
Abstract
Background:
Traumatic anterior shoulder instability in collision sports athletes often involves osseous glenoid lesions, which make surgical treatment challenging. High redislocation rates have been seen in collision sports athletes treated using arthroscopic Bankart repair.
Purpose:
To investigate the effectiveness of a combined arthroscopic Bankart repair and open Bristow procedure for the treatment of traumatic anterior shoulder instability in collision sports athletes, with a focus on osseous glenoid lesions.
Study Design:
Case series; Level of evidence, 4.
Methods:
We reviewed 149 shoulders in 141 competitive collision sports athletes (mean ± standard deviation age, 20.1 ± 4.1 years; 8 bilateral cases) who underwent a combined arthroscopic Bankart repair and open Bristow procedure with minimum 2 years of follow-up. Osseous Bankart lesions were arthroscopically reduced and fixed using a coracoid graft.
Results:
Clinical outcomes as indicated by mean Rowe score improved significantly from 50.0 preoperatively to 98.9 postoperatively (P < .001) at a median follow-up of 3.4 years (range, 2.5-7 years). There were 2 recurrent dislocations (1.3%), both of which had nonunion of the transferred coracoid. Osseous Bankart lesions were observed in 85 shoulders, and osseous glenoid lesions ≥10% of the diameter of the nonoperative side were found in 58 shoulders, including 24 off-track cases. Clinical outcomes were not significantly different between patients with a glenoid defect ≥10% and <10%. Nonunion of the transferred coracoid was observed in 16 shoulders (10.7%), which had inferior Rowe scores; however, we could not define any risk factors for nonunion, including patient characteristics or bone morphology. Postoperative computed tomography performed in 29 patients >1 year after surgery showed successful repair of the osseous glenoid lesions, with a restored glenoid articular surface in all cases. Significant pre- to postoperative increases were seen in glenoid diameter (mean, 13.1% [95% CI, 9.9%-16.3%]; P < .001) and area (mean, 10.6% [95% CI, 8.5%-12.7%]; P < .001).
Conclusion:
A combined arthroscopic Bankart repair and open Bristow procedure improved bone morphology and was a reliable surgical method for treating collision sports athletes with traumatic anterior shoulder instability involving osseous glenoid lesions.
Traumatic anterior shoulder instability is a common injury in collision sports (eg, rugby and American football) and has a great effect on the performances and careers of athletes. 3,4 It often involves osseous lesions, such as osseous Bankart lesion (OBL) of the glenoid, particularly at the anteroinferior glenoid surface, which indicates osseous glenoid defects. 11,27 Osseous injuries of the glenoid may compromise the glenoid articular surface and result in osseous defects (glenoid defects). 20 Glenoid defects impair normal kinetics, and untreated osseous lesions may contribute to an increased recurrence rate. 5,7,8 Notably, if the size of the Hill-Sachs lesion and glenoid defect causes an “off-track” lesion, reconstruction of bone morphology is usually recommended. 30
Regarding surgical treatment, even if there is no glenoid defect in the case of traumatic anterior instability of the shoulder, bony erosion and postoperative rim fracture of the glenoid have been reported at the suture anchor insertion sites used in arthroscopic Bankart repair. 9,17 Arthroscopic Bankart repair alone may not be sufficient to offer reliable stability in collision sports athletes, 6,16 and the coracoid transfer procedure (Bristow and Latarjet procedures) has been shown to be beneficial in the treatment of these patients. 26,29 However, after the coracoid transfer procedure, recurrent anterior instability can develop because of residual soft tissue impairment. 15 A biomechanical study indicated that the stabilizing mechanism of the coracoid transfer is associated with an extra-articular sling effect, which is different from the stabilizing mechanisms provided by Bankart repair. 29 Notably, Tasaki et al 28 reported that a combination of an arthroscopic Bankart repair with a Bristow procedure enabled both arthroscopic Bankart repair and coracoid transfer to the anterior glenoid rim. However, whether the glenoid defect, OBL, and off-track lesion affect the surgical outcomes of this procedure has not been verified. It also remains unclear whether this complex procedure induces surgical variabilities, such as the location of coracoid placement and the screw angle and length, which may be related to complications, especially in patients with glenoid osseous lesions.
