
Abstract
Background:
The drilling technique used to make a femoral tunnel is critically important for determining outcomes after anterior cruciate ligament (ACL) reconstruction. The 2 most common methods are the transtibial (TT) and anteromedial (AM) techniques.
Purpose:
To determine whether graft orientation and placement affect clinical outcomes by comparing clinical and radiological outcomes after single-bundle ACL reconstruction with the AM versus TT technique.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
Articles in PubMed, EMBASE, the Cochrane Library, ISI Web of Science, Scopus, and MEDLINE were searched from inception until April 25, 2020, using the following Boolean operators: transtibial OR trans-tibial AND (anteromedial OR trans-portal OR independent OR three portal OR accessory portal) AND anterior cruciate ligament.
Results:
Of 1270 studies retrieved, 39 studies involving 11,207 patients were included. Of these studies, 14 were clinical, 13 were radiological, and 12 were mixed. Results suggested that compared with the TT technique, the AM technique led to significantly improved anteroposterior and rotational knee stability, International Knee Documentation Committee (IKDC) scores, and recovery time from surgery. A higher proportion of negative Lachman (P = .0005) and pivot-shift test (P = .0001) results, lower KT-1000 arthrometer maximum manual displacement (P = .00001), higher Lysholm score (P = .001), a higher incidence of IKDC grade A/B (P = .05), and better visual analog scale score for satisfaction (P = .00001) were observed with the AM technique compared with the TT technique. The AM drilling technique demonstrated a significantly shorter tunnel length (P = .00001). Significant differences were seen between the femoral and tibial graft angles in both techniques. Low overall complication and revision rates were observed for ACL reconstruction with the AM drilling technique, similar to the TT drilling technique.
Conclusion:
In single-bundle ACL reconstruction, the AM drilling technique was superior to the TT drilling technique based on physical examination, scoring systems, and radiographic results. The AM portal technique provided a more reproducible anatomic graft placement compared with the TT technique.
Keywords
The anterior cruciate ligament (ACL) is the most frequently injured ligament of the knee. 46 Injuries to the ACL can lead to progressive instability of the knee and may result in lengthy rehabilitation and increased risk for early onset of posttraumatic knee osteoarthritis. 35,40 ACL reconstruction is often recommended to achieve knee stability, particularly for young patients with a high activity level and those who cannot adjust to instability. 7,49,89 Arthroscopic ACL reconstruction is widely accepted as the treatment of choice to address this problem.
The optimal surgical technique for ACL reconstruction remains a topic of controversy. Various arthroscopic ACL reconstruction techniques are available, but no standards are acknowledged regarding the superiority of graft choice, graft position, or number of femoral and tibial tunnels or the use of fixation materials in ACL reconstruction. 13,86 Two approaches for drilling the femoral tunnel are commonly used in single-bundle ACL reconstruction: creating the femoral tunnel through the tibial tunnel (ie, transtibial [TT] technique) or placing the femoral tunnel through a low anteromedial (AM) arthroscopic portal. 18
The success rate of single-bundle ACL reconstruction reported in the literature is between 69% and 95%. 34,62 Unsuccessful cases seem to be due to nonanatomic placement of the graft. If anatomic considerations are neglected during ACL reconstruction, residual rotational instability may remain despite the restoration of anteroposterior stability. 38 Several biomechanical and cadaveric studies 9,39,68 have pointed to superior graft positioning using the AM technique.
Therefore, correct positioning of the femoral tunnel is critical for a successful single-bundle ACL reconstruction. Positioning of the femoral tunnel during ACL reconstruction is considered a key factor in postoperative knee function and restoration of the physiological and kinematic parameters of the femorotibial joint. 12,26,32,47 Vertical ACL graft angles resulting from improper location of the femoral tunnel in the sagittal and frontal plane have been associated with inferior outcomes. 8,12,14 Both the anteroposterior and the rotational stabilities of horizontal grafts were found to be superior to those of vertical grafts. 3,9,25,53 The importance of the femoral tunnel position in the sagittal plane in ACL reconstruction was recognized many years ago, and incorrect position of the femoral tunnel yields poor clinical results. 23,26
The AM technique has been advocated to obtain a more anatomic ACL reconstruction, which could improve rotational knee stability and kinematics, resulting in a better clinical outcome. 3,15 Moreover, evidence in the literature points to high revision rates after nonanatomic placement of the ACL graft, 60 highlighting the inadequacy of the TT drilling technique regarding placement within the native femoral and tibial footprints. 1,3 Proper positioning of the femoral tunnel during ACL reconstruction is essential, and nonanatomic tunnel placement is cited as the most common cause of clinical failure secondary to pain and persistent instability. 2
The purposes of this study were to conduct a systematic review of clinical and radiological evidence directly comparing the AM and TT femoral drilling techniques in ACL reconstruction and to evaluate whether differences in graft or tunnel angle produce differences in clinical outcome after ACL reconstruction. We hypothesized that creating femoral tunnels with the AM drilling technique would provide a more anatomic femoral tunnel position and superior overall outcomes compared with using the TT technique.
