
Abstract
Background:
Femoral nerve block (FNB) and adductor canal block (ACB) have been used increasingly for pain control during anterior cruciate ligament (ACL) reconstruction in adolescent patients. However, recent evidence suggests that the use of FNB may affect quadriceps strength recovery 6 months after surgery.
Purpose/Hypothesis:
To compare postoperative isokinetic strength in adolescents who received FNB, ACB, or no block for perioperative analgesia during ACL reconstruction. We anticipated lower postoperative quadriceps and hamstring isokinetic deficits in adolescents who received FNB as compared with ACB.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients were included in the study if they had undergone hamstring tendon autograft ACL reconstruction by a single surgeon from July 2008 to January 2018 and if they underwent isokinetic muscle testing at 4 to 8 months postoperatively. The participants were divided into 3 groups (no block, FNB, and ACB), and we compared the deficit in percentages between the affected and unaffected limbs as calculated from the isokinetic quadriceps and hamstring strength testing at 60 and 180 deg/s. Between-group analysis was performed using analysis of variance, with an alpha of .05.
Results:
A total of 98 participants were included in the analysis (31 no block, 36 FNB, and 31 ACB). The mean ± SD age of the patients was 15.26 ± 1.15, 15.50 ± 1.42, and 15.71 ± 1.44, for no block, FNB, and ACB, respectively. At 5.61 months postoperatively, there was no significant difference across the 3 groups in isokinetic quadriceps deficits (P ≥ .99), and the only significant difference in isokinetic hamstring deficit was observed for peak flexion at 180 deg/s, in which the ACB group had lower peak torque than the FNB group (–9.80% ± 3.48% vs 2.37% ± 3.23%; P = .035). The ratio of participants with a deficit exceeding 15% did not differ significantly among the 3 groups.
Conclusion:
Contrary to previous research, our findings indicate only minimal difference in quadriceps strength among the 3 types of perioperative analgesia in adolescents approximately 6 months after ACL reconstruction. The only significant strength deficit was seen in the hamstrings of patients receiving ACB at peak flexion as compared with those receiving FNB.
In the pediatric and adolescent population, the rate of anterior cruciate ligament (ACL) reconstruction after sport-related injury has increased significantly over the past 10 years. 7 Given the rapid physical development at this age and the high level at which many of these athletes compete, a rapid return to sport is considered an important postsurgical outcome. Femoral nerve block (FNB) and adductor canal block (ACB) are the 2 most frequently used perioperative analgesics to reduce the intake of opioids postoperatively. ¶ While a reduction in postoperative pain and analgesic medication is beneficial, recent studies 1,5,21,22,25 have suggested that perioperative nerve blocks may delay recovery of quadriceps muscle strength, thus delaying return to sport. Determining the effects of these perioperative analgesics on the postoperative quadriceps strength of adolescents will reveal if an analgesic block is most appropriate to optimize recovery after ACL reconstruction and return to sport.
Recent studies 10,22,31 investigating the effect of perioperative FNB during ACL reconstruction have shown an increased deficit in isokinetic quadriceps strength, as compared with no nerve block, during the early postoperative period. However, at 6 months postoperatively, there remains conflicting evidence regarding whether perioperative FNB is associated with a decrease in isokinetic knee extension strength. 21,22,25,31 Differences in surgical techniques, anesthesia protocols, and rehabilitation protocols may have factored into these differing results. Early mobilization has been associated with improved outcomes after ACL reconstruction, which is affected by quadriceps strength and appropriate analgesic control. 18,28,29 Thus, the use of a nerve block that provides adequate analgesia, without significantly affecting quadriceps strength postoperatively, is desired in ACL reconstruction.
ACB has increasingly been used as an alternative to FNB in ACL reconstructive surgery. Although ACB is also an analgesic block of the femoral nerve, it is performed more distally than FNB, in the midthigh. The location of the ACB is thought to allow for greater preservation of motor fibers that innervate the quadriceps muscle, theoretically retaining more muscle strength. 1,11,17,19,24,33 However, the ability of ACB to preserve quadriceps strength postoperatively has been disputed. Two studies 1,10 have reported preservation of quadriceps strength during early postoperative recovery with ACB. Different findings have been noted later in the postoperative period. 2,5,28 Two studies 5,9 have cited greater quadriceps strength deficits with ACB when compared with FNB at 6 to 9 months after surgery. Other studies 2,9,28 have found no difference in quadriceps strength at 6 months postoperatively in patients receiving ACB or FNB. Importantly, these studies did not compare quadriceps strength in patients who received an ACB or FNB with patients who did not receive a peripheral block, and including a control would reveal if analgesia significantly impairs strength as compared with no analgesia.
