
Abstract
Background:
Knee proprioception is believed to be deficient after anterior cruciate ligament (ACL) injury. Tests of joint position sense (JPS) are commonly used to assess knee proprioception, but their psychometric properties (PMPs) are largely unknown.
Purpose:
To evaluate the PMPs (reliability, validity, and responsiveness) of existing knee JPS tests targeting individuals with ACL injury.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
PubMed, Allied and Complementary Medicine, CINAHL, SPORTDiscus, Web of Science, Scopus, CENTRAL, and ProQuest databases were searched to identify studies that assessed PMPs of knee JPS tests in individuals with ACL injury. The risk of bias for each included study was assessed and rated at the outcome level for each knee JPS test. Overall quality and levels of evidence for each PMP were rated according to established criteria. Meta-analyses with mean differences were conducted using random effects models when adequate data were available.
Results:
Included were 80 studies covering 119 versions of knee JPS tests. Meta-analyses indicated sufficient quality for known-groups and discriminative validity (ACL-injured knees vs knees of asymptomatic controls and contralateral noninjured knees, respectively), owing to significantly greater absolute errors for ACL-injured knees based on a strong level of evidence. A meta-analysis showed insufficient quality for responsiveness, which was attributed to a lack of significant change over time after diverse interventions with a moderate level of evidence. Statistical heterogeneity (I 2 > 40%) was evident in the majority of meta-analyses. All remaining PMPs (reliability, measurement error, criterion validity, convergent validity, and other PMPs related to responsiveness) were assessed qualitatively, and they failed to achieve a sufficient quality rating. This was a result of either the study outcomes not agreeing with the statistical cutoff values/hypotheses or the level of evidence being rated as conflicting/unknown or based on only a single study.
Conclusion:
Knee JPS tests appear to have sufficient validity in differentiating ACL-injured knees from asymptomatic knees. Further evidence of high methodologic quality is required to ascertain the reliability, responsiveness, and other types of validity assessed here. We recommend investigations that compare the modifiable methodologic components of knee JPS tests on their PMPs to develop standardized evidence-based tests.
Anterior cruciate ligament (ACL) rupture is a common injury, particularly in sports, with an annual incidence of 68.6 isolated tears per 100,000 person-years in the United States. 93 Treatment involves extensive rehabilitation with or without reconstructive surgery. Despite treatment, approximately 1 in 4 young athletes who return to high-risk sports, such as football and skiing, will experience a secondary ACL injury. 107 It is widely believed that ACL injury compromises neuromuscular control and proprioceptive acuity of the knee and may contribute to the increased risk for secondary injury. 48,72
Proprioceptive receptors in muscles, skin, and joints convey afferent information to the brain regarding sensations including tension, effort, force, movement, and position. 82,91 This information is subsequently interpreted by the central nervous system, which in turn conveys efferent signals to guide behavioral motor responses and avoid injury. 13,75 The presence of mechanoreceptors in the ACL has been well documented in histologic studies, 20,40,41,95,112 and the damage or loss of these receptors may negatively influence knee proprioception. 1 Proprioceptive acuity tests of the knee are therefore prevalent in the literature. 49
Assessing knee proprioception involves testing 1 specific submodality of proprioception, most often either joint position sense (JPS) or threshold to detect passive motion. 49 Differentiating submodalities of proprioception is important given the lack of correlation among tests that attempt to quantify them. 64 Meta-analyses have found significantly poorer knee proprioception among ACL-injured knees as compared with the contralateral noninjured knees of the same individuals 58,87 and with asymptomatic control groups, 87 with knee JPS tests showing greater differences than movement discrimination tests showed. However, the absolute differences in degrees of knee flexion were <1°, and differences versus asymptomatic controls are not always evident. 73 A major reason for the inconsistent results is likely the lack of standardized test procedures.
The psychometric properties (PMPs; eg, reliability, validity, and responsiveness) of proprioception assessment methods have not been established across joints or tests, and 2 systematic reviews have emphasized the need for further research in this area. 46,49 Specifically, common tests of knee proprioception lack sufficient evidence to draw reliable and valid conclusions based on their outcome measures. 87 A systematic review by Smith et al 100 found varying evidence for the reliability of knee JPS tests across pathologic and asymptomatic populations; the authors recommended additional examination of such tests among those with ACL injury. This conflicting evidence may be in part due to the many modifiable components of knee JPS tests, such as joint angles, reproduction procedure, and body position. A plethora of knee JPS tests therefore exists, and this systematic review of the updated literature assimilates the current evidence pertaining to their PMPs. It is intended to provide guidance for those seeking to evaluate knee JPS, as well as to inform future researchers aiming to develop improved methods of testing.
This article forms part of a systematic review series investigating the PMPs of all knee proprioception tests targeting individuals with ACL injury and asymptomatic controls. 8 The aim of the current systematic review is to corroborate the evidence for the PMPs of all knee JPS tests that have been applied in the scientific literature targeting those with ACL injury. In line with previous meta-analyses, we hypothesized that knee JPS tests would show sufficient validity regarding differentiation between ACL-injured and asymptomatic knees. We also hypothesized that a lack of evidence would make it difficult to sufficiently ascertain the quality of all remaining PMPs of knee JPS tests among individuals with ACL injury.
Methods
We adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for conducting this review, 69,97 as stated in our protocol, 8 which was registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration CRD42018108014).
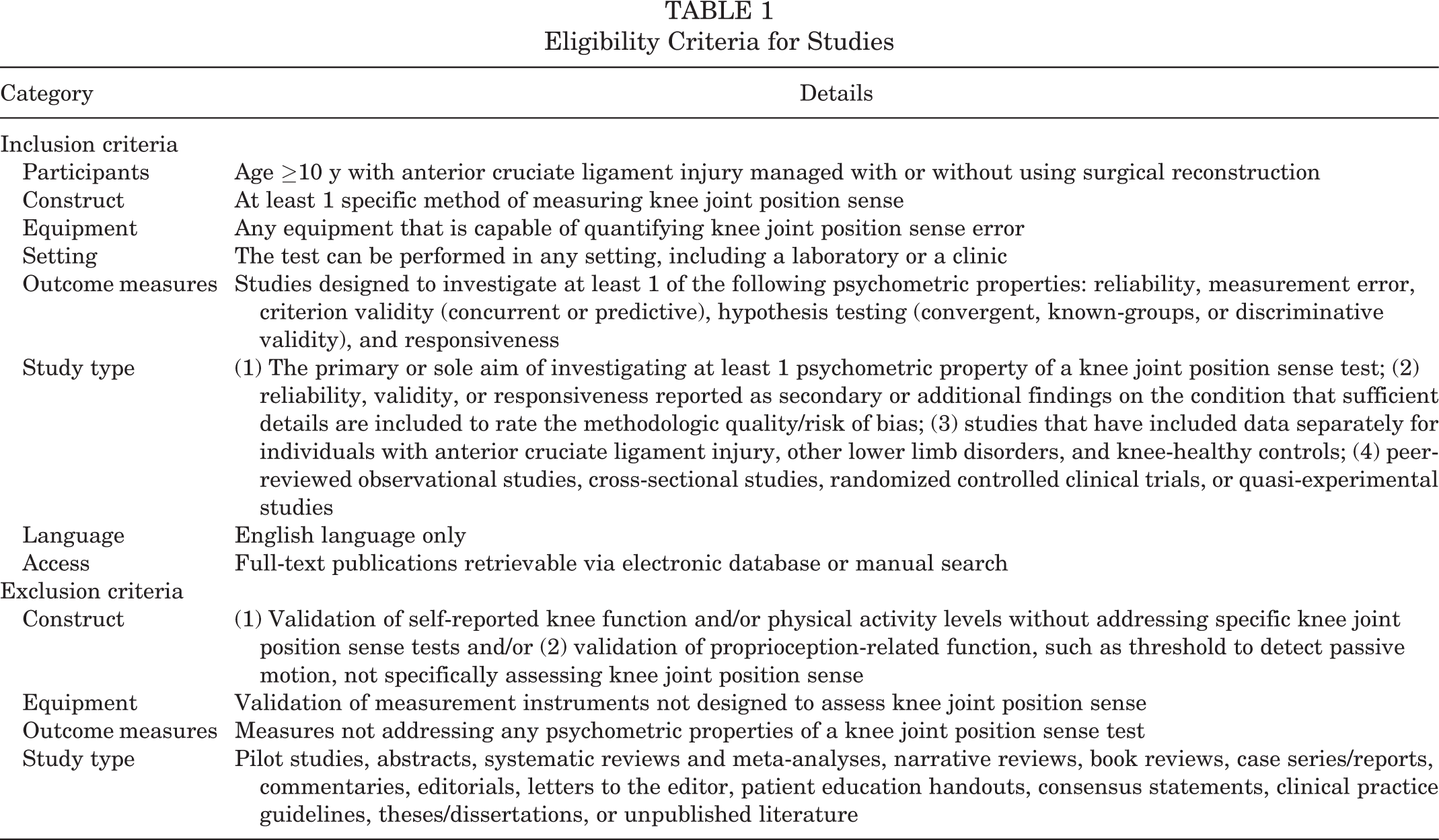
Eligibility Criteria
Eligibility criteria for inclusion and exclusion of studies are detailed in Table 1. Briefly, studies were to include individuals ≥10 years of age with ACL injury managed with or without using surgical reconstruction who performed at least 1 test of knee JPS. Studies must have investigated at least 1 PMP (reliability, validity, or responsiveness) relating to the outcome measures of the JPS tests.