Methods
Literature Search
The study design followed the recommendations in the Cochrane Review Methods. According to the guidelines of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement, several comprehensive literature databases, including PubMed, EMBASE, the Cochrane Library, ISI Web of Science, Scopus, and MEDLINE, were searched from inception to April 25, 2020, for studies evaluating tunnel drilling (AM vs TT) in patients who underwent arthroscopic ACL reconstruction. All reference lists in the literature were manually searched for articles potentially missed by the electronic search. No restrictions were placed on language or year of publication. The search used the following Boolean operators: transtibial OR trans-tibial AND (anteromedial OR transportal OR independent OR three portal OR accessory portal) AND anterior cruciate ligament.
Literature Selection
All potential studies were imported into Endnote X7 (Clarivate), and duplicates were removed. Two researchers (M.L. and R.L.) independently excluded studies based on titles and abstracts using Covidence (the primary screening and data extraction tool for Cochrane authors). If the abstract did not provide sufficient data to determine selection, the complete article was reviewed. Studies were included in the analysis if (1) they included patients who underwent primary, arthroscopic, single-bundle ACL reconstruction with AM and TT femoral drilling techniques; (2) they evaluated the femoral tunnel with validated imaging tools such as plain radiography and 3-dimensional (3D) imaging (computed tomography [CT] or magnetic resonance imaging [MRI]); and (3) they reported parameters including means, standard deviations, and sample numbers. In studies that compared single- and double-bundle reconstruction, only the results of single-bundle reconstruction were included. The exclusion criteria were as follows: (1) studies that did not provide comparative data; (2) studies on double-bundle ACL reconstruction; (3) studies that entailed ACL injury accompanied by posterior cruciate ligament, medial collateral ligament, or lateral collateral ligament injuries; (4) studies that did not report postoperative clinical or radiological outcomes; and (5) biomechanical studies or studies that included only cadaveric results.
In assessing and organizing the pooled studies, we noted the country and city of the hospital or institution at which the arthroscopic surgeries were performed, the operating surgeon’s name in the studies, and the evaluation period, in order to exclude duplicate cohorts of patients. If the same patient cohort was evaluated in more than 1 study, only the latest study with the longest follow-up period was included.
Data Extraction and Assessment of Study Quality
Two researchers (M.L. and R.L.) independently assessed all potentially suitable studies using a predesigned sheet to perform data extraction and eliminated the studies that did not satisfy the selection criteria. Disagreements were resolved by discussion with the other 2 researchers (R.D. and M.E.H.). Extracted data included first author, year of publication, research type, level of evidence, average age of patients, patient sex, sample size, follow-up duration, mean time from injury to surgery, type of implant, source of implant, International Knee Documentation Committee (IKDC) subjective and/or objective score, KT-1000 arthrometer maximum manual displacement, visual analog scale (VAS) score for satisfaction, stability of knee joint, Lachman test, pivot-shift test, Lysholm score, Tegner activity scale score, Knee injury and Osteoarthritis Outcome Score (KOOS), revision rate, recovery time from surgery, time from surgery to return to play, ACL quality of life, and intra- and postoperative complications.
Radiographic data included imaging technique, tunnel center from the center of the ACL attachment (the center of the ACL was within 2 mm of an arthroscopic reference point located at the junction of a line drawn distally from the most proximal corner of the articular margin on the lateral wall of the notch and a perpendicular line drawn to the most posterior point of the condyle), femoral graft angle (FGA), tibial graft angle (TGA), ACL angle of the normal knee on sagittal MRI view, diameter of the tibial or femoral tunnel on 3D images, length of the tibial or femoral tunnel, KOOS result, tunnel widening, and osteoarthritis. The FGA was defined as the angle between the axis of the femoral tunnel and the joint line in the coronal plane, whereas the TGA was defined as the angle between the axis of the tibial tunnel and a line perpendicular to the long axis of the tibia in the sagittal plane.