The aim of this study was to investigate the effectiveness of a combined arthroscopic Bankart repair and open Bristow procedure in the treatment of traumatic anterior shoulder instability in collision sports athletes, with a focus on osseous glenoid lesions. We hypothesized that this surgical method would show good clinical results and improve restoration of the glenoid articular surface.
Methods
Patient Cohort
This study was carried out in concordance with the Declaration of Helsinki, and ethical approval was obtained from an institutional review board. We reviewed medical records of all the patients who underwent a combined arthroscopic Bankart repair and open Bristow procedure for traumatic anterior shoulder instability at our institution between April 2008 and December 2017. The decision to perform this operation was based on 2 criteria: patients were competitive collision sports athletes who (1) wanted to continue actively participating in sports and (2) were willing to undergo this combined procedure. This procedure was adopted regardless of the presence or size of bone lesions. Those who had >2 years of follow-up and sufficient medical information were included in this study. Patients were excluded if they were athletes who could not continue sports activity for nonmedical reasons (eg, graduation and moving) or had insufficient medical information. All operations and evaluations were performed at a single institution by a single surgeon (A.T.). A chart review was performed retrospectively, and a telephone survey was conducted as required. The study detail were throughly explained to the perticipants, each of whom provided consent to perticipate.
Surgical Technique
The details of the combined arthroscopic Bankart repair and open Bristow procedure have been described elsewhere. 28 In brief, the patient was placed in the beach-chair position, and a deltopectoral approach was used to dissect the coracoid process approximately 15 mm from its tip using a sagittal saw (HALL MICRO 100; ComMed Linvatec) and curved osteotome. The anterior surface of the glenoid was exposed by separating the subscapularis in the direction of its fibers (Figure 1A). The shoulder capsule, including the inferior glenohumeral ligament, was left intact. A 4.0-mm half-threaded cannulated cancellous screw with a 2.7-mm cannulated drill (Meira) was inserted into the resected coracoid fragment. The length of the screw was the sum of the glenoid diameter measured on computed tomography (CT) images and the length of the coracoid fragment. Glenohumeral ligaments (joint capsule) were identified and preserved. The incised skin was closed to avoid fluid leakage during the following arthroscopic procedure.

Exposure of the anterior glenoid surface and the right shoulder. (A) Before the arthroscopic procedure, the anterior glenoid surface was covered by the anterior glenohumeral ligament (surrounded by circle). (B) After the arthroscopic procedure, the bony surface was exposed (surrounded by dashed circle) because the soft tissue and osseous Bankart lesion were repaired on the rim of glenoid using suture anchors so the lateral end of anterior glenoid surface could be recognized.
Next, an arthroscopic Bankart repair was performed using 3 portals (anterior, posterior, and anterosuperior). The anteroinferior glenohumeral ligament was mobilized, retensioned, and repaired using 4 absorbable suture anchors (Panalok Loops; DePuy Mitek) that were evenly placed from the 5:30- to 2-o’clock position on the right shoulder. OBLs were reduced and fixed to the glenoid by repairing the middle and inferior glenohumeral ligaments using the same suture anchors. 12 The Bristow procedure was then performed after the temporal skin sutures had been removed. When the anterior surface of the glenoid was exposed, the repaired soft tissue and OBL were repaired on the rim of the glenoid using suture anchors so the lateral end of the anterior glenoid surface could be recognized (Figure 1). The ideal position for the transferred coracoid fragment was the 4-o’clock position from the anterior surface of the glenoid in the right shoulder, as close to the joint surface as possible without protruding. If the repaired OBL was large, the coracoid fragment was fixed onto the repaired OBL and compressed using a washer and screw. Finally, the glenohumeral joint was arthroscopically inspected, and the location of the coracoid was confirmed on plain anteroposterior and axial radiographs.