Eligibility Criteria for Studies
Search Strategy and Study Selection
A systematic search was performed by the first author (A.S.) using the following databases between their inception and March 3, 2020: PubMed, Allied and Complementary Medicine (via EBSCO), CINAHL (via EBSCO), SPORTDiscus (via EBSCO), Web of Science, Scopus, the Cochrane Central Register of Controlled Trials (CENTRAL), and Physical Education Index (via ProQuest). Search terms and strategies are elaborated in the published review protocol. 8 In addition, searches were performed via Google Scholar using relevant search terms.
All identified articles were imported to EndNote X9.3.1 (Clarivate Analytics Software) and then exported to Covidence systematic review software (Veritas Health Innovation) where duplicates were removed. Two authors (A.S., E.T.) independently screened all titles and abstracts for suitability according to the predetermined eligibility criteria. The full texts of the potentially eligible articles were retrieved and screened independently by the same 2 authors. Disagreements were resolved either by consensus or by consulting a third author (A.A.). Reference lists of the included articles were screened for any potential additional studies not found in the systematic search.
Data Extraction and Risk-of-Bias Assessment
Data were extracted from all eligible studies that reported PMPs of knee JPS tests in individuals with ACL injury as primary or secondary (additional) findings. Extracted study information included the following: authors, year of publication, study design, population characteristics (number of participants, age, sex distribution, height, weight, treatment type, time since injury/surgery, activity level), testing procedures, statistical analyses, results relating to knee JPS PMP outcome measures, and any other data required for risk-of-bias (RoB) assessment. If data were missing or inadequate, an email was sent to the authors requesting the required information.
The RoB was assessed and rated using the Consensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN) RoB checklist. 70 Thus, the methodologic quality of each study was rated according to a 4-point rating scale: inadequate (high RoB), doubtful, adequate, and very good (low RoB). Studies rated inadequate were not included in evidence syntheses. The following PMPs were then examined at the outcome level:
Reliability
Measurement error
Criterion validity: concurrent or predictive
Hypothesis testing for construct validity:
Convergent versus other outcome measures
Discriminative, which was operationally defined as ACL-injured knees versus the contralateral asymptomatic knees of the same individuals
Known groups, which was operationally defined as ACL-injured knees versus either asymptomatic knees of other individuals or ACL-injured knees of otherwise asymptomatic individuals
Responsiveness: criterion and construct approach
Data extraction and RoB evaluation were piloted using 2 studies chosen to include what was assumed to be the most common general PMPs: hypothesis testing 53 and responsiveness. 14 Piloting was achieved by all authors independently performing data extraction and rating the studies for RoB before meeting to discuss any concerns and to arrive at a consensus. Data from all articles were then extracted independently by an assigned author (A.S., 38%; E.T., 17%; A.A., 15%; U.R., 15%; C.K.H., 14%) and verified by a second (A.S., 25%; E.T., 31%; A.A., 28%; C.K.H., 15%), ensuring that all pairs of authors worked together on at least 2 articles. A third author was assigned to each article in case of any disagreements, but all were resolved through consensus.
Within studies, JPS tests were considered separate if they differed regarding modifiable components of reproduction method, direction of movement, body position, measurement equipment, and test procedure but not if they differed for target angle (TA) because some studies used data from multiple TAs for the same outcome. In instances where an ACL group underwent reconstruction during the study, it was classified as having ACL reconstruction (ACLR) as opposed to being ACL deficient (ACLD). Also, when participants were followed up over time and known-groups validity or discriminative validity was examined, follow-up data for only the last test were extracted. This was done to provide more stable and homogeneous results. In studies where knee JPS was assessed during the same testing session with and without an intervention, such as Kinesio tape 15 or vibration, 71 data for known-groups and discriminative validity were extracted just for baseline. Knee JPS can be analyzed using absolute error (AE), constant error, or variable error. For this review, only data for AE were extracted because constant and variable errors were seldom reported.
Quality Assessment of PMPs
The quality of each PMP was evaluated according to our protocol 8 using a criterion list adapted from Prinsen et al 81 (see Appendix Table A1, available online as Supplemental Material). Briefly, ratings of sufficient, indeterminate, or insufficient depended on whether the synthesized study outcomes were in agreement with the threshold cutoff values of relevant statistical parameters or hypotheses. Regarding hypothesis testing for construct validity and responsiveness, ratings of sufficient and insufficient required 75% of the findings to be in favor of the hypothesis (positive) or not (negative), respectively. If <75% of the findings were in agreement, the quality of the PMP was rated as inconsistent owing to the conflicting level of evidence. In instances when a PMP was evaluated only in studies with an RoB rating of inadequate or was not investigated at all, the quality of that PMP was denoted “not estimable” because of the unknown level of evidence.
Level of Evidence
The level of evidence for each PMP was ascertained according to a scale adapted by Kroman et al
60
(Appendix Table A2, available online). Rating criteria were as follows:
Strong: the test was evaluated in multiple studies of adequate RoB rating or at least 1 study of very good RoB rating (implying a low RoB).
Moderate: the test was evaluated in multiple studies of doubtful RoB rating or at least 1 study of adequate RoB rating.
Limited: the test was evaluated in 1 study of doubtful RoB rating.
Conflicting: the test was evaluated in studies with contradictory findings.
Unknown: the test was evaluated in studies of inadequate RoB rating or not investigated at all.
Meta-analysis
Meta-analyses for each PMP were performed using the Review Manager computer program (RevMan Version 5.3; Nordic Cochrane Centre, Cochrane Collaboration) when adequate (homogeneous) data were available from at least 3 studies with a doubtful, adequate, or very good RoB rating. A random effects model was applied to account for differences in the way that the studies were conducted in addition to the sampling error. 18 The mean difference (MD) was used rather than the standardized MD, as only outcome measures in the same unit (AE) were included and for greater statistical power. 103 When the means and standard deviations (SDs) of the AE were not reported but median values with measures of dispersion were, means and SDs were estimated per the method of Wan et al. 105 Statistical heterogeneity was considered present if the I 2 statistic exceeded 40%. 28 Funnel plots with trim-and-fill analyses 29 to help identify and correct for the presence of publication bias were considered appropriate only when the following criteria were met, as described by Ioannidis and Trikalinos 51 : the inclusion of at least 10 studies (with statistically significant results in at least 1 study), statistical heterogeneity <50%, and a ratio >4 for the maximal to minimal variance across studies. Subgroups were created within each meta-analysis according to each JPS test procedure, such as passive-active (passive movement to the TA and active movement to the reproduction angle), to investigate potential differences in outcome related to this factor. Sensitivity analyses were performed for study population and methodologic quality when appropriate by restricting the meta-analyses to ACLD or ACLR and studies with an adequate or very good ROB rating, respectively. Statistical significance was set at P < .05.
Control group data were obtained for the nondominant legs, when available, to provide a more stringent comparison with the injured legs of ACL groups to analyze known-groups validity. When information of side was provided without indicating dominance, the left leg was chosen to increase the likelihood of selecting the nondominant leg. For responsiveness, when knee JPS was tested over time, just the data comparing baseline and the last time point were used for analysis. In addition, when an intervention included a control condition and a placebo condition, such as sham Kinesio tape 15 or placebo knee brace, 108 data were limited to comparisons between the control and intervention conditions to evaluate responsiveness.