Quality Assessment
Two investigators (R.L. and M.L.) independently assessed the methodological quality of each study according to a 12-item scale. 19 Methodological quality was categorized a priori as follows for all studies: a score of 0 to 4 was considered low quality, 5 to 8 moderate quality, and 9 to 12 high quality. Disagreements were evaluated by the kappa test, and consensus was reached by discussion with the other 2 investigators (R.D. and M.E.H.). The use of patient and care provider blinding could not be ensured from the 12-item list of standards, and no intention-to-treat analysis was performed in any of the included trials.
Statistical Analysis
RevMan 5.3 software (Review Manager [RevMan]; Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) was used to perform data analysis. For continuous variables, the weighted mean difference (WMD) was used to present analytical results, and the random-effects model with 95% CI was applied to the analysis; for dichotomous variables, the odds ratio (OR) was used to present analytical results, and the random-effects model with 95% CI was applied to the analysis. The I2 statistic was used to assess study heterogeneity. If I2 was 0% to 40%, heterogeneity was deemed to have a small effect on the variance in study estimates (and thus, differences were more likely to be due to a true effect). An I2 of 30% to 60% indicated moderate heterogeneity, and an I2 of 50% to 90% indicated substantial heterogeneity. If I2 was 75% to 100%, heterogeneity was thought to have a very high effect on the variance (and thus, any differences found were more likely to be due to heterogeneity between studies rather than a real effect). 33,82 The importance of the observed value of I2 depends on the magnitude and direction of effects and the strength of evidence for heterogeneity (eg, P value from the chi-square test, or a confidence interval for I2). P < .05 was considered significant.
Results
Search Results
The literature search initially yielded 1270 relevant citations (Figure 1). Among those, 802 duplicate articles were identified and removed from the search. After the removal of duplicate articles, 468 articles remained and were subject to the application of the predetermined inclusion and exclusion criteria. After the application of these criteria, 58 articles were subject to a full-text screening process, and from these, 19 trials were excluded. One randomized controlled trial (RCT) 28 used both single-bundle and double-bundle reconstruction and the AM drilling technique; thus, only the single-bundle data were extracted. Ultimately, 39 trials met the predetermined eligibility criteria (Figure 1). Of these, 14 reported only clinical outcomes, 13 reported only radiologic findings, and 12 reported both.

Flowchart of the literature search and study selection using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
A total of 8 RCTs, 21,24,28,43,48,76,79,87 3 prospective nonrandomized studies, 35,70,71 and 28 retrospective comparative studies ∥ were retrieved. Overall, 9 studies that explicitly used randomization and allocation concealment were considered high-quality studies, ¶ and the remaining 31 studies were of moderate quality # (see Table S1, available as Supplemental Material). The weighted kappa for agreement between the investigators regarding study quality was 0.81 (95% CI, 0.73-0.89).
Patient Population and Study Characteristics
The characteristics of the patients in the 39 studies are presented in Supplemental Table S2. A total of 11,207 patients were included in this review: 2549 in the TT group and 8598 in the AM group. Of the 11,207 patients, 10,543 patients were included in the clinical studies (n = 25) and 664 patients in the radiological studies (n = 14). The majority of patients included in the studies were male (65%; 6735/10,398), and the mean age per study ranged from 21.5 years 35 to 33.4 years. 29 The mean follow-up ranged from 6 months 29 to 78 months. 17
Surgical Technicalities
All studies included in this systematic review compared the AM and TT drilling techniques for single-bundle ACL reconstruction. The graft choice included hamstring autograft (71.8%), bone–patellar tendon–bone (BPTB) autograft (20.5%), BPTB allograft (2.6%), tibialis posterior allograft (2.6%), and Achilles tendon allograft (2.6%). Two studies (5%) did not specify which type of graft was used 1,66 (Supplemental Table S2).
Physical Examinations: Stability
Among the 25 clinical studies, 12 ** (48%) used the Lachman test as a benchmark to examine postoperative ACL sagittal laxity grade, and 13 studies †† (including the 12 studies that performed the Lachman test) used the pivot-shift test to examine rotational stability of the knee at the final follow-up (Supplemental Table S3). None of the other 12 studies reported either Lachman test or pivot-shift test results. Fewer patients who received the TT technique had negative Lachman test results (n = 894; mean value [MV] = 25%; OR, 0.54 [95% CI, 0.38-0.76]; P = .0005) (Figure 2A) and negative pivot-shift test results (n = 9791; MV = 51%; OR, 0.52 [95% CI, 0.38-0.71; P = .0001) (Figure 2B) compared with those who received the AM technique.