Postoperatively, the shoulder was immobilized in a neutral position using a shoulder brace for 3 weeks, after which time patients began range of motion exercises. Plain radiographs were obtained every 4 weeks until bone union of the transferred coracoid was radiographically confirmed. Running at 10 weeks, passing the ball and weight training at 12 weeks, and physical contact training at 16 weeks postoperatively were allowed.
Data Collection
Pre- and postoperative outcomes were assessed using the Rowe score. 24 Range of motion on the operative and nonoperative sides was measured using a goniometer before and 1 year after surgery. For patients who underwent bilateral surgery, measurements of the nonoperative side at the initial surgery were used as the reference values.
The presence of an osseous glenoid defect was defined using morphologic evaluation and 3-dimensional CT scans showing a difference in glenoid articular surface >3% as compared with the nonoperative side, regardless of the presence of OBLs. 27 Shoulders with a glenoid defect ≥10% of the nonoperative side were considered to be at risk of instability recurrence. 19 Data were analyzed using a picture achieving and communication system with a high-resolution monitor (Coronius Fusion 6MP LED; Barco). The circle approximation method was used for patients without contralateral imaging or with bilateral surgery. 27 An abnormal decompression on the posterolateral surface of the humeral head was recognized as a Hill-Sachs lesion, and its width was measured using 3-dimensional CT images similarly. On-track/off-track status was also assessed. 10 Associated intra-articular lesions found arthroscopically, such as superior labrum anterior and posterior (SLAP) lesions, capsular tears, and humeral avulsions of the glenoid ligament, were noted.
Postoperative CT images were taken on the first day after surgery in all patients, and the length of the transferred coracoid was measured from its tip to the glenoid neck. The position of the transferred coracoid in relation to the glenoid articular surface was assessed on axial views as lateral to the articular surface: sticking out, ≥0 to <2 mm medial to the articular surface, ≥2 to <5 mm, ≥5 to <10 mm, or ≥10 mm. The ideal positions were defined as ≥0 to <2 mm and ≥2 to <5 mm. 28 In addition, the inclination angle of the screw with respect to the joint surface, its depth (whether it reached the contralateral bone cortex), and its location on the sagittal view using clock positions were measured. 2 Union of the transferred coracoid and osteoarthritic changes were evaluated on plain radiographs 1 year postoperatively. 25