The aim of this retrospective chart review was to compare 3 perioperative analgesic approaches—FNB, ACB, and no peripheral nerve block (general anesthesia only)—and determine the one providing the best limb symmetry outcomes (quadriceps and hamstring) between the affected and nonaffected limbs at 4 to 8 months after ACL reconstruction in adolescents and young adults. Despite mixed evidence, we hypothesized that there would be a significant deficit in relative postoperative quadriceps strength among patients who had perioperative FNB as compared with those who received ACB or no nerve block. As neither FNB nor ACB should affect the sciatic nerve or its branches, we hypothesized that there would be no difference in postoperative hamstring strength among patients who had perioperative FNB, ACB, and no nerve block. The findings of this study may help with clinical decision-making regarding the use of peripheral nerve block during ACL reconstruction in adolescents and/or provide preliminary data to determine the need for a larger prospective study.
Methods
Chart Selection
To reduce the impact of other factors that might influence postoperative outcomes, all patients underwent surgery by the same orthopaedic surgeon (P.A.M.) at a subspecialized pediatric orthopaedic health center, with data for quadriceps and hamstring strength collected using a standardized isokinetic testing protocol. Specifically, we considered all patients who underwent ACL reconstruction at Shriner’s Hospital for Children–Canada (SHC-Canada) between July 2008 and January 2018. Patients were excluded from the chart review if they had undergone a previous ACL reconstruction on either knee. Inclusion criteria were (1) primary unilateral ACL reconstruction with or without meniscal repair, (2) hamstring tendon graft, and (3) autograft. Exclusion criteria were (1) isokinetic strength testing at <4 or >8 months postoperatively, (2) patellar or iliotibial band graft, (3) allograft, (4) multiligament injuries, and (5) articular cartilage injuries. Ethics approval for this retrospective chart review was received before data collection.
An a priori calculation for minimum sample size was based on a comparison of 3 group means: patients receiving FNB, those with ACB, and those with no peripheral nerve block. The calculation was based on finding a difference of 15% in the isokinetic strength of the quadriceps between the affected and unaffected limbs, with an estimated standard deviation of 15% for each group. We considered a ≤15% strength deficit 6 months postoperatively an acceptable cutoff value for progressive return to sport. A 15% deficit in isokinetic strength has been used previously, 21 which allows for better comparison across the literature.
Using an online sample-size calculator, a minimum sample size of 21 patients per group was determined for 3 pairwise comparisons (3 groups), with an alpha value of 5% and a 1 – β value of 80%. 15
Data Extraction
Electronic medical records were used to collect the characteristic data for each patient, which included age at surgery, sex, body mass index, surgery, graft type, and anesthetic type and dose as well as the isokinetic strength from the operated and nonoperated limbs 4 to 8 months after ACL reconstruction. Isokinetic testing was conducted at 2 centers: Royal Victoria Hospital (RVH) of the McGill University Health Centre from 2008 to 2017 and SHC-Canada between 2017 and 2018. Of the 98 patients included, 42 were tested at SHC-Canada. Data were retrieved from paper charts at RVH, whereas electronic data were available at SHC-Canada. Any other information that was not available in the electronic records was extracted from paper charts at the 2 facilities.
Anesthetic Selection and Dosage
The anesthetic selection and dosage were dependent on the anesthesiologist involved in the procedure. While the patient was being anesthetized for surgery, a predetermined volume of ropivacaine or bupivacaine at concentrations of 0.2% to 0.3%, with or without epinephrine, was administered as regional anesthesia, depending on the preference of the anesthesiologist. The nerve block (FNB or ACB) was administered under ultrasound guidance. Thus, the different analgesic approaches were a reflection of the different anesthesiologists involved in the surgical cases.
Postoperative Rehabilitation
After ACL reconstruction, all patients were required to follow a standardized rehabilitation protocol. The standardized protocol for an ACL repair consisted of progressive range of motion, weightbearing, and closed-chain strengthening as tolerated, starting immediately postoperatively. As quadriceps strength increased, the patient was progressively weaned off crutches and the knee immobilizer brace (Zimmer). After 5 months, straight-line jogging without the brace was allowed. In cases with concurrent meniscal repairs, the protocol was similar with additional restrictions: no knee flexion >90° and no weightbearing on the operated lower extremity for 6 weeks. Approximately 90% of the patients were seen in the physical therapy department at SHC-Canada. The rest of the patients opted for rehabilitation at private clinics.
