. We further hypothesized that there would be no significant difference in revision rate and postoperative complications among the 3 treatments.
Methods
This systematic review and meta-analysis was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 33 In addition, this network meta-analysis (NMA) has been registered at International Prospective Register of Systematic Reviews (PROSPERO No. CRD42020199497).
Study Selection
We searched for published articles using the PubMed, Web of Science, Cochrane Library, Embase, CNKI (China National Knowledge Infrastructure), and Wanfang databases from inception to December 2020. The Medical Subject Headings terms patellar dislocation, patellar instability, medial patellofemoral ligament reconstruction, medial patellofemoral ligament repair, conservative treatment, and related free words were combined to search relevant papers. There were no language and data restrictions on our primary search. Furthermore, we did a manual retrieval to identify potentially relevant papers. The retrieval process was carried out by 2 independent authors (Z.L. and Q.Y.). If there were differences, a consensus would be reached with the help of another senior author (J.J.).
Inclusion and Exclusion Criteria
The criteria for inclusion in the study were as follows: (1) clinical comparative studies of MPFL reconstruction and repair in the treatment of patellar dislocation for direct comparison of the 2 surgical techniques; (2) clinical comparative studies of MPFL reconstruction and nonoperative treatment, or MPFL repair and nonoperative treatment for patellar dislocation; and (3) outcome indicators including 1 or more of the following: incidence of complications, redislocation rate, revision surgery rate, and Kujala Anterior Knee Pain Scale score. 27
The exclusion criteria were as follows: (1) cohort studies that focused on the efficacy of MPFL reconstruction or repair without control group; (2) other surgical techniques also used in the treatment (eg, tibial tubercle osteotomy [TTO], trochleoplasty, Roux-Goldthwait technique, or soft tissue techniques such as medial retinaculum pasty, medial reefing, or medial retinaculum plication); (3) in vitro biomechanical studies, animal studies, and cadaveric studies of reconstruction and repair in the treatment of recurrent patellar dislocation; and (4) articles that were not in English or Chinese.
Data Extraction
We extracted the following information: (1) study characteristics (year of publication, location, study design, and surgical techniques); (2) population characteristics (number of patients, sex, age, and follow-up time); and (3) outcome indicators (incidence of complications [patellofemoral fibrosis, infection, patellar or cartilage fracture caused by fixation], redislocation rate, revision rate, and Kujala score at the final follow-up). These data were independently extracted by 2 authors (Z.L. and L.H.) according to the standardized extraction form.
Risk-of-Bias and Methodologic Quality Assessment
The risk of bias in the included studies was assessed by 2 authors (Z.L. and Q.Y.) according to the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) and revised tool for assessing risk of bias in randomized trials (RoB 2), approved by the Cochrane Collaboration groups. 47,48
Statistical Analysis
The outcomes we evaluated were redislocation rate, revision rate, complications, and Kujala score. Risk ratios (RRs) and 95% CIs were calculated to evaluate the dichotomous variables (redislocation rate, revision rate, and complications). For continuous variables (Kujala score), the mean differences (MDs) and 95% CIs were used. The efficacy of the treatments was compared using traditional direct pairwise meta-analysis (DMA) as well as NMA to obtain the comprehensive efficacy of all 3 treatment measures. In addition, the heterogeneity between studies was evaluated by I 2 and the Cochrane Q statistic. 23 A statistically significant difference was indicated if the P value was ≤.05 and the 95% CI did not cross the null value of 1.
Since the included treatment can form a closed loop in NMA, we used an inconsistency factor to evaluate the heterogeneity of the included studies. 46 The Z test was used to evaluate inconsistency, with P ≤.05 indicating inconsistency. Funnel plots were used to assess whether publication bias or small sample-size effect existed. 16 We used the surface under the cumulative ranking probabilities to assess the possible ranking of the MPFL reconstruction, MPFL repair, and nonoperative treatment for patellar dislocation. 41 Considering the high clinical heterogeneity of the included original studies, the random-effects model was used to combine the effects.