Results
Search Results
The electronic database search yielded 2978 studies, and manual searches yielded an additional 63. After removal of duplicates, the titles and abstracts of 2527 articles were screened, of which 462 full-text articles were then screened for eligibility. Subsequently, 80 articles were included in this review (Figure 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram illustrating inclusion of studies. ACL, anterior cruciate ligament.
Characteristics of the Studies
Study characteristics are provided in Appendix Table A3 (available online). To summarize, in the 80 studies, we identified 2475 participants with a unilateral ACL injury from 112 cohorts. Of these, 81 cohorts were classified as having ACLR (17 of which were ACLD at inclusion but underwent ACLR during the study), and 31 were classified as being ACLD. Sex distribution was indicated for 99 (88%) ACL populations, revealing that 30% were female. The mean weighted age of the ACL populations was 27.91 years, as based on the 104 ACL populations for which the mean age was reported. Three studies 1,43,66 cited median age only, and 4 studies2,10,30,54 did not report age.
A total of 119 knee JPS tests were identified. The most common procedure was passive-active (54 tests), followed by active-active (25 tests), passive-passive (19 tests), passive–visual estimation (13 tests), and active-passive (1 test). The procedure was not reported or was unclear for 7 tests. In total, 74 tests were performed with participants seated; 16, side lying; 14, supine lying; 8, standing; 3, reclined; and 1, prone lying; and for 3 tests, this information was not indicated. The most common equipment used to measure the knee angle was a dynamometer (48 tests). The most common starting angle was 90° of knee flexion (47 tests), followed by 0° (23 tests), 60° (18 tests), and 30° (10 tests). Three tests used a specified range, 6 tests used >1 starting angle, and starting angle was not reported for 14 tests. The most common TA was 30° (38 tests), followed by 15° (24 tests), 60° (23 tests), and 45° (21 tests). More than 1 TA was used in 39 tests, unspecified TAs within a range or multiple ranges were used in 25 tests, and TA was not cited for 15 tests. The reproduction method was the ipsilateral leg in 101 tests, with a form of visual estimation in 13 tests and with the contralateral leg in 4 tests. The method was not reported for 1 test. Movement direction (toward the TA and reproduction angle) was extension for 61 tests, flexion for 33 tests, and a mixture of flexion and extension for 12 tests (eg, flexion toward TA but extension toward reproduction angle). Direction was not noted for 13 tests.
Assessment of RoB was performed at the outcome level (Appendix Table A4, available online). However, the RoB standards (ie, the questions that are scored) differ among PMPs to better reflect the specific study designs required; thus, some overall ratings differed for the same studies among PMPs. For example, 1 study 104 received an RoB rating of doubtful for known-groups validity but a lower rating of inadequate for convergent validity in part because the comparator outcome measures were not performed on the same day as were the knee JPS tests. One standard that was included for rating all PMPs was related to other important flaws in the design or statistical methods of the study. Considerations for this standard included but were not limited to the number of knee JPS test trials performed (a minimum of 5 trials was considered appropriate), sample size, description of the participant characteristics, and methodologic procedures. Thus, because the COSMIN checklist operates on a worst-score-counts principle, many of the studies received their lowest score for this standard; subsequently, the overall RoB rating was often equal to the score for this standard.
Assessment of Quality and Level of Evidence of the Studies
Reliability and Measurement Error
Test-retest reliability of knee JPS tests was analyzed among participants with ACLR in 3 studies, 6,62,68 in which measurement error was reported in 2 studies 6,68 (Table 2). However, all studies had an inadequate RoB rating (Appendix Table A4, available online). Thus, the quality of test-retest reliability and related measurement error was not estimable because of the unknown level of evidence.
Reliability and Measurement Error a

a A, active; ACLD, anterior cruciate ligament deficient; ACLR, anterior cruciate ligament reconstruction; COSMIN, Consensus-Based Standards for the Selection of Health Measurement Instruments; ICC, intraclass correlation coefficient; JPS, joint position sense; NR, not reported; P, passive; PMP, psychometric property; RoB, risk of bias; SDD, smallest detectable difference; TA, target angle.
b Ratings: +, sufficient; ?, indeterminate; –, insufficient; NA, not applicable (owing to rating of inadequate risk of bias).
c For intrasession reliability.
Intrasession reliability and associated measurement error were evaluated for 1 active knee JPS test in 1 study, 16 which had an RoB rating of very good (Appendix Table A4, available online). Thus, the intraclass correlation coefficient (2,1) of 0.06 (95% CI not reported) and SEM of 2.7° (without reference to minimal important change) (Table 2) indicated insufficient and indeterminate quality for intrasession reliability and associated measurement error, respectively, based on a strong level of evidence.
Criterion Validity
No gold standard knee JPS test exists; therefore, no studies that performed such a comparison were identified. In addition, no studies that investigated the predictive validity of knee JPS tests were identified. Concurrent validity (ie, comparison among knee JPS tests) was analyzed in 1 study, 30 which had an RoB rating of inadequate (Appendix Table A4, available online). Thus, the quality of criterion (concurrent) validity for knee JPS tests among individuals with ACL injury was not estimable because of an unknown level of evidence.
Convergent Validity
Convergent validity (ie, correlation between knee JPS and other outcome measures) was analyzed in 16 studies ∥ (Appendix Table A5, available online). In case of multiple correlations in the same study, all were given the same RoB rating: very good for 1 study, 47 doubtful for 9 studies, ¶ and inadequate for 6 studies 10,21,26,63,77,104 (Appendix Table A4, available online). The most commonly examined outcome measures were quadriceps strength, 21,62,74,104,111 hamstring strength, 21,62,74,104 hamstring to quadriceps ratio, 26,62,74,111 and knee laxity. 1,10,32,35 A meta-analysis was precluded because set criteria were not met. As 91.2% of the findings did not show correlations between the relevant knee JPS tests and the other outcome measures, we found insufficient quality for convergent validity of knee JPS tests. The level of evidence was determined to be moderate because of the multiple diverse outcome measures, and despite 1 study having an RoB rating of very good, the remaining 9 studies had an RoB rating of doubtful.
Hypothesis Testing
Known-Groups Validity
Known-groups validity was evaluated in 181 group comparisons across 52 studies # (Appendix Table A6, available online). All multiple within-study comparisons received the same overall RoB rating: very good for 3, 34,44,86 adequate for 4, 47,79,85,88 doubtful for 32, ** and inadequate for 13 studies †† (Appendix Table A4, available online). Meta-analyses including, when appropriate, subgroup comparisons and sensitivity analyses were thus performed as detailed in the following sections. The criteria for funnel plots with trim-and-fill analyses were not met by the studies.