We compared the clinical results of patients and surgical variables of this combined procedure between shoulders with a preoperative glenoid defect <10% and ≥10% (a postoperative risk factor for recurrence of instability 19 ). In addition, because coracoid nonunion is considered a possible complication, we investigated which factors were related to the nonunion (patient background, preoperative osseous morphology, or surgical variabilities). In 29 shoulders with OBL and CT imaging >1 year postoperatively, changes of the glenoid articular surface were assessed by measuring its diameter and area on the sagittal view (Figure 2). Complications and related factors were also reviewed.
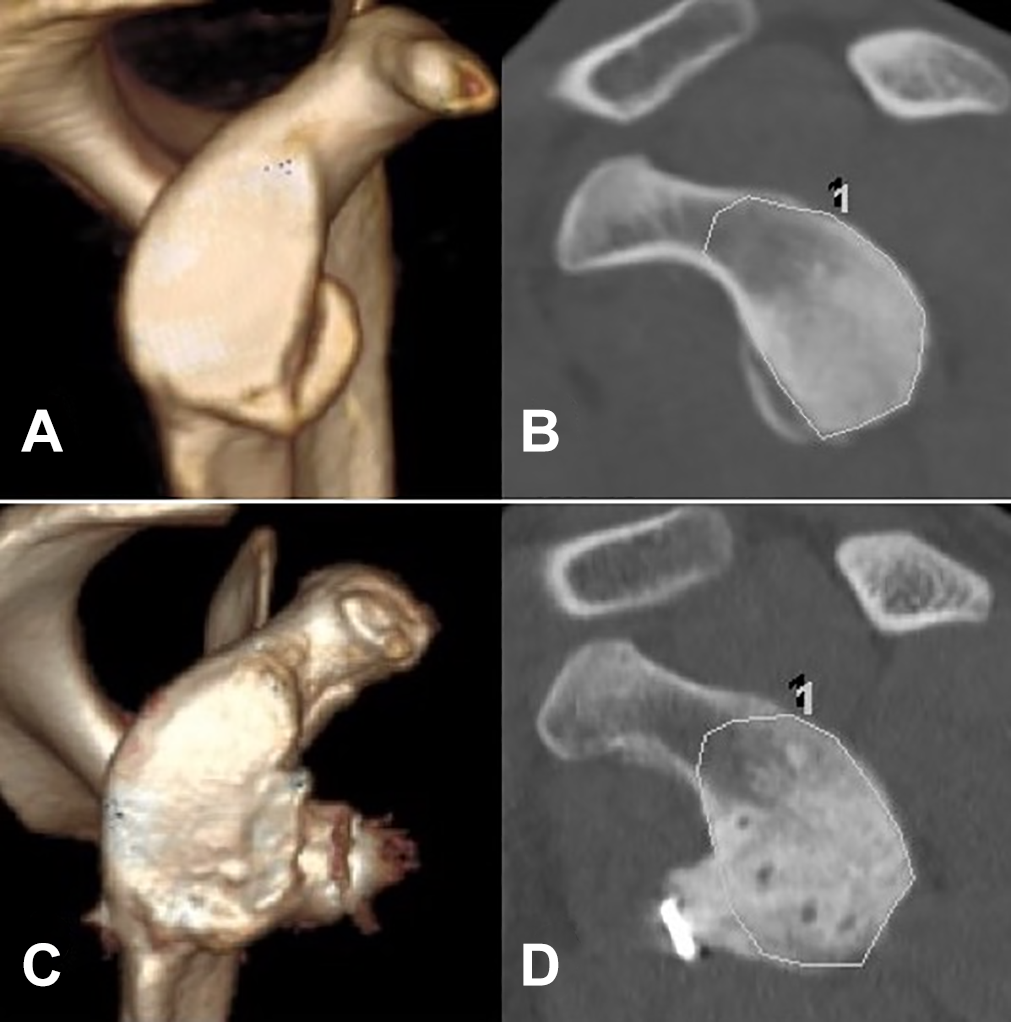
Computed tomography images of a patient with a glenoid bony lesion of the right shoulder. (A) Three-dimensional sagittal image before surgery. (B) The area of the glenoid articular surface was preoperatively measured on a raw sagittal view using the picture achieving and communication system. The area surrounded by the line was measured. (C) Three-dimensional sagittal view 2 years postoperatively. (D) The area of the restored glenoid articular surface was measured 2 years postoperatively on a raw sagittal view using the picture achieving and communication system for available cases. The “1” on (B) and (D) appeard on the measurement softwere at the time of measurement and had no meaning.
Statistical Analysis
Statistical analyses were performed using SPSS Version 25.0 (IBM Corp). Categorical data are presented as counts and percentages. Continuous data are described as means and standard deviations except for follow-up period and Rowe scores (presented as mean, interquartile range, and range because the data were not always normally distributed with a low ceiling). Differences in the presence of an osseous glenoid defect and union of the transferred coracoid were compared using the chi-square test, Fisher exact test, Welch t test, or Mann-Whitney U test. Postoperative changes of the glenoid articular surface were assessed using the paired t test. The significance level was set at P < .05.
Results
Patient Characteristics
There were 160 surgical cases during the study period. Eleven patients were excluded: 8 who preferred isolated arthroscopic Bankart repair using different postoperative treatments, 2 who did not play collision sports for 2 years because of graduation or employment, and 1 who was lost to follow-up because of studying abroad. Ultimately, 149 shoulders (cases) in 141 patients with a mean age of 20.1 years met the criteria (Table 1); 21 shoulders (14%) had revision procedures after failed arthroscopic Bankart repair. Overall, 122 cases were from rugby, 18 from American football, 6 from martial arts, 2 from ice hockey, and 1 from lacrosse. Athletes competed at 4 levels: international (n = 13 cases), domestic professional (n = 4 cases), collegiate (n = 120 cases), and high school (n = 12 cases). The median follow-up period was 3.4 years. The preoperative Rowe scores and findings on CT images and arthroscopy are shown in Table 1.
