
Abstract
Background:
The current coronavirus 2019 (COVID-19) pandemic has prompted a multitude of public health response measures including social distancing, school cancellations, and cessation of organized sports.
Purpose:
To examine the impact of COVID-19 and corresponding public health measures on the characteristics of common pediatric musculoskeletal injuries associated with sports.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a multicenter retrospective cohort study comparing patients with sports injuries presenting to 3 geographically diverse level I pediatric trauma hospitals and outpatient orthopaedic surgery clinics in the United States during the COVID-19 pandemic and a prepandemic period at the same institutions. Patients were included if they presented for care between February 15 and July 15 in 2020 (pandemic cohort) or between March 15 and April 15 in 2018 and 2019 (prepandemic cohort).
Results:
Included were 1455 patients with an average age of 12.1 ± 4.5 years. When comparing patients presenting in 2018 and 2019 with those presenting in 2020, we observed a decrease in mean age during the pandemic (12.6 ± 4.0 vs 11.0 ± 5.2 years; P = .048). Additionally, a decrease in the proportion of injuries attributed to sports (48.8% vs 33.3%; P < .001) and those occurring at school (11.9% vs 4.0%; P = .001) was observed. The proportion of injuries attributable to clavicle fractures increased during the early stages of the pandemic (13.2% vs 34.7%; P < .001). There was no statistically significant delay to care in injuries presenting during the pandemic (41.5 ± 141.2 vs 19.23 ± 79.1 days; P = .175).
Conclusion:
Across 3 tertiary care institutions, patients were seen without significant delay during the pandemic. We observed a significant decline in pediatric musculoskeletal injuries associated with sports during the COVID-19 pandemic. This decrease has been accompanied by a shift in both injury type and mechanism.
Keywords
The novel coronavirus 2019 (COVID-19) was first reported in December 2019 as a cluster outbreak in Wuhan, China, 31 and it has since spread around the world, reaching pandemic status in March 2020. 29 Policies put in place in China, including quarantine, social distancing, and public closures, were demonstrated to slow the spread of COVID-19, leading to implementation in countries around the world including the United States. 1 This has included school closures, stay-at-home orders, and the closing of businesses in an effort to reduce strain on the health care system.
In addition to slowing the spread of the viral outbreak, these practices were expected to alter the epidemiology of patients reporting to both emergency rooms and clinics across the health care system. For children, the cancellation of school, afterschool activities, and organized sports would likely mean a decrease in musculoskeletal injuries, particularly those related to sports involvement. This decrease could be especially prevalent given the typical increase in pediatric injury presentation in the spring and fall seasons when sport activities are most common. 11,21
Significant delays to care and decreased patient volume have been observed in a variety of medical subspecialties, including orthopaedic surgery, 4,10 as a result of the COVID-19 pandemic. 16,17,24 This may suggest reluctance for patients to seek medical care because of concerns for increased COVID-19 exposure. 5 Combined with cessation of organized and school-related sports, this raises the likelihood for both decreased occurrence and presentation of musculoskeletal injuries.
The objective of this study was to examine the effect of COVID-19 and corresponding public health measures on the incidence and distribution of common pediatric musculoskeletal injuries associated with sports. Our hypothesis was that sports injury presentation would decrease and that there would be a shift in the characteristics of patients presenting for care during the pandemic. We also hypothesized that a delay to care after injury would be observed.
Methods
Included in this institutional review board–approved retrospective cohort study were patients who were evaluated with common musculoskeletal injuries at 1 of 3 hospital systems during the COVID-19 pandemic. These patients were compared with a cohort with similar injuries at the same institutions during a prepandemic timeframe. The pandemic cohort consisted of patients arriving for initial care between March 15 and April 15, 2020. The prepandemic cohort consisted of patients arriving between March 15 and April 15 in 2018 and 2019. Additionally, comparisons were made between the early pandemic (March 15 to May 15, 2020) and midpandemic (May 16 to July 15, 2020) time periods.