ACL-Injured Knees vs Asymptomatic Controls
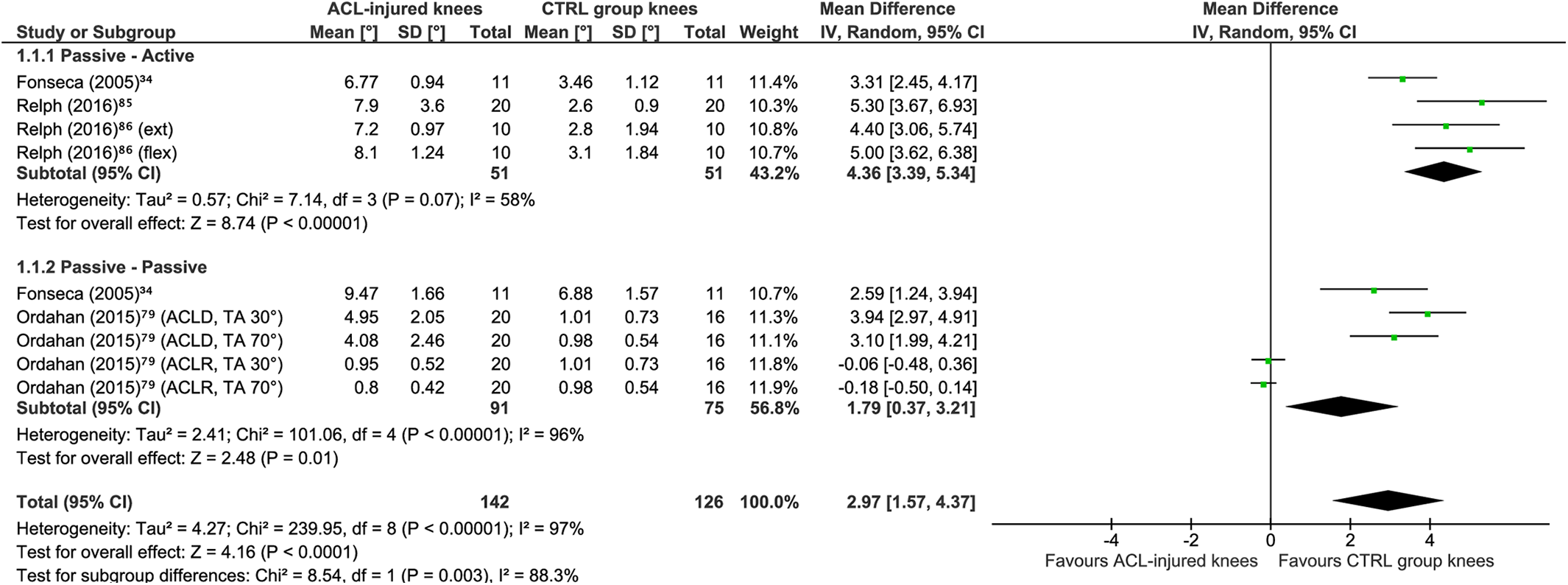
A meta-analysis included 59 comparisons between ACL groups and asymptomatic controls across 18 studies ‡‡ (Figure 2). ACL-injured knees showed significantly greater JPS error than did those of asymptomatic controls (MD, 0.70°; 95% CI, 0.40°-1.01°; P < .00001; I 2 = 91%). A sensitivity analysis for study quality was performed by including only studies with an adequate or very good RoB rating (Figure 3) (9 comparisons across 4 such studies 34,79,85,86 ). ACL-injured knees produced significantly greater JPS error than did asymptomatic controls (MD, 2.97°; 95% CI, 1.57°-4.37°; P = .00001; I 2 = 97%).

Meta-analysis comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament (ACL)–injured knees and the knees of healthy controls (known-groups validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. ACLD, anterior cruciate ligament deficient; ACLR, anterior cruciate ligament reconstruction; BPTP, bone–patellar tendon–bone; CTRL, control; ext, extension; flex, flexion; HT, hamstring tendon; IV, inverse variance; TA, target angle.
Meta-analysis including only studies with a risk of bias rating of adequate or very good comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament (ACL)–injured knees and the knees of healthy controls (known-groups validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. ACLD, anterior cruciate ligament deficient; ACLR, anterior cruciate ligament reconstruction; CTRL, control; ext, extension; flex, flexion; IV, inverse variance; TA, target angle.
Subgroups were created in the meta-analysis based on the type of JPS test: passive-active (29 comparisons across 11 studies §§ ), passive-passive (10 comparisons across 5 studies 7,34,65,79,111 ), active-active (14 comparisons across 4 studies 19,67,71,92 ), and passive–visual estimation (6 comparisons across 2 studies 89,90 ). Because of an insufficient number of studies, 1 meta-analysis subgroup (passive–visual estimation) was precluded, and only the other 3 subgroup meta-analyses were considered relevant (Figure 2). The JPS error was significantly greater for ACL-injured knees as compared with asymptomatic controls for passive-passive procedures (MD, 1.59°; 95% CI, 0.96° to 2.22°; P < .00001; I 2 = 95%) and was close to being significantly greater for ACL-injured knees for passive-active procedures (MD, 0.61°; 95% CI, –0.03° to 1.25°; P = .06; I 2 = 87%) and active-active procedures (MD, 0.26°; 95% CI, 0.00° to 0.51°; P = .05; I 2 = 60%). Sensitivity analyses comparing ACLD and ACLR separately against asymptomatic controls are detailed hereafter.
ACLD Knees vs Asymptomatic Controls
Twenty-four comparisons between ACLD knees and asymptomatic controls were identified across 8 studies. 7,32,34,79,80,86,90,114 ACLD knees produced significantly greater JPS errors than did asymptomatic controls (MD, 0.94°; 95% CI, 0.48°-1.39°; P = .0001; I 2 = 89%) (Figure 4). A sensitivity analysis limited to studies with only adequate or very good RoB ratings 34,79,86 revealed similar findings (MD, 3.56°; 95% CI, 2.84°-4.27°; P < .00001; I 2 = 50%) (Figure 5).

Meta-analysis comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament deficient (ACLD) knees (treated without using surgical reconstruction) and the knees of healthy controls (known-groups validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. CTRL, control; ext, extension; flex, flexion; IV, inverse variance; TA, target angle.
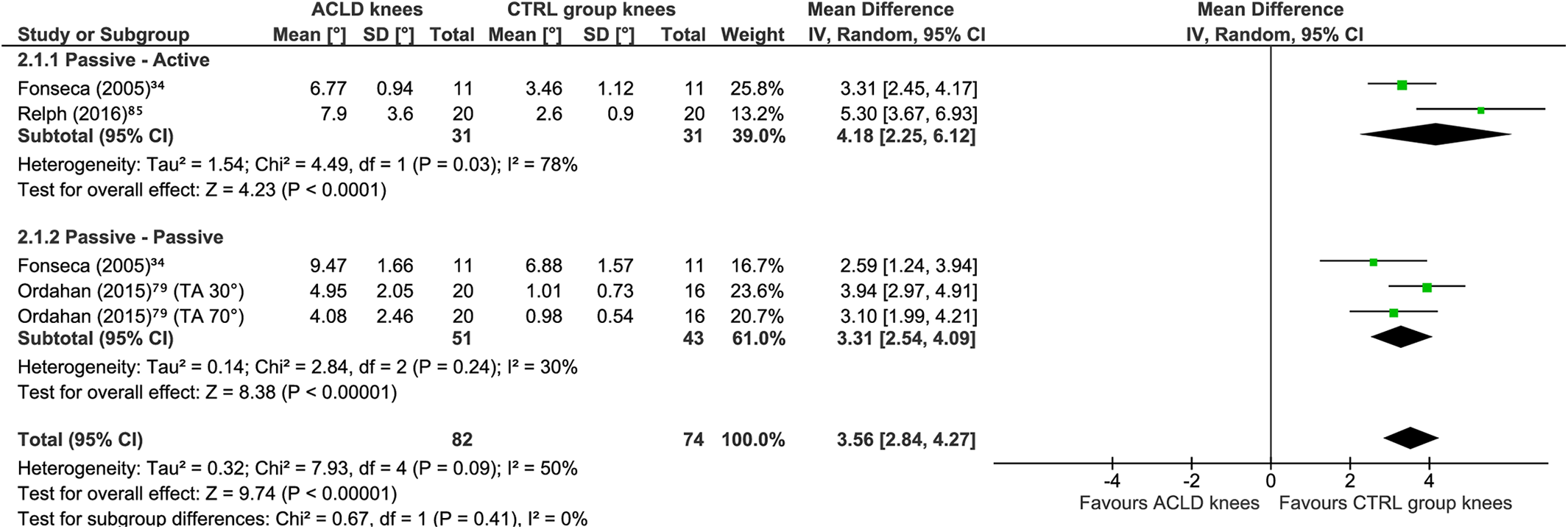
Meta-analysis including only studies with a risk of bias rating of adequate or very good comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament deficient (ACLD) knees (treated without using surgical reconstruction) and the knees of healthy controls (known-groups validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. CTRL, control; IV, inverse variance; TA, target angle.
ACLR Knees vs Asymptomatic Controls
After 35 comparisons between ACLR knees and asymptomatic controls across 13 studies, ∥∥ ACLR knees showed significantly greater JPS error as compared with asymptomatic controls (MD, 0.48°; 95% CI, 0.18°-0.78°; P = .002; I 2 = 80%) (Figure 6). A sensitivity analysis was precluded owing to an insufficient number of studies with RoB ratings of adequate or very good.

Meta-analysis comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament reconstruction (ACLR) knees and the knees of healthy controls. A random effects model with mean difference was used. Subgroups are shown per test procedure. BPTP, bone–patellar tendon–bone; CTRL, control; ext, extension; flex, flexion; HT, hamstring tendon; IV, inverse variance; TA, target angle.