Forest plots of (A) negative Lachman test, (B) negative pivot-shift test, and (C) KT-1000 arthrometer measurement, for transtibial (TT) versus anteromedial (AM) drilling techniques, using the Mantel-Haenszel (M-H) statistical method and random-effects analysis model.
Of the 25 clinical studies, 9 3,17,21,24,28,37,49,51,87 (36% of all clinical studies) described KT-1000 arthrometer results (Figure 2C and Supplemental Table S3). Based on these studies, the maximum manual displacement was 2.27 mm in the TT group and 1.54 mm in the AM group. A pooled analysis of these studies resulted in an increased maximum manual displacement after the TT technique (n = 699; WMD, 0.39 [95% CI, 0.23-0.56]; P = .00001) (Figure 2C). Low to moderate heterogeneity was found for patients who had negative results on the pivot-shift test (I2 = 37%) and high maximum manual displacement (I2 = 73%).
Functional Outcomes: Scoring Systems
The Lysholm knee score was analyzed as a continuous variable in 18 articles (72% of all clinical studies), ‡‡ where a total of 1331 of patients were included in the comparison of TT and AM techniques (Supplemental Table S3). The overall Lysholm score was 89.4 for patients in the TT group and 92.3 for those in the AM group.
A meta-analysis of these articles indicated statistically significant differences in Lysholm knee score between the TT and AM groups (n = 1311; WMD, –1.81 [95% CI, –2.90 to –0.72]; P = .001). The data showed a certain degree of heterogeneity within the tolerance interval (P = .0001; I2 = 70%) (Figure 3A).
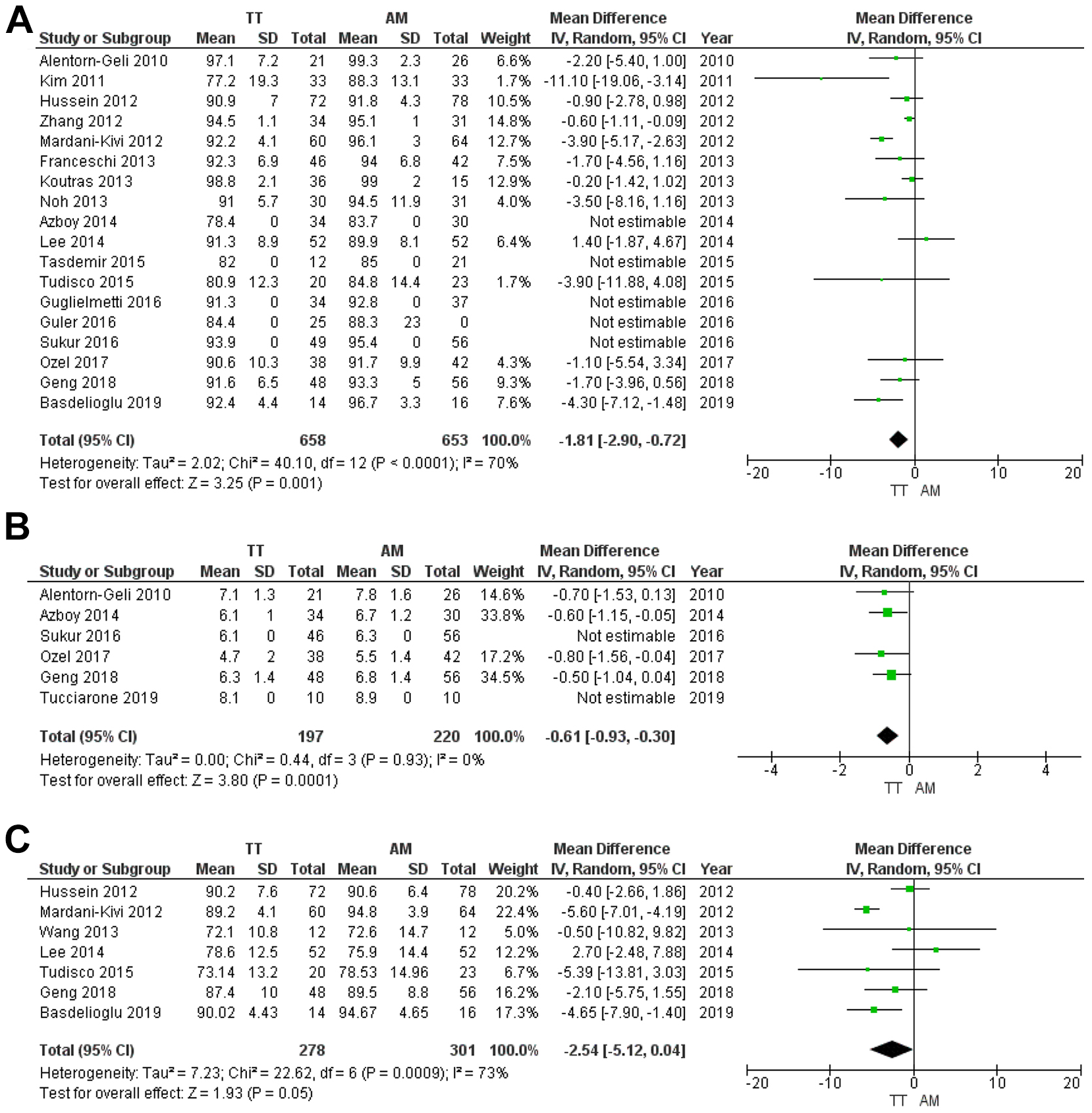
Forest plots of (A) Lysholm scores, (B) Tegner scores, and (C) International Knee Documentation Committee subjective scores for transtibial (TT) versus anteromedial (AM) drilling techniques, using the inverse variance (IV) statistical method and random-effects analysis model.
The Tegner score was analyzed as a continuous variable in 6 articles 3,6,21,51,72,76 (24% of all clinical studies), where 417 patients were included in the comparison between the TT and AM techniques (Figure 3B). The overall Tegner score was 6.22 for patients in the TT group and 6.78 for those in the AM group. According to the study results, statistically significant differences were seen in Tegner scores between the TT and AM groups (n = 295; WMD, –0.61 [95% CI, –0.93 to –0.30]; P = .0001). The data showed low heterogeneity (P = .93; I2 = 0%) (Figure 3B).
