
Abstract
Background:
There is much room for improvement and optimization of meniscal allograft survivorship.
Purpose:
To understand prognostic factors for survivorship using evidence-based selection criteria in order to identify patients who would best benefit from meniscal allograft transplant (MAT).
Study Design:
Systematic review; Level of evidence, 4.
Methods:
We conducted this systematic review to analyze prognostic factors for survivorship of MAT. The Cochrane Central Register, PubMed publisher, Embase.com, and Web of Science databases were searched through August 8, 2019. Included studies entailed patients of any age who received MAT with a reported association between prognostic factors and survivorship of the allograft. Two reviewers independently screened all titles and abstracts for eligibility, extracted the data, assessed the risk of bias using the Newcastle-Ottawa Scale, and performed a best-evidence synthesis.
Results:
The review included 18 studies with a total of 1920 patients. The mean follow-up time was 6.0 years (range, 2.1-11.2 years). A total of 20 prognostic factors were identified and shown to be associated with survivorship of MAT. Strong evidence was found that severe cartilage damage was associated with poor survivorship. Strong evidence was also found showing that sex, knee compartment, surgical side, concomitant anterior cruciate ligament (ACL) reconstruction, and concomitant osteotomy for malalignment had no effect on survivorship. Moderate evidence was found that body mass index (<36), tobacco use, and arthroscopic versus open procedure had no influence on survivorship. Conflicting evidence was found that older age and kissing cartilage lesions (lesions on both the femur and tibia vs on a single side) decreased survivorship.
Conclusion:
Severe cartilage damage decreases the survivorship of MAT. Concomitant ACL reconstruction and osteotomy showed no relationship to survivorship. Many determinants showed conflicting and limited evidence. Older age may be of interest and should be further studied.
Meniscal tears are common injuries in sports participants. Most meniscal tears are treated using partial meniscectomy or repair, with current trends toward repair for preservation of function. However, subtotal meniscectomy may be the only choice for large, complex, or chronic tears. It is well known that meniscal deficiency is a risk factor for osteoarthritis (OA) of the knee, with a 134-fold increase in the rate of total knee arthroplasty in the long term. 31
Management of a patient who has symptoms of meniscal deficiency can be difficult. For these often young and active patients, meniscal allograft transplant (MAT) is an effective intervention to partially restore the native biomechanical environment in the knee 25 and relieve symptoms. 26 MAT is performed relatively rarely (estimated 1/1,000,000 population) because of the strict indications for MAT and the limited availability of allografts. 10 Because long-term studies (>20-year follow-up) have reported satisfactory outcomes, MAT is no longer considered experimental. 8 However, whether MAT is chondroprotective and can prevent progression of OA remains elusive. 35
Given that young, active people comprise the population that most commonly experiences meniscal tears and may undergo MAT, it is important to understand survivorship of the allograft because of the potential to alter the progression and burden of OA. A recent systematic review found that 73.5% and 60.3% of meniscal allografts remained functional after 10 and 15 years, respectively. 26 Thus, it is important to identify factors that affect the survivorship of MAT and to determine whether these factors can be modified.
Careful patient selection is essential to achieve optimal clinical outcomes and long-term survivorship of the meniscal allograft. To predict graft survivorship, an evidence-based approach to understanding prognostic factors is essential. Factors of concern might include patient characteristics, concomitant procedures (chondral lesions and cartilage repair or regeneration, anterior cruciate ligament [ACL] reconstruction, and osteotomy), and surgical technique. To the best of our knowledge, no systematic review of prognostic factors for meniscal allograft survivorship has been conducted.
The purpose of this study was to review all available literature and identify prognostic factors for the survivorship of meniscal allograft. We hypothesized that the literature has reported some prognostic factors that predict MAT failure and that an evidence-based systematic review may be helpful in developing better strategies to identify patients who would best benefit from MAT.
Methods
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement, 24 and the study protocol was registered with PROSPERO (CRD42020145026).
Search Strategy
Four online databases (Cochrane Central Register, PubMed publisher, Embase.com, and Web of Science) were independently searched by 2 reviewers (D.Y.W. and Y.Z.L.) on August 8, 2019. The search string was “menisc* AND (transplant* OR allograft* OR homograft*).” The article types included in the search were randomized controlled trials, prospective or retrospective cohort studies, and case series. There was no restriction regarding date of publication.
Inclusion criteria for studies were as follows: (1) entailed patients of any age with a symptomatic, meniscal-deficient compartment of the knee who received MAT; (2) described a correlation or association between 1 or more prognostic factors and meniscal allograft survivorship; (3) entailed no follow-up time restriction because allograft failure could happen any time after transplant; and (4) written in English.