ACLD vs ACLR Knees
Based on 10 comparisons across 3 studies, 32,59,80 a meta-analysis found significantly greater JPS error for ACLD knees than ACLR knees (MD, 0.80°; 95% CI, 0.29°-1.32°; P < .002; I 2 = 34%) (Figure 7). A sensitivity analysis was precluded owing to a lack of studies meeting the defined criteria.

Meta-analysis comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament deficient (ACLD) knees (treated without using surgical reconstruction) and anterior cruciate ligament reconstruction (ACLR) knees (known-groups validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. ext, extension; flex, flexion; IV, inverse variance; Std, standardized; TA, target angle.
Overall Quality of Known-Groups Validity and Level of Evidence
To summarize, knee JPS tests elicited significantly greater errors for ACL-injured knees as compared with healthy controls and for ACLD knees as compared with ACLR knees. Thus, the known-groups validity of knee JPS tests targeting individuals with ACL injury was sufficient. The sensitivity analysis supported these findings; thus, the level of evidence was rated as strong.
Discriminative Validity
Discriminative validity was analyzed in 146 comparisons across 44 studies ¶¶ (Appendix Table A7, available online). All relevant within-study comparisons received the same RoB rating, which was very good for 3 studies, 33,34,86 adequate for 3 studies, 47,79,85 doubtful for 26 studies, ## and inadequate for 12 studies a (Appendix Table A4, available online). Meta-analyses were performed with subgroup comparisons and sensitivity analyses when appropriate, as described hereafter. Funnel plots and trim-and-fill analyses were precluded owing to the aforementioned criteria not being met.
ACL-Injured vs Contralateral Noninjured Knees
A meta-analysis comparing knee JPS AE between ACL-injured knees (ACLD or ACLR) and the contralateral noninjured knees of the same persons included 57 comparisons across 22 studies. b ACL-injured knees showed significantly greater knee JPS error than did the contralateral knees (MD, 0.69°; 95% CI, 0.31° to 1.06°; P = .0003; I 2 = 87%) (Figure 8). A sensitivity analysis of 16 comparisons across 6 studies was performed. 33,34,47,79,85,86 Significantly greater JPS error was again seen for ACL-injured knees as compared with the contralateral knees of the same individuals (MD, 1.55°; 95% CI, 0.57° to 2.53°; P = .002; I 2 = 96%) (Figure 9). In addition, within the main analysis, subgroups based on test procedure were created for the following: passive-active (29 comparisons across 14 studies c ), passive-passive (12 comparisons across 6 studies 31,34,53,62,74,79 ), active-active (16 comparisons across 8 studies 16,27,33,43,50,53,67,71 ), passive–visual estimation (2 comparisons in 1 study, 89 thus precluding meta-analysis), and not reported (1 comparison in 1 study 15 ). Significantly greater errors were seen for the ACL-injured knees than the contralateral knees for test procedures that were passive-active (MD, 1.10°; 95% CI, 0.36° to 1.83°; P = .003; I 2 = 92%) and passive-passive (MD, 0.78°; 95% CI, 0.27° to 1.29°; P = .003; I 2 = 72%) but not active-active (MD, 0.11°; 95% CI, –0.33° to 0.55°; P = .63; I 2 = 35%).

Meta-analysis comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament (ACL)–injured knees (treated with or without using surgical reconstruction) and the contralateral healthy knees of the same individuals (discriminative validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. ACLD, anterior cruciate ligament deficient; ACLR, anterior cruciate ligament reconstruction; ext, extension; flex, flexion; IV, inverse variance; MJA, maximum joint amplitude; MVC, maximal voluntary contraction; P-F, poor-functioning; TA, target angle; W-F, well-functioning.
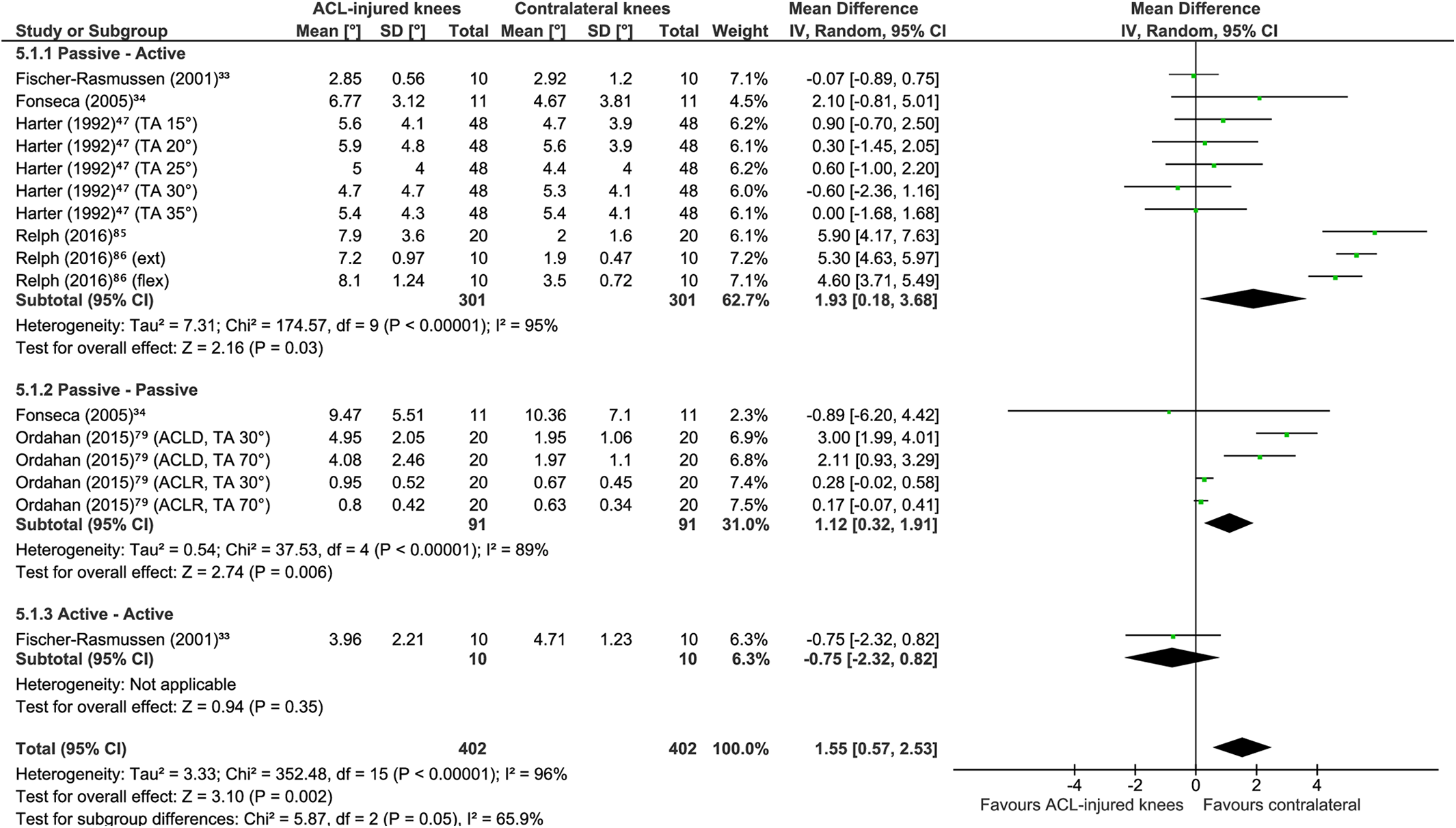
Meta-analysis including only studies with a risk of bias rating of adequate or very good comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament (ACL)–injured knees (treated with or without using surgical reconstruction) and the contralateral healthy knees of the same individuals (discriminative validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. ACLD, anterior cruciate ligament deficient; ACLR, anterior cruciate ligament reconstruction; ext, extension; flex, flexion; IV, inverse variance; TA, target angle.