With regard to subgroup analysis, there was a slight difference between primary and recurrent dislocation in the condition of pathology. As a result of the insufficient number of studies, only DMA was able to be used to compare MPFL reconstruction and MPFL repair for recurrent patellar dislocation. We were able to apply NMA to the studies on primary dislocation to compare clinical outcomes among the 3 treatment types. Stata 15.0 (Stata) was used to conduct the DMA and NMA.
Results
Identification of Studies
A total of 2355 articles were retrieved. Among these, 978 articles were duplicates. By reading the remaining 1377 titles and abstracts, articles that were not related to the purpose of the study were excluded; 5 papers were excluded because they used the retinaculum plasty technique, distal realignment technique duplication and additional augmentation, medial retinaculum reefing, and Roux-Goldthwait technique, and thus, they did not meet the inclusion criteria 30,34,35,43,45 ; 1 paper was excluded because some of the patients in the repair group underwent lateral release (LR), and the authors did not describe data for the remaining patients who underwent MPFL repair 37 ; and 1 paper was excluded because the reconstruction group used reconstruction combined with repair of medial retinaculum and LR. 8 Twelve articles were included for making NMA among reconstruction, repair, and nonoperative treatment. Ultimately, 5 articles 7,13,15,40,51 were included for DMA between MPFL reconstruction and MPFL repair, 5 articles 3,9,12,26,38 compared MPFL repair and nonoperative treatment, and 2 articles 5,56 compared MPFL reconstruction and nonoperative treatment. The details of the search process are shown in Figure 1.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart. CNKI, China National Knowledge Infrastructure; DMA, direct pairwise meta-analysis; LR, lateral release; NMA, network meta-analysis.
Characteristics of the Included Studies
Of the 12 studies for NMA, there were 6 randomized controlled trials (RCTs) 3,5,9,12,26,38 and 6 retrospective comparative studies (RCSs). 7,13,15,40,51,56 The year of publication was distributed from 2008 to 2019. A total of 142 knees of 141 patients were in the MPFL reconstruction group, 217 knees of 214 patients in the MPFL repair group, and 181 knees of 179 patients in the nonoperative group. The follow-up period for all studies ranged from 6 to 59.7 months. In the reconstruction group, 3 studies 7,13,51 used the transpatellar technique, 3 studies 15,40,56 used the suture anchor technique, and 1 study 5 used the nonabsorbable suture technique for patellar fixation. All 7 studies 5,7,13,15,40,51,56 used absorbable or nonabsorbable screws for femoral fixation. In the repair group, all 10 studies § used suture anchor to fix MPFL according to the position of the rupture, and 1 study 9 sutured the MPFL when the ruptured position was closed to patella. In the nonoperative group, all patients were immobilized for 2 to 4 weeks and had subsequent physical therapy (Table 1). 3,5,9,12,26,56
Characteristics of Included Studies a

a F, female; FF, femoral fixation; G, graft used for reconstruction; M, male; MPFL, medial patellofemoral ligament; Nonop, nonoperative treatment; NR, not reported; PF, patellar fixation; RCS, retrospective comparative study; RCT, randomized controlled trial; Recon, MPFL reconstruction; Repair, MPFL repair; SA, suture anchor.
Quality Assessment
The ROBINS-I was used to assess the quality of methodology for RCSs, which included the assessment of bias due to confounding, selection bias, classification of interventions, deviation bias, missing data bias, measurement bias, and reported bias in selection. The overall risk of bias for RCSs was serious in 4 studies 7,13,15,51 and moderate in 1 (Table 2). 40 RoB 2 was used to evaluate the bias of RCTs, which included randomization process, deviations from intended intervention bias, missing outcome data, and selection of reported result bias. The overall risk of bias for RCTs was moderate in 3 studies 3,5,26 and low in 3 (Table 3). 9,12,38
Risk of Bias Summary for Included RCSs Based on ROBINS-I

a RCS, retrospective comparative studies; ROBINS-I, Risk of Bias in Nonrandomized Studies of interventions.