In total, 17 studies §§ (68% of all clinical studies) used the IKDC system, and 10 studies 7,21,24,28,37,45,72,74,78,83 reported the grade results: A, normal; B, nearly normal; C, abnormal; and D, severely abnormal (Supplemental Table S3). A total of 7 studies 3,6,17,31,43,44,48 included subjective scores in their results. Fewer patients had IKDC grade A/B after the TT technique than after the AM technique, but no intergroup difference was found in IKDC scores (n = 579; WMD, −2.54 [95% CI, −5.12 to 0.04]; P = .001) (Figure 3C). A total of 4 studies (16% of all clinical studies) reported VAS scores expressing patient satisfaction with the surgery (Figure 4A and Supplemental Table S3).The mean VAS score was 8.8 in the TT group and 9.3 in the AM group. A pooled analysis of these studies showed that the VAS score was lower after surgery with the TT technique (n = 340; WMD, −0.34 [95% CI, −0.47 to −0.20; P = .00001) (Figure 4A). Low heterogeneity was found for VAS score results (P = .22; I2 = 33%).

Forest plots of (A) visual analog scale scores for satisfaction, (B) return to sports time, and (C) time from surgery to normal life for transtibial (TT) versus anteromedial (AM) drilling techniques, using the inverse variance (IV) statistical method and random-effects analysis model.
Return to sports time was reported in 6 studies (24% of all clinical studies). 3,6,44,45,72,76 The mean time from surgery to return to sports was 9 months in the AM group and 10 months in the TT group. The meta-analysis showed no significant differences between the groups (Figure 4B). Use of the AM technique significantly improved the recovery time from surgery to normal life compared with the TT technique (n = 171; WMD, 0.78 [95% CI, 0.53-1.03]; P = .00001) (Figure 4C).
Revisions
Among the 25 clinical studies, ** †† 4 (16% of all clinical studies) reported the incidence of revision. 16,17,24,71 The overall revision rate was 5.9% (442/7498 patients) in the AM group and 6.2% (94/1508 patients) in the TT group. Meta-analysis revealed no significant differences between the groups (n = 9006; OR, 1.05 [95% CI, 0.76-1.45]; P = .76) (Figure 5). The data showed low heterogeneity (P = .55; I2 = 0%).