ACLD vs Contralateral Noninjured Knees
For 24 comparisons between the knees of individuals with unilateral ACLD across 11 studies, d ACLD knees showed significantly greater knee JPS error (MD, 0.95°; 95% CI, 0.44° to 1.45°; P = .0003; I 2 = 77%) (Figure 10). A sensitivity analysis (7 comparisons across 4 studies 33,34,79,86 ) also showed significantly greater JPS errors for ACLD knees than for the contralateral knees of the same individuals (MD, 1.81°; 95% CI, 0.09° to 3.54°; P = .04; I 2 = 90%) (Figure 11). To elucidate the potential effects of test procedure on outcomes, the following subgroups of tests were created: passive-active (10 comparisons across 8 studies 32 –34,43,53,56,80,86 ), passive-passive (5 comparisons across 3 studies 34,53,79 ), active-active (8 comparisons across 4 studies 27,33,43,53 ), and not reported (1 comparison in 1 study 15 ). Greater JPS errors were evident for ACLD knees than for the contralateral knees for procedures that were passive-active (MD, 1.06°; 95% CI, 0.23° to 1.89°; P = .01; I 2 = 82%) and passive-passive (MD, 2.25°; 95% CI, 1.39° to 3.12°; P < .00001; I 2 = 17%) but not active-active (MD, 0.49°; 95% CI, –0.27° to 1.24°; P = .21; I 2 = 59%).
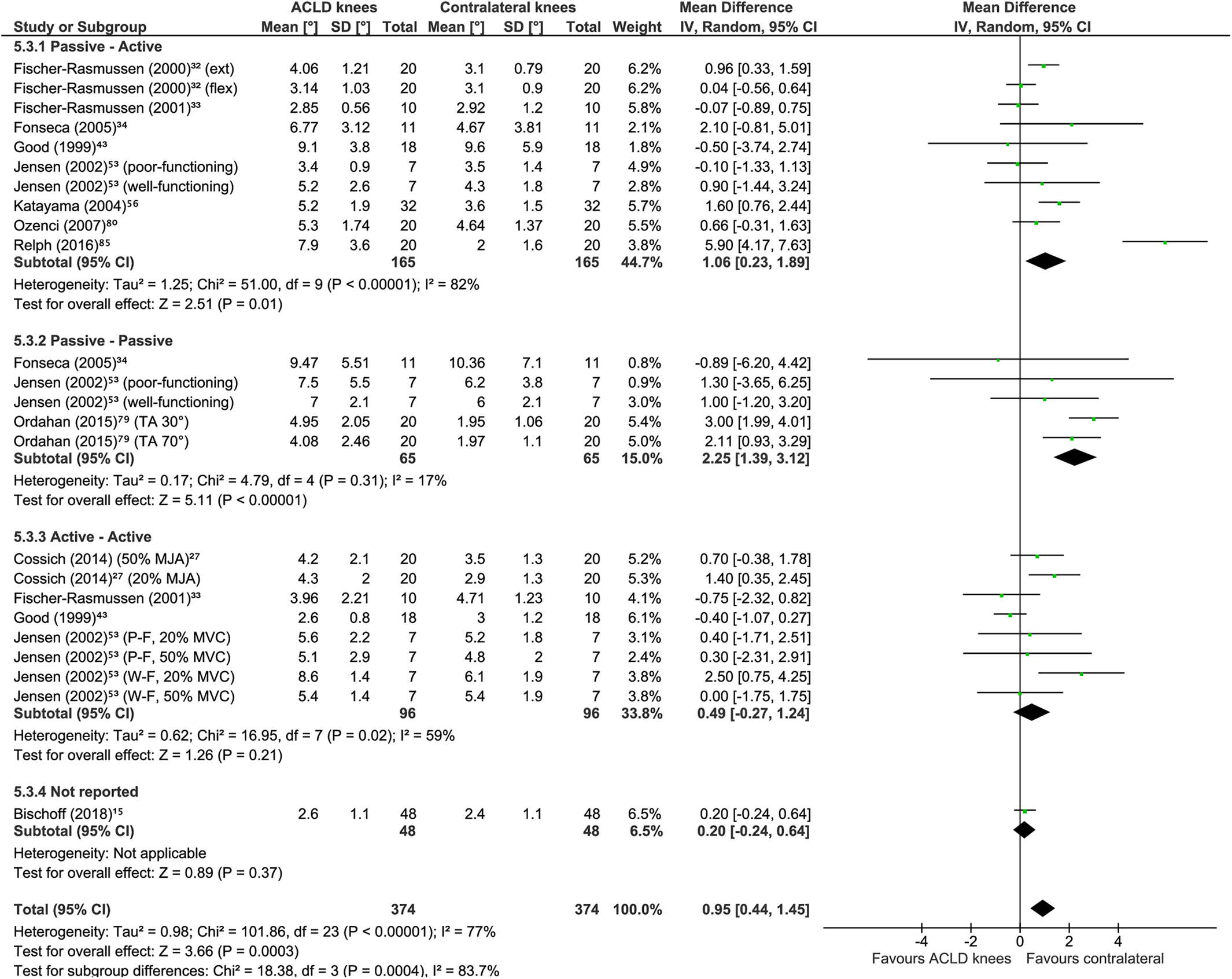
Meta-analysis comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament deficient (ACLD) knees (treated without using surgical reconstruction) and the contralateral healthy knees of the same individuals (discriminative validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. ext, extension; flex, flexion; IV, inverse variance; MJA, maximum joint amplitude; MVC, maximal voluntary contraction; P-F, poor-functioning; TA, target angle; W-F, well-functioning.
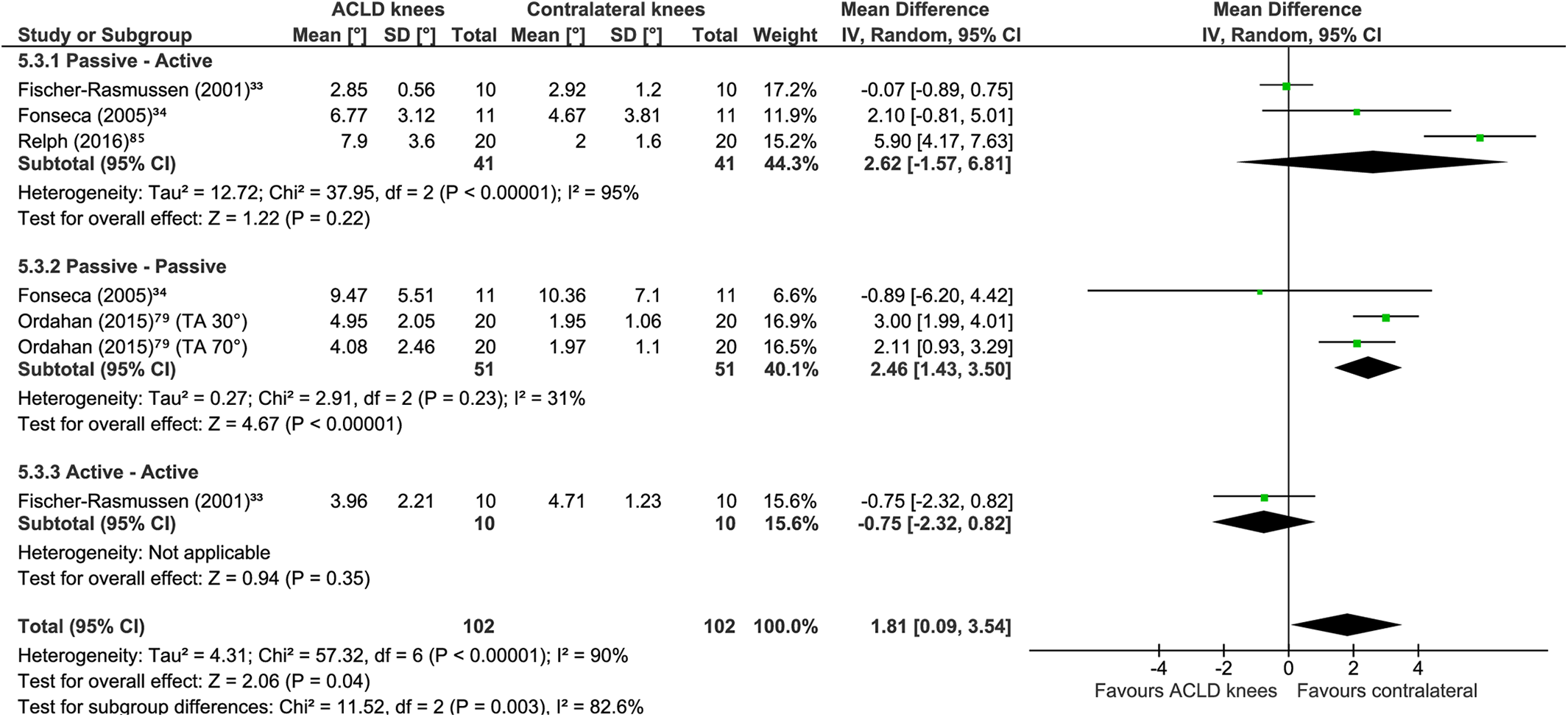
Meta-analysis including only studies with a risk of bias rating of adequate or very good comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament deficient (ACLD) knees (treated without using surgical reconstruction) and the contralateral healthy knees of the same individuals (discriminative validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. IV, inverse variance; TA, target angle.