Risk of Bias Summary for Included RCTs Based on RoB 2

RCT, randomized controlled trial; RoB 2, revised tool for assessing risk of bias in randomized trials.
Results of DMA
The results of the DMA are shown in Tables 4 to 6. A higher postoperative redislocation rate was seen after nonoperative treatment compared with MPFL reconstruction (RR, 0.11 [95% CI, 0.01-0.80]; I 2 = 0.0%) and MPFL repair (RR, 0.59 [95% CI, 0.35-1.00]; I 2 = 0.0%). The difference in redislocation rates between MPFL reconstruction and repair was not significant (RR, 0.39 [95% CI, 0.10-1.49]; I 2 = 10.3%) (Tables 4 and 6). There was no significant difference in complications, revision rate, or Kujala score among the three treatments (Tables 4 and 5).
High heterogeneity was seen in the Kujala score in the comparison of nonoperative treatment versus MPFL reconstruction and nonoperative treatment versus MPFL repair, whereas high heterogeneity was not seen in the other 3 clinical outcomes (I 2 = 0.0% [overall redislocation rate], 0.0% [overall revision rate], 0.0% [overall incidence of complications]) (Table 6).
Meta-Analysis of Redislocation, Revision, and Complications a

a MPFL, medial patellofemoral ligament; Nonop, nonoperative treatment; PD, primary dislocation; Recon, MPFL reconstruction; Repair, MPFL repair.
bP value for inconsistency.
c No closed loop existed.
d Significant difference (95% CI does not cross 1).
e Insufficient studies to conduct NMA.
Meta-Analysis of Kujala Score a
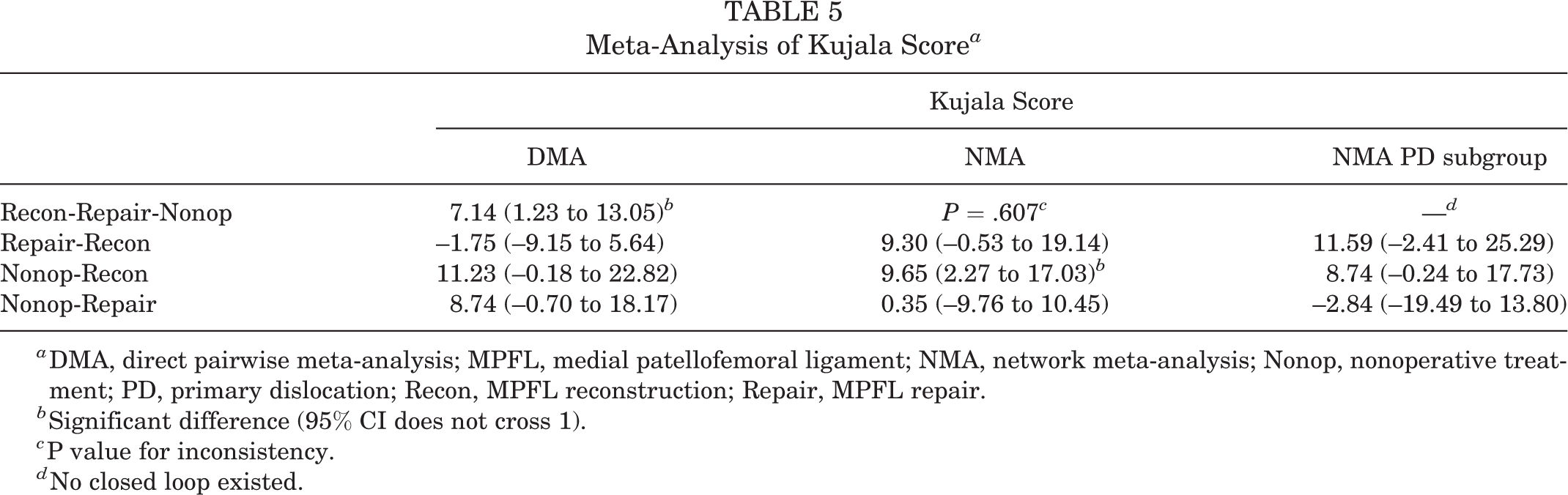
a DMA, direct pairwise meta-analysis; MPFL, medial patellofemoral ligament; NMA, network meta-analysis; Nonop, nonoperative treatment; PD, primary dislocation; Recon, MPFL reconstruction; Repair, MPFL repair.
b Significant difference (95% CI does not cross 1).
c P value for inconsistency.
d No closed loop existed.