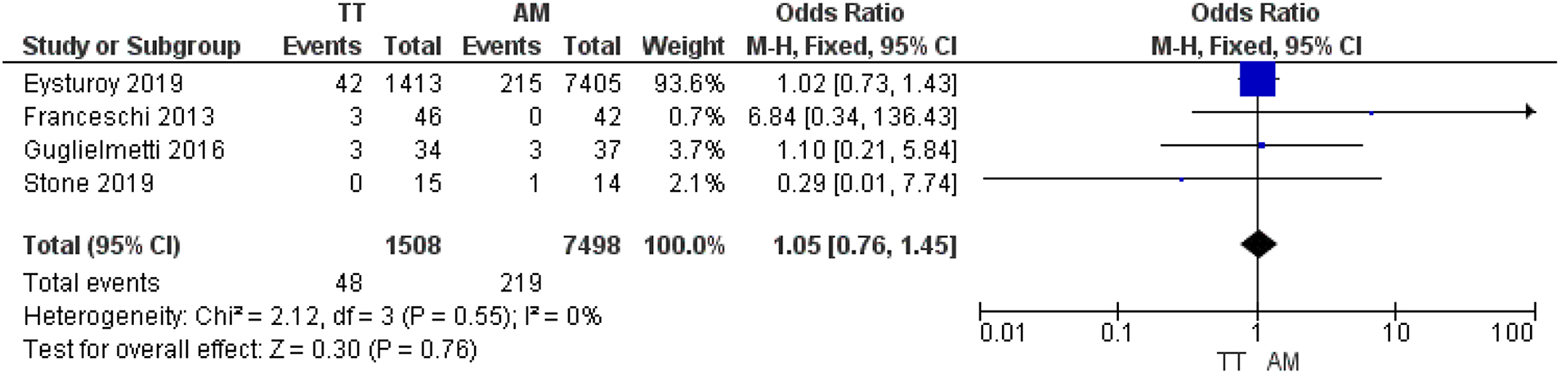
Forest plot of revision rates for transtibial (TT) versus anteromedial (AM) drilling techniques, using the Mantel-Haenszel (M-H) statistical method and random-effects analysis model.
Radiographic Outcomes
The radiographic outcomes reported in the included studies are summarized in Supplemental Table S4. In almost all cases, the FGA was measured by MRI (86%); in 1 case, the FGA was measured by CT. Within the 14 radiological studies,
∥∥
10 studies
¶¶
analyzed the FGA in both surgical techniques. Based on these studies, the mean FGA was 51.8° in the AM group and 63.3° in the TT group. According to the study results, statistically significant differences were seen in FGA between the TT and AM groups (n = 478; WMD, –16.79 [95% CI,

Forest plots of (A) femoral graft angle, (B) tibial graft angle, and (C) femoral tunnel length for transtibial (TT) versus anteromedial (AM) drilling techniques, using the inverse variance (IV) statistical method and random-effects analysis model.
The TGA was analyzed as a continuous variable in 5 articles (36% of all radiological studies),
26,29,53,71,80
where a total of 220 of patients were included in the comparison between the TT and AM techniques. According to the study results, the mean TGA was 59° in the AM group and 61° in the TT group. Meta-analysis of these articles indicated statistically significant differences in TGA between the TT and AM groups (n = 268; WMD,
Only 4 studies (29% of all radiological studies) reported the tunnel length (Supplemental Table S4). Based on these studies, the mean tunnel length was 36.8 mm in the AM group and 43.9 mm in the TT group. A pooled analysis of these studies revealed shorter tunnel length after the AM technique (n = 217; WMD, 5.44 [95% CI, 4.22-6.67]; P = .00001) (Figure 6C).
The occurrence of osteoarthritis on radiographic evaluation was reported by only a single study 17 (Supplemental Table S5). At the 6-year follow-up, the authors reported no significant difference between the 2 techniques (28.2% of patients in the TT group and 11.9% of patients in the AM group). The authors showed grade 1-2 degenerative changes according to the Fairbank grading system (P = .06, χ2 test). No patient in either group showed Fairbank grade 3 osteoarthritis.
Tunnel widening was reported by only a single study. Ozel et al 51 reported no significant differences between the AM and TT groups (1.2 ± 0.47 mm and 3.0 ± 0.9 mm, respectively) (Supplemental Table S4). Those authors found that femoral tunnel widening was significantly associated with anterior joint instability when all of the patients were evaluated as a single cohort (P < .001).