Isokinetic Strength Testing
Isokinetic strength testing for all patients was performed by a licensed physical therapist at 4 to 8 months postoperatively using either a Biodex System 3 Pro instrumented dynamometer (Biodex Medical Systems; at RVH before 2017) or a Con-Trex MJ Mk2b-15622 isokinetic dynamometer (Physiomed Elektromedizin; at SHC-Canada, 2017-2018).
Patients were requested not to exercise for 48 hours prior to the isokinetic testing. Before the isokinetic testing session, patients were asked to warm up on a stationary bicycle for 5 minutes at moderate intensity (4 or 5/10 on the Borg scale). On the isokinetic dynamometer, patients were then asked to perform 10 repetitions of knee extension (quadriceps) and flexion (hamstring) at 300 deg/s with moderate effort (5/10 on the Borg scale) to familiarize them with the movement. The patients were then asked to perform 3 sets at maximum effort: 5 repetitions at 60 deg/s and 10 repetitions at 180 deg/s. The testing was performed in that order, and adequate rest was provided between the sets for the patient to feel prepared for the subsequent set. Testing always began with the nonaffected leg, followed by the affected leg.
Outcome Measures
The primary outcome measures for this study were the deficits in percentages in peak torque and total work values from the quadriceps and hamstring during isokinetic testing at 60 and 180 deg/s. Peak torque (N·m) was defined as the maximum torque produced during knee extension (quadriceps) or flexion (hamstring) for each velocity of testing over the tested range of motion. Total work (J) for each velocity and direction of movement was the product of the torque and angular displacement over the tested range of motion. 3,16 These parameters provide accurate and highly reproducible measurements and are considered the gold standard in isokinetic testing. 16 The deficit percentage was calculated by dividing the values of the affected limb with those of the nonaffected limb, multiplying by 100, and subtracting from 100.
Statistical Analysis
Descriptive statistics (mean, standard deviations, and ranges) were calculated for patient characteristics (age, sex). Before hypothesis testing, chi-square tests were performed to determine if proportions were equivalent across groups (FNB, ACB, no nerve block) for sex (female/male) and meniscal procedure (yes/no). One-way analysis of variance was used to assess differences among the groups (FNB, ACB, no nerve block) for potential confounding factors (meniscal repair, tourniquet time, surgical time, age at testing, postoperative time of testing), and none were found.
One-way analysis of variance was also used to assess difference among the 3 groups (FNB, ACB, no nerve block) for the deficit of peak torque and total work values from the quadriceps and hamstring during isokinetic testing at 60 and 180 deg/s. Post hoc test using Sidak correction was performed to account for multiple comparisons. Chi-square tests were performed to determine if the proportion of patients with deficits exceeding 15% differed significantly across groups.
All statistical analyses were performed using IBM SPSS Statistics Version 24 (IBM). P < .05 was considered significant.
Results
A total of 292 patients were initially considered for this study, of which 98 were included in the analysis (31 no block, 36 FNB, and 31 ACB). A flowchart illustrating the study inclusion process is shown in Figure 1.

Flowchart of patient inclusion in the study. ACL, anterior cruciate ligament.
Participant characteristics did not differ significantly among the 3 groups regarding time of testing postoperatively, age at surgery and testing, and tourniquet and surgery time (Table 1). The number of patients who underwent meniscal repair was significantly different across the groups, where only 30% of the patients in the ACB group had a meniscal repair (P = .02).
General Characteristics of Patients in the Study Groups: No Block, FNB, and ACB a

a Data are reported as mean ± SD or No. (%). Dash indicates no anesthetic administered to patients in the No Block group. Bold P value indicates statistically significant difference across all 3 groups (P < .05). ACB, adductor canal block; FNB, femoral nerve block.