Patient Characteristics and Preoperative Findings a

a Data are reported as mean ± SD (range) or No. (%) of shoulders unless otherwise indicated. ABR, arthroscopic Bankart repair; BMI, body mass index; CT, computed tomography; HAGL, humeral avulsion of glenohumeral ligament; HSL, Hill-Sachs lesion; IQR, interquartile range; OBL, osseous Bankart lesion; SLAP, superior labrum anterior and posterior.
b Ratio of bone defect to diameter of the nonoperative side.
c There are some overlaps.
Postoperative Measurements
All patients returned to play at their previous competitive levels after surgery. Evaluations of surgical variabilities using postoperative CT images are shown in Table 2. In 87% of shoulders, the transferred coracoid was placed <5 mm from the glenoid surface. In 2 shoulders (1.3%), the transferred coracoid stuck out laterally from the joint surface, and the lengths were both <2 mm; there were no adverse clinical effects. Nonunion of the transferred coracoid was observed in 16 shoulders (10.7%). The coracoid fragment was displaced in 12 shoulders: 4 cases were recognized as a fibrous union, and there were no signs of screw loosening or any displacement. The loosened screws that could migrate were removed in 7 cases with notable displacement. Partial bone absorption was seen in 2 cases despite the union of the transferred coracoid.
Postoperative Measurements a

a Data are reported as mean ± SD (range) or No. (%) of shoulders unless otherwise indicated. ABD 0, abduction at 0°; ABD 90, abduction at 90°; AE, anterior elevation; ER, external rotation; IQR, interquartile range.
b Difference vs the nonoperative side.
There were 2 shoulders with postoperative deep infection that were successfully treated using arthroscopic irrigation and administration of antibiotics. Union of the transferred coracoid was achieved in both cases. There were 2 recurrent dislocations (1.3%), which were on-track lesions. Both patients experienced redislocation after returning to competition, despite nonunion of the transferred coracoid because the fibrous union was subclinical, and each patient required revision surgery to return to competition again. Osteoarthritic changes (grade I) were noted in 3 cases, all of which were asymptomatic. Transient axillary nerve palsy was noted in 3 cases, but the symptoms were resolved in 3 months. The mean postoperative Rowe score was 98.9 (range, 75-100), which was significantly better than the preoperative Rowe score (P < .001).
Clinical Results of Shoulders With Glenoid Defects <10% vs ≥10%
There were 58 cases (38.9%) with a glenoid defect ≥10% (Table 3). Significant differences were observed in age and on-track/off-track status between cases with defects of <10% and ≥10%; significantly more off-track cases had a defect ≥10% (P < .001). The presence of a ≥10% glenoid defect did not affect surgical results (time, length and location of the transferred coracoid, screw inclination angle) or clinical outcomes including the postoperative Rowe score and postoperative rates of infection, recurrence, and nonunion of the transferred coracoid.
Comparison of Clinical Results Between Cases With <10% and ≥10% Glenoid Defect a

a Data are reported as mean ± SD (range) or No. (%) of shoulders unless otherwise indicated. Bolded P values indicate statistically significant difference between groups. ABR, arthroscopic Bankart repair; BMI, body mass index; HSL, Hill-Sachs lesion; IQR, interquartile range.
b Ratio of bone defect to diameter of the nonoperative side.
c Welch t test.
d Fisher exact test.
e Chi-square test.
f Mann-Whitney U test.