Regarding outcomes with respect to ACL graft placement in both the AM and the TT groups, 5 radiological studies 2,26,66,70,79 concluded that the optimal tunnel location was more often reproduced with the AM technique. This enables a more horizontal or oblique position close to the native ACL.
Complications
The overall complication rate was 3.4%. The infection rate was 3.3% and 2.9% for the AM and TT groups, respectively. Intraoperative complications were reported in only 1 study 16 (11.9% in the AM group vs 13% in the TT group) in which hamstring autograft was used (Supplemental Table S5). These were neurosensory disturbances caused by damage to the infrapatellar branch of the saphenous nerve.
Discussion
The key finding of this systematic review was that the AM technique for ACL reconstruction was superior to the TT technique based on postoperative functional and radiological results in terms of the sagittal and rotational stability of the knee. Specifically, the AM technique resulted in better objective stability. Accordingly, the Lachman test, the pivot-shift test, and the KT-1000 arthrometer test results were significantly improved; however, statistically significant differences may not be clinically relevant. Similarly, a review study by Alentorn-Geli et al 3 found that the AM technique resulted in better KT-1000 arthrometer and Lachman test results, greater knee range of motion, and earlier return to activity than the TT technique at 1- to 2-year follow-up.
Furthermore, the AM technique resulted in improvements in the Lysholm knee score, Tegner activity score, and VAS score. However, the TT and AM group difference for these results was small and may not be clinically meaningful: 2.9, 0.6, and 0.5, respectively.
In total, 4 studies analyzed the use of drilling techniques and their association with the risk of revision 15,17,24,71 and complications. 6,17,45 No differences in revision and complication rates were reported between both groups. Moreover, this systematic review showed no significant difference in time to return to sport between the 2 techniques.
The method of creating the femoral tunnel is one of the most important topics in ACL reconstruction. Some radiographic studies have revealed that drilling the femoral tunnel through the AM arthroscopy portal rather than using a TT drilling technique resulted in a graft position more posterior and closer to a position that has been suggested as favorable on a lateral radiograph of the knee. 2,26,59,61,66,70,79,84 In the frontal plane, the bone tunnel is inclined more toward the lateral cortex of the lateral femoral condyle when drilled through the AM portal, eventually resulting in superior rotatory stabilization of the knee joint compared with TT drilling. 12 In general, it is difficult to accurately identify the tunnel location on 2-dimensional images (radiograph, CT, or MRI) and impossible to accurately measure tunnel diameter (the tunnels appear as ellipses on the axial images). The tibial tunnel can be placed in an anatomic position with the TT technique. The tibial tunnel is made in the same way in the TT and AM techniques. Obtaining an anatomic femoral tunnel position using the TT technique is more difficult, 57,65 and the nonanatomic ACL will lead to abnormal knee kinematics, placing additional force on the graft. According to these radiological studies, 10,50,75,85 the AM technique might be superior in terms of positioning the ACL femoral tunnel at the center of the native ACL footprint and probably allows for creation of the femoral tunnel in a more anatomic position. Silva et al 67 reported that compared with the TT technique, the AM technique places the femoral and tibial tunnels more centrally in the ACL footprint, allowing better control of the anteroposterior and rotational stability of the knee and therefore improving the long-term clinical outcome. Alentorn-Geli et al 3 found that the oblique 10-o’clock position restored rotational knee stability better than the 11-o’clock position.