The hospital systems in this study were geographically diverse (Northeast, Southwest, and West) level I pediatric trauma hospitals or associated pediatric orthopaedic surgery outpatient clinic sites, and patients were evaluated for 1 of the following acute injuries: anterior cruciate ligament injury, meniscal injury, patellar dislocation, osteochondritis dissecans (OCD), shoulder dislocation, ankle ligament sprain, clavicle fracture, medial epicondyle fracture, and tibial spine fracture. Data collection was performed based on review of emergency department and outpatient clinic records for first-time presentations of these injury types. Follow-up visits were excluded. Descriptive data including age at time of injury, sex, race, and insurance status were recorded. Insurance status as listed in the electronic medical record was classified as no insurance, public insurance (Medicaid), or private insurance. Location of injury was classified as home, public, school (including day care), organized sports, playground, or not reported. The mechanism of injury was classified as sports, low-energy fall, high-energy fall, direct blow, or not reported. A high-energy fall was classified as a fall with more energy than body weight including falling downstairs, falling from monkey bars, and trampoline falls. If patients were injured with a sports-related mechanism, then the specific sport was reported. The laterality of the injury (right vs left vs bilateral) was also reported.
To understand care pathways, both the location of the visit (emergency department vs outpatient clinic vs virtual outpatient clinic) and the previous site of treatment were documented. The delay to care was calculated as the number of days between the date of injury and first clinic or emergency department visit.
Variables were compared between the prepandemic and pandemic cohorts and the early pandemic and midpandemic cohorts. Categorical variables were compared utilizing chi-square and Fisher exact tests, while continuous variables were compared using Mann-Whitney U tests. In all cases, statistical significance was identified with a threshold of P < .05. All statistical analyses were performed using SPSS Statistics for Macintosh Version 24.0 (IBM Corp).
Results
A total of 1455 patients with a mean ± SD age of 12.1 ± 4.5 years were included (Figure 1). The most common presenting injury was ankle sprains (n = 696; 47.8%), and the least common was tibial spine fractures (n = 21; 1.4%). The number of patients seen between March and April, April and May, May and June, and June and July during the pandemic was 75, 76, 145, and 174, respectively.

Flow diagram of patient inclusion. Prepandemic group was defined as all patients presenting between March 15 and April 15, 2018; March 15 and April 15, 2019; and February 15 and March 14, 2020. The pandemic cohort was defined as all patients presenting between March 15 and July 15, 2020.
A total of 75 patients presented during the first month of the 2020 pandemic, compared with a mean of 337 patients between March and April in 2018 and 2019. The proportion of injuries occurring in male patients increased during the early stages of the pandemic from prepandemic (60.0% [45/75] vs 46.4% [313/674]; P = .026). There were no differences in race (P = .971) or insurance status (P = .240) between cohorts. The mean ± SD presenting age during the pandemic was lower than that prepandemic (11.0 ± 5.2 vs 12.6 ± 4.0 years; P = .048) due to a decrease in the proportion of injured patients aged >12 years (50.7% [38/75] vs 61.6% [415/674]; P < .001) and a corresponding increase in children aged <6 years (24.0% [18/75] vs 7.7% [52/674]; P < .001) (Figure 2). The location of injury was found to differ between cohorts, with a higher proportion of injuries occurring at home during the pandemic than prepandemic (30.7% [23/75] vs 17.2% [116/674]; P = .001). A lower proportion of injuries occurred as a result of playing sports during the pandemic than prepandemic (33.3% [25/75] vs 48.8% [329/674]; P < .001). The most common sport leading to injury in both the pandemic and the prepandemic cohorts was basketball, with an increase in the proportion of basketball-related injuries observed during the pandemic (48.0% [12/25] vs 25.2% [83/329]; P = .023) (Table 1).