There was no significant difference in isokinetic quadriceps deficits at 5.61 ± 2 months (mean ± SD; P ≥ .99) postoperatively among adolescent patients receiving FNB, ACB, or no nerve block (Table 2). The difference in isokinetic hamstring deficits was not significant among the 3 experimental groups except for knee flexion peak torque at 180 deg/s, where participants who underwent ACB had lower peak torque than those who received the FNB (ACB, –9.80% ± 3.48%; FNB, 2.37% ± 3.23%; P = .035). Those who did not receive any block did not differ significantly from the other 2 groups (FNB vs no block, P = .802; ACB vs no block, P = .258). For hamstring and quadriceps, there was a trend for the ACB group to show greater deficit percentages (more negative values), indicating weaker muscles in the affected limb as compared with the nonaffected one.
Postoperative Isokinetic Strength Deficit Percentages for Peak Torque and Total Work a
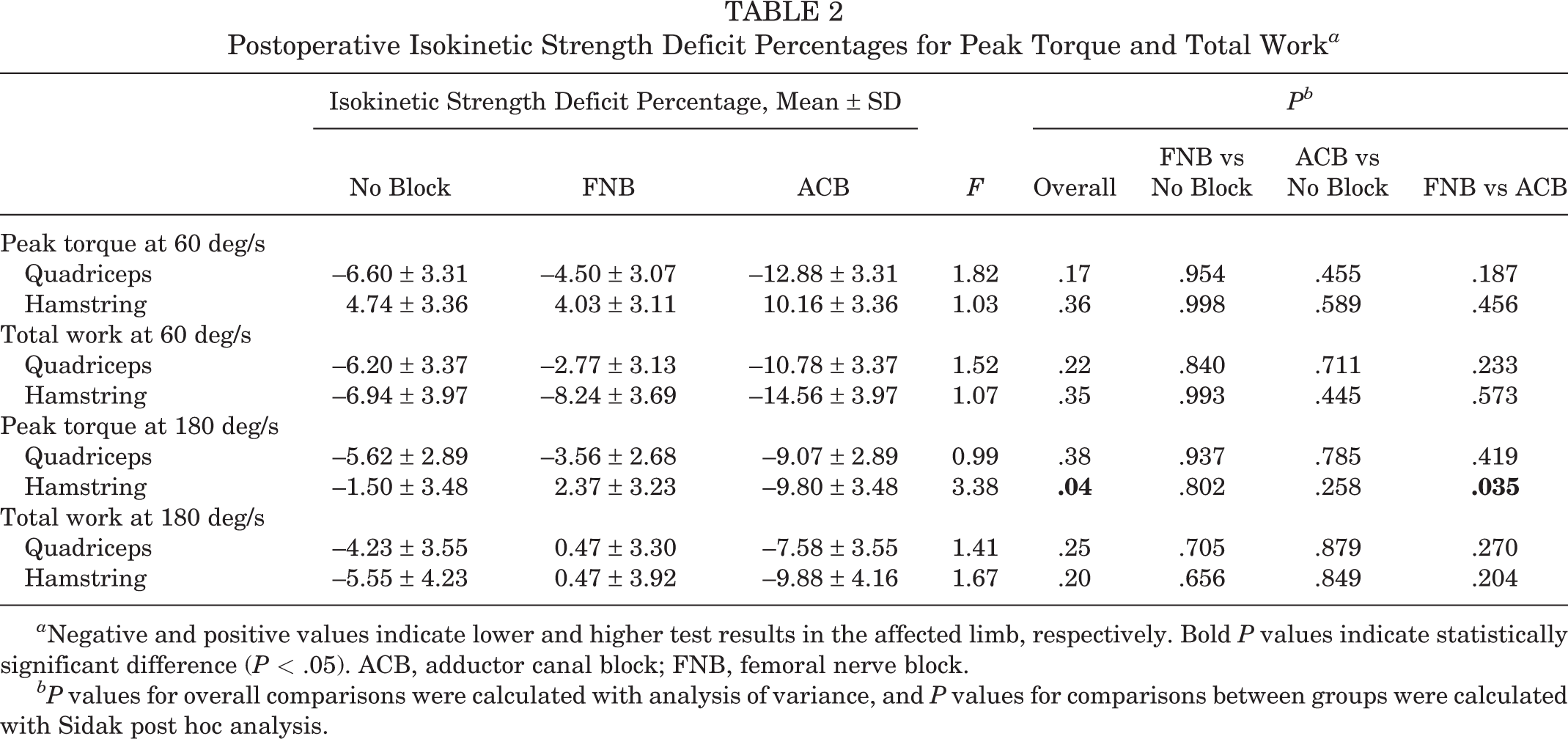
a Negative and positive values indicate lower and higher test results in the affected limb, respectively. Bold P values indicate statistically significant difference (P < .05). ACB, adductor canal block; FNB, femoral nerve block.
bP values for overall comparisons were calculated with analysis of variance, and P values for comparisons between groups were calculated with Sidak post hoc analysis.