Clinical Results and Factors Associated With Nonunion of the Transferred Coracoid
We next investigated whether nonunion of the transferred coracoid is associated with negative results (Table 4). There were no significant differences in patient characteristics (age, sex, dominant or nondominant side, height, body weight, and body mass index), revision surgery, or degree of injury (presence of a glenoid defect, OBL and Hill-Sachs lesion size, and on-track/off-track status) between cases with union of the transferred coracoid and those with nonunion of the transferred coracoid. Surgical results (time, length and location of the transferred coracoid, screw length, and inclination angle) and postoperative infection rate did not relate to nonunion of the transferred coracoid. Postoperative recurrence rates did not differ between the groups, but the postoperative Rowe score (total, stability, and function) was significantly lower in the nonunion group (P = .004).
Clinical Results and Factors Associated with Nonunion of the Transferred Coracoid a

a Data are reported as mean ± SD (range) or No. (%) of shoulders unless otherwise indicated. Bold P values indicate statistically significant difference between groups. ABR, arthroscopic Bankart repair; BMI, body mass index; HSL, Hill-Sachs lesion; IQR, interquartile range.
b Welch t test.
c Fisher exact test.
d Chi-square test.
e Mann-Whitney U test.
Postoperative CT scans >1 year after surgery showed union of the transferred coracoid and successful repair of the glenoid defect, with union of the bone fragment in all cases (29 patients), despite variances in the position of the transferred coracoid (Figure 3). The diameter of the glenoid increased from 24.8 ± 1.7 mm to 28.0 ± 1.8 mm postoperatively (mean increase, 13.1% [95% confidence interval [CI], 9.9%-16.3%]; P < .001), and the area of the glenoid articular surface increased from 761.1 ± 78.5 mm2 to 840.9 ± 89.9 mm2 (mean increase, 10.6% [95% CI, 8.5%-12.7%]; P < .001). Detailed results are described in Appendix Table A1.

Postoperative morphology of the glenoid surface in cases with osseous bony Bankart lesion. Three-dimensional computed tomography images of a patient with a bony glenoid lesion. The coracoid fragment was fixed onto the repaired bony Bankart fragment, which had achieved bony union. The left shoulder of an 18-year-old man (A) before surgery, (B) just after surgery, and (C) 3 years after surgery. The right shoulder of an 18-year-old man (D) before surgery, (E) just after surgery, and (F) 2 years after surgery. The right shoulder of a 19-year-old man (G) before surgery, (H) 3 months after surgery, and (I) 3 years after surgery.
Discussion
We investigated the effectiveness of a combined arthroscopic Bankart repair and open Bristow procedure in the management of traumatic anterior shoulder instability in collision sports athletes, with a focus on osseous glenoid lesions. Surgical outcomes as assessed using the Rowe score showed significant improvement postoperatively, and all patients returned to play at their previous competition levels. The presence of an osseous glenoid defect did not affect clinical outcomes. There were 2 recurrent dislocations, both of which were associated with nonunion of the transferred coracoid. There were 16 shoulders with nonunion of the transferred coracoid, and nonunion of the coracoid was related to significantly lower postoperative Rowe scores. We could not define any risk factors for nonunion, including patient characteristics, degree of injury, or surgical results. This surgical method also improved glenoid bone morphology by restoring osseous glenoid defects.