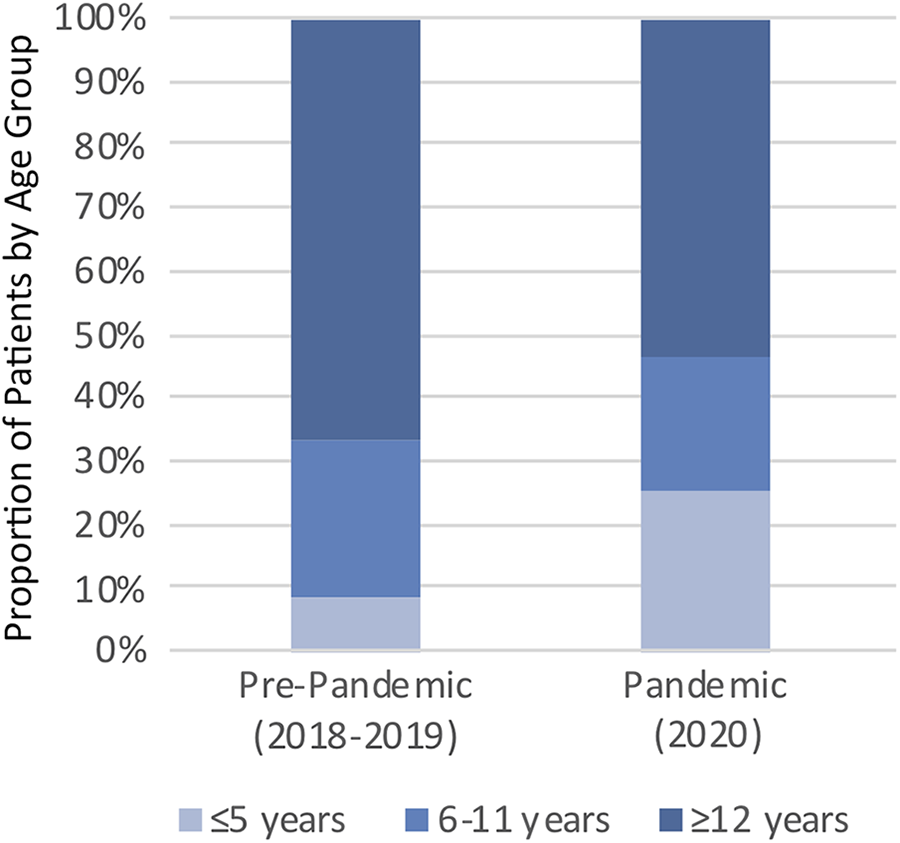
Proportion of injuries by age group in patients prepandemic versus those during the first month of the COVID-19 pandemic.
Characteristics of Prepandemic Group Versus Group During the First Month of the Pandemic a

a Data are reported as n (%) or mean ± SD. Values in bold indicate a statistically significant difference between groups (P < .05).
There was a higher proportion of clavicle fractures (34.7% [26/75] vs 13.2% [89/674]; P < .001) and a lower proportion of ankle sprains (32.0% [24/75] vs 58.9% [397/674]; P < .001) in the pandemic versus prepandemic cohort. Patients in the pandemic cohort were more likely to be seen virtually (4.0% [3/75] vs 0; P < .001). There was no overall increase in time to presentation during the pandemic (P = .175) (Table 2).
Injury Characteristics and Management of Prepandemic Group Versus Group During the First Month of the Pandemic a

a Data are reported as n (%) or mean ± SD. Values in bold indicate a statistically significant difference between groups (P < .05). ACL, anterior cruciate ligament; ED, emergency department; OCD, osteochondritis dissecans; OSH, outside hospital.
When comparing injuries from early pandemic (March 15 to May 15) to midpandemic (May 16 – July 15), the number of patients presenting increased >2 times (Figure 3). Accompanying this increase, the proportion of children aged <6 years presenting for care decreased (17.2% [55/319] vs 24.5% [37/151]; P = .002) and the proportion of children aged >12 years increased (59.2% [189/319] vs 50.3% [76/151]; P = .002) from early to midpandemic (Table 3). Additionally, patients seen later during the pandemic were more likely to be seen in an outpatient clinic setting compared with those seen in the first 2 months of the pandemic (61.8% [197/319] vs 50.3% [76/151]; P = .016) (Table 4).

Comparison of sports injury presentations by month during the COVID-19 pandemic between February and July of 2020 and March and April of 2018 and 2019.
Characteristics of Early Pandemic and Midpandemic Groups a

a Data are reported as n (%) or mean ± SD. Value in bold indicates a statistically significant difference between groups (P < .05).
Injury Characteristics and Management of Early Pandemic and Midpandemic Groups a

a Values reported as n (%) or mean ± SD. Values in bold indicate a statistically significant difference between groups (P < .05). ACL, anterior cruciate ligament; ED, emergency department; OCD, osteochondritis dissecans; OSH, outside hospital.
Discussion
The COVID-19 pandemic has had a profound effect on all aspects of daily life for children, with the closing of schools, cancellation of organized sports, and a greater amount of time spent at home. This study examined trends of injury presentation in 3 large geographically diverse pediatric hospitals as a result of the COVID-19 pandemic and demonstrated a drastic reduction in overall volume and a decreased mean patient age. Additionally, the distribution of injury types was affected with clavicle fractures making up a larger proportion of presenting injuries during the pandemic. This is the first reported study assessing the effect of the COVID-19 pandemic and public health policies on pediatric sports injuries. Understanding the changing epidemiology of pediatric injuries presents an opportunity for basic safety precautions to improve public health.