The ratio of participants with a deficit >15% for the affected limb are in Table 3, and the ratio ranged between 25% and 50% for quadriceps and hamstring across the 3 groups. None of the groups differed significantly from one another.
Proportion of Participants With Isokinetic Strength Deficit Percentage >15% a

a ACB, adductor canal block; FNB, femoral nerve block.
bdf = 2; N = 98.
Discussion
The objective of this retrospective chart review was to determine if peripheral nerve blocks (FNB and ACB) used perioperatively during ACL reconstruction to provide postoperative analgesia may contribute to quadriceps and hamstring strength deficits in adolescents and young adults relative to those who received no nerve block. Contrary to our initial hypothesis, there was minimal difference among the 3 types of perioperative analgesia (FNB, ACB, or no block) used during the surgical procedure on the quadriceps strength recovery in adolescents after ACL reconstruction. The only significant difference was observed for knee flexion peak torque at 180 deg/s, where participants who underwent ACB had lower peak torque than those who received the FNB, indicating greater hamstring muscular deficits in those receiving ACB as compared with FNB.
The results of this study are not entirely surprising, with recent studies by Bailey et al 2 and Runner et al 28 reporting similar findings. These studies measured the quadriceps strength of patients after FNB and ACB after 6 months, finding similar isokinetic quadriceps strength in both groups. Bailey et al also assessed the quadriceps strength earlier postoperatively, noting significant functional deficits in the patients receiving the FNB after 24 hours and 2 weeks, demonstrating that any functional deficits in muscle strength from the FNB are temporary and self-resolving. The strength of our study was the inclusion of patients who did not receive a nerve block, with our findings suggesting that the nerve blocks do not contribute a significant functional deficit in quadriceps strength several months after ACL reconstruction. In other words, analgesic blocks will not impair recovery after ACL reconstruction versus no block, allowing for sufficient pain relief and appropriate return to sport.
A hamstring deficit at peak torque 180 deg/s in those who received ACB as compared with FNB was an intriguing result. Persistent hamstring deficits 6 months postoperatively is concerning, as this weakness may affect the overall rehabilitation process and increase the risk of ACL reinjury. 27 This is particularly true in female athletes, in which quadriceps dominance is frequently observed and the quadriceps muscles are preferentially recruited over hamstrings, increasing the risk of ACL injury. 26 The weakness observed in the current study reached statistical significance for peak torque at 180 deg/s but not at 60 deg/s. Sport activities are believed to involve high angular velocities, 30 and hamstring deficits approaching sport-level velocities may indicate that the patients are not prepared to return to sport. Furthermore, all surgical procedures in the study were performed with a hamstring graft; therefore, if the weakness was graft harvest related, it should have been present in all groups. Given that hamstring function is dictated by sciatic innervation, the hamstring weakness cannot be directly attributed to the blockage of femoral nerve distribution. However, it is possible that local diffusion of the ACB into the posterior compartment occurs, and this may contribute to the hamstring weakness through a local toxic effect. Myotoxicity, as a result of peripheral nerve blocks, may impair functional recovery for up to 1 year, and ACB is known to be associated with this risk as compared with other nerve blocks. 14 Overall, the reasons for which hamstring deficits were increased at peak torque of 180 deg/s in patients who received ACB versus FNB largely remain unclear and warrant follow-up investigation to determine if this finding is robust and repeatable in other patient groups. This effect has not been reported and may have important clinical ramifications.
Our study did not measure quadriceps strength within the first 4 months postoperatively. However, the FNB has been shown to lead to more significant quadriceps strength deficits in the short term as compared with ACB, while providing similar analgesic effects. 1,2 The FNB likely blocks many of the motor fibers innervating the quadriceps, normally preserved in an ACB, leading to an initial strength deficit in the early postoperative period. Over time, as suggested by Runner et al, 28 the blockade of the motor fibers likely resolves such that no significant difference in quadriceps strength exists after 6 months and any muscle weakness that exists 6 months postoperatively is suggestive of lingering pain from the procedure itself rather than any specific nerve block used perioperatively. Proper rehabilitation of the ACL-reconstructed knee is essential in restoring overall muscular balance and strength. 23 It is possible that patient adherence to rehabilitation and his or her ability to recover from surgery may have affected muscle strength. Additionally, despite the use of a standardized protocol, postoperative rehabilitation may have varied if patients received therapy via the hospital or from a private clinic, with differing physical therapists.