Heterogeneity in DMA a

a DMA, direct pairwise meta-analysis; MPFL, medial patellofemoral ligament; Nonop, nonoperative treatment; Recon, MPFL reconstruction; Repair, MPFL repair.
b P value could not be calculated.
c Statistically significant difference between treatments according to DMA.
Results of Network Meta-analysis
No inconsistency was detected among any of the 4 outcome indicators (Tables 4 and 5). According to our results, MPFL repair had a higher risk of postoperative redislocation than nonoperative treatment (RR, 3.93 [95% CI, 1.40-11.07]; P value of inconsistency = .578). Nonoperative treatment has a higher risk of postoperative redislocation than MPFL reconstruction (RR, 0.51 [95% CI, 0.31-0.84]). Accordingly, when MPFL repair is compared with reconstruction, the risk of postoperative redislocation is higher (RR, 0.13 [95% CI, 0.04-0.39]) (Table 4). MPFL reconstruction led to significantly improved postoperative Kujala scores compared with nonoperative treatment (MD, 9.65 [95% CI, 2.27-17.03]; P value of inconsistency = .607). There was no significant difference in Kujala scores between MPFL reconstruction versus repair and nonoperative treatment versus repair (Table 5). There was no significant difference among the 3 treatments in terms of revision rate and complications.
Rank Possibility
In terms of preventing redislocation rate of the patella, reducing revision rate, and improving Kujala score, the rank possibility of MPFL reconstruction was the highest. In terms of preventing complications, nonoperative treatment seemed to be ranked first (Table 7).
Rank Possibility a

a MPFL, medial patellofemoral ligament; Nonop, nonoperative treatment; Recon, MPFL reconstruction; Repair, MPFL repair.
Subgroup Analysis
Because there are no articles on nonoperative treatment of recurrent patellar dislocation, only MPFL reconstruction versus repair could be compared for these patients. DMA showed that there was no difference between MPFL reconstruction and repair in preventing postoperative redislocation, revision surgery, and complications and in improving postoperative knee function.
In the comparison of 3 treatments for patients with an initial patellar dislocation, there was no significant difference in the postoperative redislocation rate after intervention with MPFL repair or nonoperative treatment (RR, 5.87 [95% CI, 0.74 to 46.49]), which was different from that of all patients with patellar dislocation after NMA (Table 4). There was no significant improvement in the Kujala score of MPFL reconstruction in patients with primary dislocation compared with nonoperative treatment (MD, 8.74 [95% CI, –0.24 to 17.73]), which was different from the NMA results of all patients (Table 5).
Discussion
The most important findings of this review were that, although there were no significant differences between MPFL reconstruction and repair in terms of postoperative redislocation rate, revision rate, Kujala score, and the occurrence of complications for patellar dislocation in DMA, the NMA did show a significant lower risk of recurrent dislocation in the MPFL reconstruction group. In the comparison of nonoperative treatment and MPFL reconstruction in DMA, there was significant statistical difference in the redislocation rate among the 4 outcome indicators, the significant differences between these 2 treatments were detected in terms of redislocation rate and Kujala score by using NMA technique. In the comparison of nonoperative treatment and MPFL repair in DMA, no significant differences were found in any of the outcome indicators, and only the redislocation rate showed a significant difference in NMA.
According to our results, we can see that MPFL reconstruction has relatively obvious advantages in preventing postoperative redislocation and improving postoperative knee joint function. As the rank possibility showed, MPFL reconstruction is probably the best treatment plan in preventing postoperative redislocation, reducing revision rate, and improving knee function score. Compared with the other 2 surgical treatments, nonoperative treatment would not cause infection, and patellar fracture was unlikely to occur; therefore, nonoperative treatment ranks relatively high in preventing the risk of complications (patellofemoral fibrosis, infection, or patellar or cartilage fracture caused by fixation).