Before the COVID-19 pandemic, the majority of the injuries evaluated in this study had been shown to be increasing in frequency, most likely attributable to increased involvement in competitive sports. 2,3,14,20,28 However, in our analysis, we observed a 4-fold reduction in injury presentation compared with the previous 2 years. In the typical prepandemic year, >48% of the 9 injury types discussed here were the direct result of sports. However, during the early stages of the COVID-19 pandemic, this proportion decreased to 33% of injuries. The bulk of this reduction was a result of decreased organized sports, thus preferentially affecting older-aged children. Sports that continued to cause injuries to children during the pandemic were basketball and soccer, which are easily played at home or in outside organized groups. Furthermore, we observed a 13.5% increase in the proportion of injuries occurring in or around the home, with the majority resulting from high- or low-energy falls. This represents a vulnerable group of patients being injured during the pandemic. Several organizations have released statements that include mention of fall risk for pediatric populations; 9,30 however, continued education by medical providers on how parents can best protect children from falls and other injuries at home remains important. 7,13
Significant delays to care as a result of the COVID-19 pandemic have been demonstrated in a variety of other specialties. 12,16,17,24,26 However, Bram et al 4 showed no delay to treatment for pediatric fractures during the first month of the COVID-19 pandemic. We report similar findings for musculoskeletal sports injuries, with no delays to care demonstrated. This could indicate adequate clinical capacity for orthopaedic care for acute musculoskeletal injuries in our 3 respective geographic regions. However, for conditions such as shoulder dislocations, patellar dislocations, and OCD, which may represent acute presentations of chronic injuries, we saw very few patients presenting for care during the pandemic. Delays to care have been shown to lead to poor functional outcomes and poor joint health for pediatric patients in a variety of injury types. 15,18,22,23 Additionally, if not properly evaluated, sports injuries can lead to prolonged return to sports times, which have been shown to negatively affect pediatric development and athletic lifestyle. 8,19,27 While we did not observe delays, it is important to continue monitoring for signs of delayed presentation, especially regarding acute-on-chronic conditions, as the COVID-19 pandemic continues to develop.
While the COVID-19 pandemic has resulted in a significant decline in sports injuries, there are likely other negative health effects as a result of decreased involvement in organized sports. These include the risk for decreased conditioning and obesity in children as well as mental health decline. Furthermore, it will be important to monitor the risk of pediatric musculoskeletal injuries as organized sports resume. Given the potentially long period of inactivity and deconditioning, this poses an increased risk for pediatric athletes.
Despite the use of a multicenter study design to evaluate injuries presenting to 3 large geographically diverse pediatric orthopaedic practices, several limitations should be noted including the overrepresentation of certain injury types including ankle sprains and clavicle fractures. Additionally, while we evaluated the total presentations of the 9 key injuries, we cannot definitively differentiate if patients are being injured at a lower rate because of sports and school cancellations or if there is a failure to present. Another potential explanation for the decrease in volume demonstrated is that local orthopaedists or nonpediatric trained orthopaedic sports surgeons may be more likely to treat pediatric patients during the COVID-19 pandemic. Changes in referral patterns are difficult to assess in the rapidly changing landscape of the COVID-19 pandemic with different injury types having different pathways to orthopaedic care. Additionally, our study does not accurately reflect the rate of virtual clinic visits at our institutions’ orthopaedic surgery departments, with visits only representing acute first-time presentations of injuries, rather than follow-up visits, which are more adaptable for telemedicine. 25
Conclusion
In this multicenter study monitoring pediatric injury presentations, we observed a profound effect of the COVID-19 pandemic on pediatric musculoskeletal injury presentation across the United States. The overall volume has decreased, sports injuries have decreased, and the proportion of injuries occurring in the home have increased. With >9.2 million cases of COVID-19 reported and >230,000 deaths as of November 1, 2020, 6 social distancing and working from home initiatives are likely to remain in effect moving forward. The information presented here highlights the changing epidemiology of musculoskeletal injuries in pediatric patients and represents an important opportunity for basic safety precautions for injury prevention at home.
Footnotes
Final revision submitted March 4, 2021; accepted March 24, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: H.B.E. has received consulting fees from Smith & Nephew, education payments from Arthrex and Pylant Medical, and speaking fees from Smith & Nephew and Synthes. K.G.S. has received education payments from Evolution Surgical and hospitality payments from Arthrex. T.J.G. has received research support from Vericel, Arthrex, and AlloSource and education payments from Liberty Surgical and is a paid associate editor for The American Journal of Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Children’s Hospital of Philadelphia Research Institute (IRB 15-012614).