Other studies 5,21 have shown long-term postoperative quadriceps weakness after perioperative analgesia. This difference from the findings of the current study may be due to multiple variables, including patient age, graft type, testing site, and the operating surgeon. The patient population in our study consisted entirely of adolescents, on average 15 years of age, while Christensen et al 5 studied a young adult population. Patients of a younger age were shown to have a better quadriceps strength recovery 6 months after ACL reconstruction. 32 The young age of our patients in this study may also explain the lack of significant differences among the studied groups. Furthermore, the 2 aforementioned studies used a mix of patellar tendon and hamstring grafts. Graft choice has been demonstrated to affect knee extension and flexion symmetry 6 months after ACL reconstruction, 20 and this effect was avoided in our study, with patients receiving only a hamstring autograft. In addition, the patients were tested at 2 sites, a pediatric hospital and an adult hospital, where the instrumented dynamometer and physical therapists varied. However, the use of a within-participant design for this study minimized the degree of this effect. In addition, all the participants in this study underwent surgery by the same surgeon, which ensured greater uniformity in postoperative recovery independent of the perioperative analgesic procedure. Nonetheless, more studies are required to determine the actual mechanism and factors that contribute to quadriceps muscle recovery in the long term.
Our study was constrained by various limitations. We used a retrospective methodology, where the patients were selected according to previously defined inclusion criteria rather than randomized to receive the intervention. Despite not having randomized the sample, there was relative homogeneity in the categories of age, sex, and tourniquet time among groups. Therefore, it is unlikely that the findings were significantly affected by the lack of randomization. Furthermore, the sample size in the current study was quite small, with a total of 98 patients (31 each receiving no block or ACB and 36 receiving FNB), which may have introduced a type II error. This small number was due in part to the exclusion of 162 patients with missing isokinetic data. Each group, however, met the required sample size to support the comparisons performed. Of this small number, patients receiving a meniscal repair were not excluded to meet an adequate sample size number. The number receiving a meniscal repair differed significantly among groups. However, the patients receiving ACB had greater isokinetic deficits than those receiving no block and FNB, despite less frequent meniscal repair and thus earlier weightbearing.
This study was limited to hamstring autografts, so the results cannot be generalized to other graft types. In addition, the pain secondary to hamstring harvest was unlikely to be diminished by the use of either block group, FNB or ACB, which may have ultimately affected the adequacy of the analgesia. In addition, despite having the same surgeon perform the ACL reconstruction, the anesthesiologists and anesthesia administration varied among patients, further influencing the efficacy of the analgesic. Last, despite a standardized rehabilitation protocol, the exact postoperative treatment received by each patient may have been affected by the individual approach of each physical therapist as well as the motivation of the patient.
Conclusion
Since quadriceps deficits increase the risk of ACL reinjury, 13 they can delay the progressive return to modified sport activities, highlighting the importance of quadriceps muscle strength postoperatively. Our study showed no significant difference in isokinetic quadriceps function at approximately 6 months postoperatively among adolescent patients receiving FNB, ACB, or no nerve block after ACL reconstruction. The only significant strength deficit was seen for knee flexion peak torque in the hamstrings of patients receiving ACB as compared with FNB, which represents a novel and concerning finding. Altogether, the findings of this study suggest that the choice of FNB, ACB, or no nerve block for ACL reconstruction analgesia should not be constrained by concerns about quadriceps muscle strength for adolescent patients who received a hamstring autograft. The factors that influence quadriceps recovery postoperatively need to be studied to further improve athletic rehabilitation and return to sport. The prolonged significant deficit on 1 of 4 measures of hamstring strength for patients in the ACB group warrants further investigation.
Footnotes
Acknowledgment
The authors thank the Department of Rehabilitation of the Royal Victoria Hospital in Montreal for supporting the data-collection process and Dr Reggie Hamdy, medical director of the Shriners Motion Analysis Center, for supporting the current work.
Final revision submitted December 14, 2020; accepted February 9, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from McGill University Health Centre.