ACLR vs Contralateral Noninjured Knees
For 36 comparisons between the knees of individuals with unilateral ACLR across 15 studies, e no statistically significant difference in knee JPS errors were found (MD, 0.47°; 95% CI, –0.03° to 0.96°; P = .06; I 2 = 89%) (Figure 12). A sensitivity analysis (9 comparisons across 3 studies 47,79,85 ) conversely revealed significantly greater knee JPS error for ACLR knees than for the healthy contralateral knees (MD, 1.36°; 95% CI, 0.08° to 2.65°; P = .04; I 2 = 97%) (Figure 13). The following subgroups of tests were also analyzed: passive-active (19 comparisons across 8 studies 31,32,47,55,80,85,89,99 ), passive-passive (7 comparisons across 4 studies 31,62,74,79 ), active-active (8 comparisons across 4 studies 16,50,67,71 ), and passive–visual estimation (separate meta-analysis precluded owing to 2 comparisons in only 1 study 89 ). JPS error was significantly greater for the ACLR knee as compared with the contralateral knee for passive-passive procedures (MD, 0.22°; 95% CI, 0.05° to 0.40°; P = .01; I 2 = 0%) and close to significant for passive-active procedures (MD, 0.95°; 95% CI, 0.01° to 1.89°; P = .05; I 2 = 93%); yet, no significant differences were seen for active-active (MD, –0.34°; 95% CI, –0.82° to 0.13°; P = .15; I 2 = 0%).

Meta-analysis comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament reconstruction (ACLR) knees and the contralateral healthy knees of the same individuals (discriminative validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. ext, extension; flex, flexion; IV, inverse variance; TA, target angle.

Meta-analysis including only studies with a risk of bias rating of adequate or very good comparing knee joint position sense absolute error group means in degrees of flexion between anterior cruciate ligament reconstruction (ACLR) knees and the contralateral healthy knees of the same individuals (discriminative validity). A random effects model with mean difference was used. Subgroups are shown per test procedure. ext, extension; flex, flexion; IV, inverse variance; TA, target angle.
Overall Quality of Discriminative Validity and Level of Evidence
To summarize, knee JPS tests generally elicited significantly greater errors for ACL-injured knees as compared with the healthy contralateral knees of the same individuals. Thus, the discriminative validity of knee JPS tests targeting individuals with ACL injury was rated as sufficient. The sensitivity analysis found even greater differences in agreement with the hypothesis; therefore, the level of evidence was rated as strong.
Responsiveness
Criterion Approach
Responsiveness regarding comparisons with a gold standard or other knee JPS test over time was not examined in any study.
Construct Approach Among Other Outcome Measurements
One study analyzed correlations between a passive-active knee JPS test and somatosensory evoked potentials for 2 ACLR groups over time, 77 but this received an RoB rating of inadequate (Appendix Table A4, available online). Thus, the quality of responsiveness among other outcome measurements for knee JPS tests among individuals with ACL injury was not estimable owing to an unknown level of evidence.
Construct Approach Among Subgroups
Responsiveness among subgroups was evaluated in 18 comparisons across 10 studies f (Appendix Table A8, available online). Eight of these studies compared change in knee JPS over time among ACL-injured groups that received different interventions 6,9,23,38,68,98,106,113 ; 1 compared change between male and female patients with ACLR 3 ; and 1 compared change in knee JPS after one 36-minute exercise protocol between an ACLR group and a control group. 42 All multiple comparisons within studies received the same RoB rating: adequate for 1 study, 38 doubtful for 3 studies, 6,9,42 and inadequate for 6 studies 3,23,68,98,106,113 (Appendix Table A4, available online). A meta-analysis was precluded because data were missing from the relevant studies. Qualitatively, none of the findings from the studies rated as having a doubtful or adequate RoB agreed with the hypothesis that the experimental ACL group would show significantly greater improvements in knee JPS as compared with the subgroups. The quality of the PMP responsiveness among subgroups for knee JPS tests among individuals with ACL injury was therefore estimated as insufficient, and the level of evidence was rated moderate.
Construct Approach Before and After Intervention
Responsiveness of knee JPS tests to the effects of interventions for ACL-injured knees was assessed for 64 before-versus-after intervention comparisons across 22 studies g (Appendix Table A9, available online). All multiple within-study comparisons achieved the same RoB ratings: very good for 1, 76 adequate for 1, 79 doubtful for 11, h and inadequate for 9 studies i (Appendix Table A4, available online). A meta-analysis (12 comparisons across 6 studies 15,38,71,79,108,113 ) found no statistically significant differences in JPS error for ACL-injured knees after interventions (Figure 14) (MD, 0.67°; 95% CI, –0.46 to 1.81; P = .25; I 2 = 89%). A sensitivity analysis and a funnel plot with trim-and-fill analysis were precluded because the previously stated criteria were not met. Thus, the quality of responsiveness to intervention for knee JPS tests was rated insufficient. The level of evidence for these findings was rated moderate owing to the studies in the meta-analysis consisting of only 1 study with an RoB rating of adequate and the remaining 11 having an RoB rating of doubtful.

Meta-analysis comparing knee joint position sense absolute error group means in degrees of flexion between baseline (preintervention) and postintervention assessments (responsiveness to intervention) among anterior cruciate ligament–injured knees (treated with or without using reconstruction). A random effects model with mean difference was used. Subgroups are shown per test procedure. IV, inverse variance; TA, target angle.
Discussion
The purpose of this systematic review was to substantiate the evidence for the PMPs of knee JPS tests targeting individuals with ACL injury. The main findings based on meta-analyses were that ACL-injured knees produced significantly greater AEs for knee JPS tests as compared with the knees of asymptomatic controls (known-groups validity) as well as the contralateral healthy knees of the same individuals (discriminative validity). Thus, the quality of these properties was rated as sufficient, and the level of evidence for both was rated as strong. However, a meta-analysis for responsiveness to interventions did not show statistically significant results. As a result, the quality of this property was rated as insufficient, and the level of evidence was rated moderate, as was responsiveness in comparison with subgroups based on a qualitative synthesis. Caution should nonetheless be taken with these findings, as the presence of statistical heterogeneity in the majority of meta-analyses and publication bias may have affected the results. Reliability and associated measurement error of an active-active JPS test procedure for an intrasession design were the only properties to show a strong level of evidence for the qualitative syntheses, but this was based on just 1 study, the findings of which indicated insufficient and indeterminate quality for each property, respectively. 16 The quality of the remaining PMPs—reliability and measurement error for test-retest design, criterion validity, responsiveness from a criterion approach, and responsiveness in comparison with other outcome measures—could not be estimated because of an unknown level of evidence.
Reliability and measurement error were investigated in only 4 studies. The 3 studies that evaluated test-retest reliability 6,62,68 found high reliability, but all had an RoB rating of inadequate; however, the 1 study with an intrasession design 16 received an RoB rating of very good but indicated poor intrasession reliability. The low intrasession intraclass correlation coefficient of 0.06 and relatively large accompanying SEM of 2.7° indicated large within-patient variability among trials within the same session. These findings support calculating a mean value from multiple trials to avoid erroneous data. A previous study of knee JPS tests among individuals with patellofemoral pain syndrome determined that 5 trials were required for stable estimates for active procedures, whereas 6 trials were required for a passive knee JPS test. 96 A previous systematic review investigating the reliability of knee JPS tests using pathologic and asymptomatic cases found mixed evidence from 18 studies, largely dependent on the type of test methods. 100 The authors cited a lack of studies investigating reliability of the test among pathologic populations such as those with ACL injury. Thus, studies with a low RoB are required to establish the quality of reliability and measurement error for knee JPS tests among individuals with ACL injury and to improve the level of evidence.
Criterion (concurrent) validity was examined in only 1 study 30 with an RoB rating of inadequate, highlighting the need for further research in this area. This is of interest given the differences in results seen in the current review for the subgroup analyses of known-groups validity (see Figure 2), which showed mixed results for different test procedures. As there is no gold standard available to compare JPS tests, the criterion validity relating to the gold standard remains uncertain; however, additional studies are warranted on concurrent and predictive validity of JPS tests in individuals with an ACL injury.