Traumatic anterior shoulder instability in collision sports athletes often involves osseous injuries of the glenoid and subsequent off-track status, thereby increasing the likelihood of recurrent instability. 30 Arthroscopic osseous Bankart repair can improve the morphology of the glenoid after the bony union is achieved. 12 However, the nonunion rate is not low in this procedure. 21 Therefore, competitive athletes do not usually want the uncertainty of the outcomes of this procedure. In addition, the coracoid transfer procedure has been shown to be beneficial in the management of these patients. However, some patients may report recurrent instability caused by the unrepaired soft tissue and OBL. 15 Some surgeons perform the combined Bankart repair and Bristow procedure or Latarjet arthroscopically (arthroscopic Bankart-Bristow-Latarjet procedure), but OBLs are commonly resected as the Bankart repair is carried out after the coracoid transfer. 2,13 Notably, a combined arthroscopic Bankart repair and open Bristow procedure has strengths in treating soft tissue and osseous lesions. Specifically, our surgical method can accurately reduce and arthroscopically fix OBLs, which are common in collision sports athletes with traumatic anterior shoulder instability, while performing the Bristow procedure. We showed that good clinical outcomes could be obtained using this procedure in shoulders with or without osseous glenoid lesions. Our study did not allow us to discuss whether to resect or repair an OBL; however, we demonstrated that repairing the OBL did not have negative outcomes, such as nonunion of the transferred coracoid, but might contribute to the restoration of the glenoid articular surface. 12 We speculate that the repaired Bankart lesion may act as a scaffold and the transferred coracoid may act as a bone graft to enhance repair of the glenoid defect. 14
Postoperative CT images showed variabilities in the surgical procedure such as screw fixation angle and the position of the transferred coracoid. However, they were not associated with nonunion of the transferred coracoid. Our data indicated that satisfactory clinical outcomes could be achieved when the screw was inserted within 0° to 30° as long as the transferred coracoid was placed and fixed firmly at the intended position. Furthermore, the position of the transferred coracoid relative to the glenoid articular surface may not be so critical when osseous glenoid lesions are repaired sufficiently, with the coracoid transfer contributing to shoulder stability via a sling effect. 29
The occurrence rate of nonunion of the transferred coracoid in this study is comparable with that in other studies of Bristow and Latarjet procedures. 2,11,31 In this study, nonunion of the transferred coracoid was associated with significantly lower Rowe scores. Any risk factors for nonunion including patient characteristics, degree of injury, or surgical results were not identified. However, 14 of 16 patients with nonunion of the transferred coracoid were able to return to their previous competitive levels without any recurrence. The coracoid transfer procedure has its strength in buttressing the repaired OBL and improving shoulder stability via the extra-articular sling effect, while the additional arthroscopic Bankart repair reinforces intrinsic stability. 29 Indeed, we noted fibrotic tissue development at the anterior joint capsule beneath the subscapularis in patients who underwent surgery to remove the loosened screw, which might have contributed to the stability. It is important that the coracoid artery and the vessels at the anterior surface of the glenoid are preserved while soft and osseous lesions are carefully repaired for an adequate clinical outcome. 1
We acknowledge the limitations of this study. The medical records of patients from a single institution with a nonuniform follow-up period were reviewed retrospectively. The number of cases was based on availability rather than a sample size assessment, and a control group was not included in this study. This study comprised 21 cases of revision Bankart repair but with a potential selection bias. The comparison between the coracoid union and nonunion cases (133 vs 16 cases) was underpowered to detect differences in clinical outcomes. Postoperative CT >1 year after surgery could not be performed in all cases, owing to the risk of radiation exposure. These scans were therefore taken in limited, clinically necessary cases where arthroscopic OBL repair and the Bristow procedure were still being conducted, especially at the beginning of this series, because of concerns regarding the irregularity of the glenoid surface. 23 The recent series included cases of initial dislocation without a glenoid defect. Based on a 2019 study, a low postoperative recurrence rate after isolated arthroscopic Bankart repair can be expected. 22 However, pain was often the only subjective concern when the collision sports athlete was initially injured, especially when OBLs were associated; therefore, the number of dislocations reported by patients might be inaccurate and was not one of the analysis items. Glenoid bone loss at the anterior rim caused by the suture anchor technique after Bankart repair can be another concern, even if there are no preoperative glenoid defects for competitive collision sports athletes. 9 Although our combined procedure showed reliable clinical results, additional investigations are needed to explore the indications of bone morphology, in terms of the reduction of time, cost, and potential complications. 18
Conclusion
The findings of the current study suggested that a combined arthroscopic Bankart repair and open Bristow procedure is effective in treating traumatic anterior shoulder instability in collision sports athletes with or without osseous glenoid lesions. This surgical method improved clinical outcomes and bone morphology in patients with osseous glenoid lesions.
Footnotes
Acknowledgment
The authors are profoundly appreciative of Tomoshige Tamaki, MD, for his excellent clinical contribution and friendship. In addition, the authors are deeply grateful for the editorial education given by Kay Daugherty, Campbell Foundation, Memphis, Tennessee.