Schairer et al 63 used MRI to evaluate the translational and rotational kinematics of ACL-reconstructed knees with single-bundle TT and AM femoral tunnel drilling techniques. The investigators found that knee kinematics were better restored with the AM technique than with the TT technique, which resulted in increased knee laxity. Vignos et al 81 found that nonanatomic graft geometry was linked to asymmetric knee mechanics. Those authors suggested that restoring the native ACL geometry may be essential to mitigate the risk of early cartilage degeneration in these patients. However, the AM technique is independent of the respective tibial tunnel position, allowing more anatomic graft position, which may play a role in decreasing rerupture rates. 30 An AM tunnel is more precise and closer to the anatomic femoral ACL insertion than a TT tunnel, allowing for a more horizontal placement. 59,73 It was recently proposed that vertical and anterior graft placement is required for the TT technique owing to drilling through the tibial tunnel, increasing biomechanical demand during rehabilitation. 58 A vertical graft orientation leads to worse clinical outcomes (pivot shift, KT-1000 arthrometer measurements, and Lysholm score) compared with a more oblique graft placement. 36
According to the results of this systematic review, the AM technique has many advantages and disadvantages. A significant advantage is the independent placement of femoral and tibial tunnels 11,42,45,77 and more accurate and anatomic horizontal placement of the ACL femoral insertion. 3,11,20,27,35,41,45,54 Another advantage is that the tunnel placement is independent of graft type, fixation devices, or tunnel guides, 3,11,27,41,77 and drilling with the AM technique results in a shorter tunnel and decreased tunnel widening. 27,77 For the surgeon, using the AM technique makes it easier to put the graft in the right place but requires drilling in hyperflexion to reduce the risk of posterior wall blowout. 3,88 The AM technique provides better anteroposterior stability as assessed by Lachman and KT-1000 arthrometer testing at 1 to 2 years, as well as improved anteroposterior and rotational stability 3,17,64 and visualization of the native footprint without excessive notchplasty. 17 A substantial disadvantage of using the AM technique for ACL reconstruction is that it is technically demanding. 11,22,77 Another drawback is the limited visibility of the notch area, and excessive angulation in the sagittal plane may lead to tunnel enlargement from erosion. 20 A frequent criticism of the AM technique is the difficulty of seating the endoscopic aimer 42,54 and the inability to maintain the aimer in a hyperflexed knee. 42 Another drawback of the AM technique is the portal tightening in hyperflexion and difficulty viewing in hyperflexion. ##
When using an AM drilling technique, surgeons must be aware of the possibility of a short femoral tunnel length 3 ; however, no significant differences regarding intra- and postoperative complications and revisions were demonstrated here. Several studies have compared the femoral tunnel position using different techniques, a although few studies have investigated the graft angle inclination. 53,55,69 In addition, the influence of graft positioning on ACL reconstruction clinical outcomes is still debated. Snoj et al 69 observed a relationship between increased graft inclination in ACL reconstruction and anterior tibial translation, a condition correlating with poor clinical outcomes, whereas Araujo et al 4 reported increased graft forces, possibly associated with greater risk of ruptures, when anatomic positioning was used.
During an ACL reconstruction, tunnels made with the TT technique are more vertical to the femoral and tibial axial plane than those made with the AM technique. 5 With the TT technique, the femoral tunnel position is dictated by the tibial tunnel, whereas the AM technique provides the surgeon with greater freedom to place the graft in the anatomic position. 26,27
Strengths
This is the first comprehensive systematic review analyzing the correlation between clinical and radiological outcomes after single-bundle ACL reconstruction using the AM and TT drilling techniques. The use of multiple databases, a broad search strategy, and a duplicate systematic approach to reviewing the literature ensured that relevant articles were not overlooked. Excellent agreement at all screening stages and quality assessment was obtained.
Limitations
Some limitations should be acknowledged, such as the inclusion of retrospective studies that lacked randomization and blinding. Some studies included in the systematic review had modest sample sizes, and there was statistically significant heterogeneity due to the differences in research design, patient diversity, and surgical plans. The studies had relatively short follow-up periods, thus failing to provide long-term clinical evidence. Greater consistency in reporting outcomes across studies of all drilling techniques is needed to allow more definitive analyses. Future studies should use large prospective cohorts and randomized controlled designs with long-term follow-up to further assess the results presented in this review. As well, future studies should provide more consistent reporting of essential information, such as functional and radiological outcomes, as these results are often lacking in the currently available literature.
Conclusion
The literature presented in this review suggests that the AM drilling technique is superior to the TT technique in creating reproducible anatomic femoral tunnel placement during single-bundle ACL reconstruction. Compared with the TT drilling technique, the AM drilling technique resulted in better objective knee laxity and modestly better Lysholm scores but equal IKDC scores. Low overall complication and revision rates were seen in both techniques.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211024591 - Clinical and Radiological Outcomes of Anteromedial Portal Versus Transtibial Technique in ACL Reconstruction: A Systematic Review
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211024591 for Clinical and Radiological Outcomes of Anteromedial Portal Versus Transtibial Technique in ACL Reconstruction: A Systematic Review by Marios Loucas, Rafael Loucas, Riccardo D’Ambrosi and Michael Elias Hantes in Orthopaedic Journal of Sports Medicine
Footnotes
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Final revision submitted February 14, 2021; accepted February 28, 2021.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.