For convergent validity, knee JPS test procedures were compared with many other diverse outcome measures, such as self-reported satisfaction and biomechanical measures of gait, making it difficult to draw conclusions regarding this PMP. However, >90% of findings did not find a correlation with the specific knee JPS tests and their comparator outcome measures, indicating a lack of correlation with at least those tested in this review. Thus, further studies are required to provide evidence for the convergent validity of knee JPS tests targeting individuals with ACL injury.
Our results for known-groups validity are in line with 1 previous meta-analysis 87 but in contrast to a systematic review without meta-analysis, 73 finding that ACL-injured knees produced significantly greater AE (MD, 0.70°) (see Figure 2) as compared with asymptomatic controls, regardless of whether ACLD and ACLR groups were combined or evaluated separately. In addition, our sensitivity analysis, which was limited to studies with an adequate or very good rating for RoB, showed even greater differences in errors (MD, 2.97°) (see Figure 3). However, subgroup analyses indicated that these results may depend on the test procedure, with only the knee JPS tests involving passive-passive test procedures producing statistically significant results; yet, passive-active (P = .06) and active-active (P = .05) procedures showed a trend toward statistical significance. It is possible that active procedures may facilitate compensation for potential loss of proprioceptors (Ruffini nerve endings, Pacini receptors, and Golgi tendon organ–like endings) in the injured/reconstructed ligament by relying more on muscle spindles. Further studies with a low RoB (very good rating) are required to substantiate these findings.
Our results for discriminative validity were in agreement with 2 previous meta-analyses, 58,87 finding significantly greater knee JPS errors for ACL-injured knees than for the contralateral noninjured knees of the same individuals (MD, 0.67°) (see Figure 8). When analyzed separately, however, only ACLD knees (MD, 0.95°) (Figure 10), not ACLR knees, showed significantly greater errors. Sensitivity analyses (ie, studies with a very good or adequate RoB rating) did nevertheless reveal a statistically significant difference for the separate analysis of ACLR groups (MD, 1.36°) (Figure 13) as well as even greater differences for the combined analysis (MD, 1.55°) (Figure 9) and for ACLD groups (MD, 1.81°) (Figure 11). Similar to known-groups validity, active-active test procedures did not differentiate between knees, supporting the hypothesis of compensatory mechanisms during active movements.
Responsiveness as compared with a gold standard or other knee JPS test over time was not assessed in any study, and responsiveness versus other outcome measurement instruments was examined in only 1 study of inadequate quality. 77 Thus, these PMPs require further research to provide evidence for their quality. Despite responsiveness among subgroups being analyzed in 10 studies, a meta-analysis was not possible owing to the studies having an RoB rating of inadequate or a lack of available data. 3,6,9,23,38,42,68,98,106,113 Although a meta-analysis was performed for responsiveness to interventions, the lack of statistically significant differences suggests that the knee JPS test methods might not be sensitive enough to detect change over time among the ACL populations. However, differences among JPS tests, types of interventions, and study populations make it difficult to generalize conclusions from these findings. Additional research investigating the responsiveness of knee JPS tests targeting individuals with ACL injury is therefore required.
Limitations of this review should be acknowledged. Recommending specific knee JPS tests based on our results is difficult, given the many paradigms used for assessment and their often poorly reported methods and outcomes. Although we differentiated among tests by performing subgroup analyses based on test procedures, it would be of value to investigate the effects on outcome measures of other modifiable components, not least TA and movement direction. It should be noted that AE was the sole outcome measure considered in this review as it was by far the most commonly reported. However, constant and variable error can provide valuable information regarding JPS and may provide different results when compared with AE. Specifically, AE provides the absolute difference between the TA and reproduction angle without consideration for the direction of the error, whereas constant error provides a measure of systematic bias by considering the direction of the error (ie, whether the individual under- or overshoots the TA). In contrast, variable error indicates the variance of the errors regardless of the proximity to the TA and can be considered a measure of precision. 94 To increase the generalizability of our results, we included a range of ACL populations. We also differentiated between populations in our meta-analyses by performing separate analyses for ACLD and ACLR groups when appropriate. Nevertheless, ACL groups differed with regard to, for example, age, sex, time since injury, activity level, and body composition, as well as time since and type of surgery in the case of the ACLR groups. Further investigations focusing on the potential effects of these factors would be of clinical and scientific value.
Studies that had received an RoB rating of inadequate were precluded from qualitative and quantitative examinations of quality. This was done to provide a more accurate evaluation of the quality of each PMP as opposed to including studies regardless of their methodologic quality. For qualitative syntheses, however, a post hoc sensitivity analysis of studies with an RoB rating of inadequate showed little effect on the overall quality ratings of the respective PMPs and their levels of evidence. To assess RoB, we used the COSMIN RoB checklist 70 but adhered to alternative guidelines, as stated in our protocol. 8 The latest COSMIN guidelines (2018) now cautiously recommend the inclusion of studies with an RoB rating of inadequate in analysis syntheses, as long as their findings are in line with those of the studies with a better RoB rating; thus, future studies may consider whether this is appropriate.
The lack of standardized reporting of knee JPS methods among studies, as well as unclear or missing information, made compiling evidence difficult. For example, we provided specific starting angles and TAs whenever this was indicated; however, 26 tests used unspecific angles within ranges of motion, and 15 tests failed to cite 1 or both angles. Finally, statistical heterogeneity was present in the majority of meta-analyses in this systematic review; thus, according to our stated criteria, no funnel plots with trim-and-fill analyses were produced to identify and correct for potential publication bias. There is therefore a possibility that publication bias might have been present in our findings, and caution should be taken while interpreting the results. Nevertheless, we searched 8 databases between their inception and March 2020 and included as many published studies (in English) from peer-reviewed journals as available in this area.
Future studies implementing knee JPS tests should publish clear and detailed testing methods. Reporting of outcomes should include a minimum of group mean and SD for AE with correlation, change scores, or both when relevant and also for constant and variable error. In addition, to further differentiate among ACL populations, it may be pertinent to control for and report the following: time since injury, time to surgery in the case of individuals with ACLR, preinjury and current activity level, leg dominance, side of injury, other concomitant injuries, demographic factors (age and sex), and anthropometric factors (body height and mass).
Conclusion
This systematic review and meta-analysis identified specific gaps in knowledge and provided evidence that can help to guide future investigations. Meta-analyses indicated sufficient quality and a strong level of evidence for known-groups and discriminative validity of knee JPS tests, given the significantly greater AEs for ACL-injured knees as compared with asymptomatic controls and the asymptomatic contralateral knees of the same individuals. Furthermore, passive test procedures appeared to elucidate greater differences between groups than did active test procedures. However, responsiveness to intervention was rated insufficient with a moderate level of evidence, owing to a lack of statistically significant change in AE over time after various interventions and limited studies of low RoB, respectively. The remaining PMPs in this review—reliability, criterion validity (concurrent and predictive), convergent validity, and responsiveness (criterion approach and construct approach between other outcome measurements as well as subgroups)—were assessed only qualitatively and require more studies with a low RoB to increase their level of evidence to better evaluate their quality. Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211007878.
Supplemental Material
Supplemental Material, sj-docx-1-ojs-10.1177_23259671211007878 - Properties of Knee Joint Position Sense Tests for Anterior Cruciate Ligament Injury: A Systematic Review and Meta-analysis
Supplemental Material, sj-docx-1-ojs-10.1177_23259671211007878 for Properties of Knee Joint Position Sense Tests for Anterior Cruciate Ligament Injury: A Systematic Review and Meta-analysis by Andrew Strong, Ashokan Arumugam, Eva Tengman, Ulrik Röijezon and Charlotte K. Häger in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors thank Anna Cronström for her critical review of the manuscript.
Final revision submitted November 9, 2020; accepted January 1, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Swedish Research Council (grant 2017-00892); Region Västerbotten (grant ALF 7003575 VLL838421, strategic funding VLL-358901, project No. 7002795); the Swedish Research Council for Sports Science (grant CIF P2019-0068), Umeå School of Sport Science, Umeå University; and King Gustaf V and Queen Victoria’s Foundation of Freemasons 2019 (Dr Häger). The funders did not have any role in the study design. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.