Final revision submitted November 20, 2020; accepted December 21, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.B.P. has received education payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from St Luke’s International University (17-R038).
Appendix
Postoperative Changes of the Postoperative Diameter and Area of the Glenoid Articular Surface in the Patients With OBL a

| Diameter, mm | Area, mm2 | ||||||
|---|---|---|---|---|---|---|---|
| No. | Age, y | Size of OBL, % b | Preoperative | Postoperative | Preoperative | Postoperative | Follow-up, y |
| 1 | 18 | 1.3 | 22.1 | 26.7 | 775 | 934 | 3.5 |
| 2 | 19 | 4.2 | 25.4 | 26.8 | 735 | 829 | 2.6 |
| 3 | 19 | 2 | 27.2 | 31.5 | 816 | 948 | 3 |
| 4 | 17 | 10.6 | 23 | 27.5 | 738 | 832 | 3.4 |
| 5 | 18 | 3 | 23.2 | 28.2 | 696 | 800 | 3 |
| 6 | 19 | 2 | 21.1 | 28.5 | 741 | 875 | 2.5 |
| 7 | 20 | 5 | 23.2 | 26.7 | 688 | 711 | 2.1 |
| 8 | 18 | 9.2 | 22.5 | 29.1 | 688 | 783 | 3 |
| 9 | 20 | 10.2 | 26.6 | 28.5 | 934 | 948 | 1.5 |
| 10 | 17 | 5.2 | 25.1 | 30.5 | 824 | 912 | 2 |
| 11 | 18 | 4.2 | 24.4 | 29.9 | 698 | 750 | 2 |
| 12 | 19 | 6.5 | 25.3 | 26.8 | 809 | 859 | 2 |
| 13 | 20 | 13.4 | 23.8 | 26.2 | 727 | 773 | 1.8 |
| 14 | 19 | 5.1 | 27.3 | 31.5 | 774.9 | 830 | 1.6 |
| 15 | 15 | 6.8 | 26.1 | 28.9 | 764 | 890 | 1.5 |
| 16 | 16 | 4.2 | 25.1 | 28.8 | 741 | 825 | 2.2 |
| 17 | 18 | 3.3 | 27.5 | 30.5 | 904 | 986.1 | 1.4 |
| 18 | 18 | 7.7 | 25.1 | 25.9 | 672.6 | 720 | 1.6 |
| 19 | 19 | 11.3 | 27.6 | 30.9 | 886.5 | 1072.7 | 1.5 |
| 20 | 18 | 7.8 | 24.7 | 27.2 | 735.2 | 852.8 | 1 |
| 21 | 18 | 2.0 | 26.6 | 27.4 | 816.7 | 822 | 1.3 |
| 22 | 17 | 4.5 | 24.1 | 26.2 | 711 | 751 | 1.5 |
| 23 | 17 | 6.8 | 22.9 | 28 | 668.4 | 768.2 | 1.2 |
| 24 | 23 | 3.7 | 23.6 | 24.9 | 585.7 | 640.9 | 2.2 |
| 25 | 17 | 6.5 | 24.9 | 26.9 | 680.9 | 773.5 | 1.5 |
| 26 | 20 | 3.2 | 26.8 | 28.1 | 839.8 | 872.8 | 1.3 |
| 27 | 22 | 4.7 | 26.8 | 26.4 | 734.8 | 816.2 | 1 |
| 28 | 19 | 5 | 23.4 | 27.1 | 823.5 | 912.4 | 1.7 |
| 29 | 20 | 2.9 | 24.2 | 26 | 863.2 | 899.1 | 2.1 |
| Mean ± SD | 5.5 ± 3.0 | 24.8 ± 1.7 | 28.0 ± 1.8 | 761.1 ± 78.5 | 840.9 ± 89.8 | 2.0 | |
| Range | 1.3-13.4 | 21.1-27.6 | 24.9-31.5 | 585.7-934 | 640.9-1072.7 | 1-3.5 | |
a OBL, osseous Bankart lesion.
b Compared with the glenoid diameter of the nonoperative side.