Each treatment for patellar dislocation has its own unique characteristics. If risk factors such as trochlear shape, tibial tuberosity-trochlear groove (TT-TG) distance, and patellar height of the patients are normal; the MPFL is not completely torn; and the patient has only occasional instability, nonoperative treatment can be selected for the treatment of patellar dislocation. 3,44 Several studies have found that redislocation after treatment is a serious weakness in nonoperative treatment. ∥ At present, there is no consensus on how long to use a knee brace and how to carry out functional rehabilitation for nonoperative treatment of patellar dislocation. If the patient sustains injury of medial stabilizers, severe trochlear dysplasia, excessive TT-TG or patellar height, and severe cartilage injury, surgical intervention is necessary. 18 Dislocators with trochlear dysplasia, TT-TG >20 mm, patellar tilt, or patella alta are suitable not only for MPFL repair or reconstruction, but also, additional surgery such as TTO, trochleoplasty, or derotation osteotomy can or should be used.
MPFL repair is suitable for patients with fresh patellar dislocation with MPFL rupture at the attachment point of ligament or MPFL repairable. 1 The efficacy of MPFL repair in preventing postoperative redislocation has been recognized by some researchers. 1,6 However, there are some limiting factors in the choice of MPFL repair to some extent; for example, midsubstance MPFL ruptures or a scarred MPFL in chronic injuries can be difficult to repair. In addition, MPFL repair showed a high failure rate in patients with recurrent patellar dislocation and chronic patellar dislocation with a long natural history. 2,10 The use of autogenous or allogeneic tendons to refix the graft to the original anatomic position of MPFL by its reconstruction can be applied to all cases of MPFL ruptured, whether it is traumatic primary dislocation or recurrent dislocation. Although reconstruction is used widely, the complications of reconstruction, such as patellar fracture, 7 arthrofibrosis, 40 tunnel enlargement caused by graft loosening, 4 and femoral tunnel malposition, may require revision surgery. Revision surgery can improve stability, but subjective outcomes cannot be significantly improved and may even worsen. 11
According to the current studies, a standard consensus to correct patellar movement and instability has not yet been established. 14 Lee et al 28 investigated the efficacy of MPFL reconstruction versus soft tissue realignment surgery, including medial retinaculum pasty, MPFL repair, medial reefing, and medial retinaculum plication, in patients with patellar dislocation. The authors found significantly favorable Kujala scores after MPFL reconstruction compared with soft tissue realignment surgery (MD, –8.91 [95% CI, –14.05 to –3.77]; I 2 = 94%). Previtali et al 39 compared MPFL reconstruction with other soft tissue surgical techniques, including medial reefing, retinaculum plication, and retinaculum plasty and repair, and found no significant differences between the groups in redislocation (0.7% vs 2.9%) or minor complication (12% vs 9%) rates. In addition, they found more favorable Kujala scores for MPFL reconstruction than for soft tissue surgical techniques at short- and long-term follow-up (P < .001 for both). However, the soft tissue techniques in the above 2 studies included various surgical methods (medial reefing, retinaculum plication, retinaculum plasty, and repair), which was probably the greatest source of heterogeneity that may have influenced the outcomes. The low level of evidence in the original studies is also a cause of deviation in the results.
Tian et al 50 compared the efficacy of nonoperative treatment with MPFL repair in primary patellar dislocation in a systematic review and meta-analysis. They found that MPFL repair technique did not reduce the risk of postoperative redislocation, and MPFL repair led to better postoperative Kujala scores compared with nonoperative treatment (MD, –9.73; 95% CI, –15.90 to –3.57; I 2 = 85%). However, Tian et al 50 included in their review the study of Palmu et al 37 , in which 7 patients in the surgical group underwent only LR; moreover, Palmu et al 37 did not analyze data from these 7 patients separately. The occurrence of this situation may have affected the results of Tian et al. 50 Based on the existing DMA, researchers did not entirely agree on which treatment has a better clinical outcome; according to our analysis, the main reasons may be the level of evidence of the original studies, the risk of bias, and other surgical procedures that may be required for patellar dislocation, such as TTO, LR, and cartilage fracture refixation.
Arendt et al 2 found that MPFL repair has a high failure rate for patients with recurrent patellar dislocation with a long natural history. The authors speculated that the reason for the high failure rate of MPFL repair was the failure to correct the risk factors (patella alta and trochlear dysplasia). Camp et al 10 also found that the MPFL repair technique had a high failure rate for recurrent patellar dislocation. The authors believed that if TT-TG were taken into account, patients may benefit from TTO. TTO is also an effective surgical technique for the treatment of patellar dislocation, especially in patients with excessive TT-TG. 24,49 Other than TTO, trochleoplasty 42,52 and femoral osteotomy 53,55 are also useful surgical techniques for the treatment of patellar dislocation. These surgical techniques share the common feature of being able to change the anatomic structure of bones and correct bone deformities. From existing studies, bone-correction surgery plays a very important role in patients with primary or recurrent patellar dislocation.
On the basis of our combined results, we believe that it is very important to assess the risk factors associated with patellar dislocation before treatment. If the patient has risk factors, bone-correction surgery is necessary. Among the treatments designed to protect, repair, or reconstruct MPFL, MPFL reconstruction has obvious advantages in preventing postoperative redislocation and improving the function of the knee joint after surgery. However, if a patient has experienced only a primary dislocation, the advantage of MPFL reconstruction in improving knee joint function is no longer obvious. On the contrary, the possibility of complications of MPFL reconstruction will expose patients to some potential and unnecessary trouble. MPFL repair is not superior to nonoperative treatment in the prevention of postoperative redislocation in patients with primary patellar dislocation.
Strengths and Limitations
A strength of our study is that it is the first NMA to compare the clinical outcomes of nonoperative treatment, MPFL repair, and MPFL reconstruction. We retrieved all clinical comparative studies including nonoperative treatment, MPFL reconstruction, and MPFL repair. Our study was performed in strict accordance with the PRISMA statement.
There were four limitations to our study. First, although all databases in English and Chinese were searched, the number of included studies and sample sizes were still relatively low. Second, the different surgical techniques of MPFL reconstruction among the included studies were the greatest source of heterogeneity. The patellar fixation and femoral fixation in MPFL reconstruction were different among included studies. The main reason for the high heterogeneity of the continuous variable Kujala score is that the final score was obtained through patient description or physical examination by doctors, the patient had no medical background, and the score was not evaluated separately by 2 doctors. Third, the quality of included studies for comparing MPFL reconstruction with repair was relatively low, which was possibly the main reason why the results of DMA differed from those of NMA. Fourth, there were no controls for risk factors, and patients requiring bony procedures (TTO, trochleoplasty, derotation osteotomy, etc) were not included in our study.
Above all, future studies should focus on (1) creating a more scientific and reasonable rehabilitation program for nonoperative treatment; (2) improving the biomechanical strength of MPFL repair; and (3) refining technique to reduce the risk of complications of MPFL reconstruction.
Conclusion
For patients with patellar dislocation, MPFL reconstruction decreases recurrent dislocation compared with MPFL repair or nonoperative treatment, but it has a higher possibility of complications. MPFL repair results in less postoperative redislocation than nonoperative treatment but does not show an obvious benefit in primary dislocation.
Footnotes
Final revision submitted February 9, 2021; accepted February 28, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the National Natural Science Foundation of China (81874017, 81960403, and 82060405); Natural Science Foundation of Gansu Province of China (20JR5RA320); Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (CY2017-ZD02, CY2017-QN11, CY2020-BJ03); Traditional Chinese Medicine Inheritance and innovation platform construction project (TCM-IPC-2020-03); and Lanzhou science and technology development guiding plan project (2019-ZD-58). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.