Exclusion criteria were as follows: (1) review articles, (2) nonclinical studies (biomechanical and cadaveric studies, surgical technique notes, and basic science studies), (3) studies that did not report clinical outcomes, (4) studies that included overlapping cohorts (in such conditions, repeated prognostic factors from the largest cohort were included), and (5) studies with a published abstract only.
Study Screening
Two reviewers (D.Y.W. and B.Z.) independently screened all titles and abstracts for eligibility. Disagreements were discussed and resolved by consensus. If consensus could not be reached, a third reviewer was consulted to decide whether the study should be included. Reference lists of the included articles were screened for potential inclusion of additional studies.
Risk of Bias
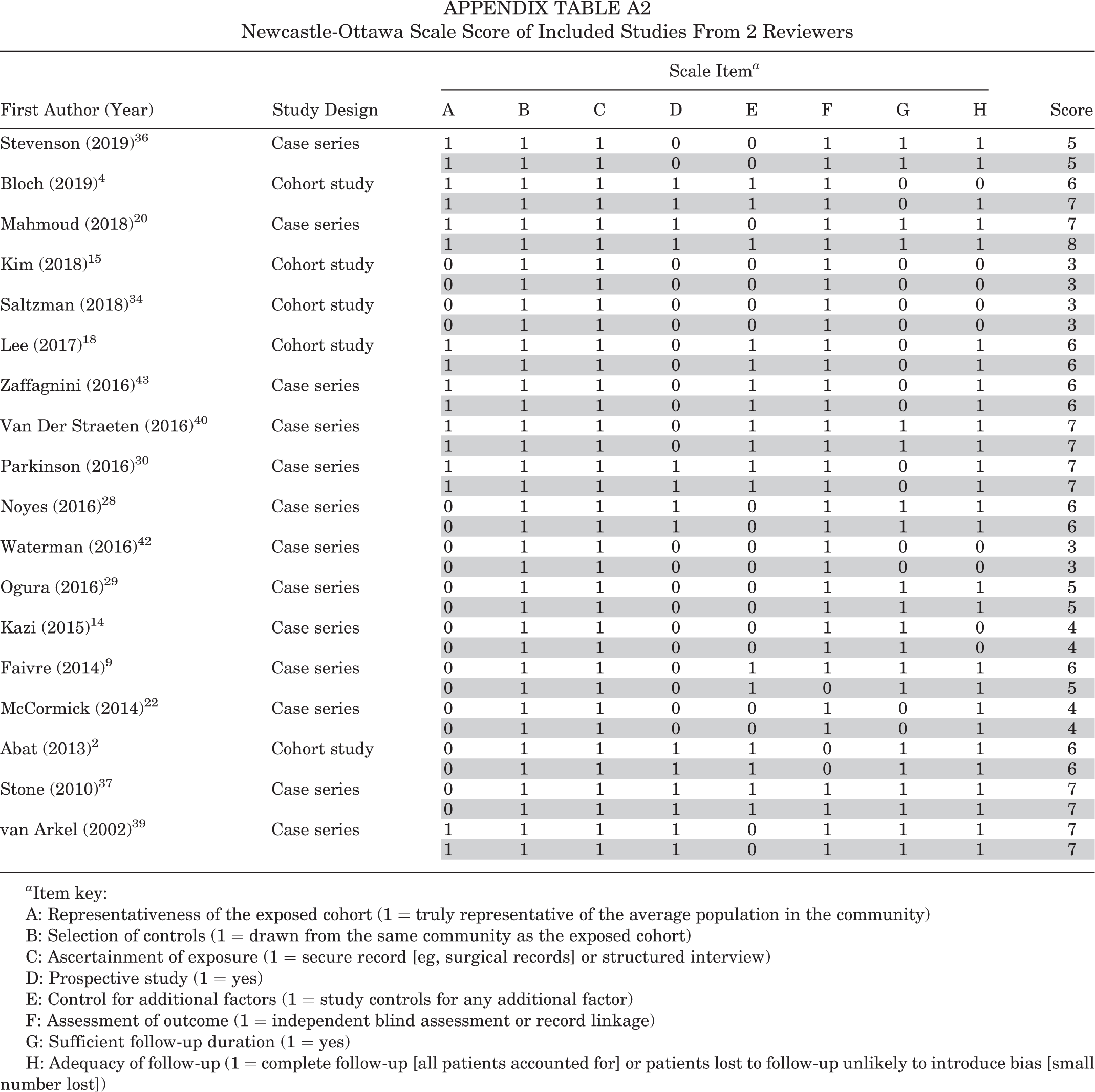
Two reviewers (Z.Y.L. and B.Z.) independently assessed the potential risk of bias using the Newcastle-Ottawa Scale (NOS). The NOS list involves 8 questions that assess the bias of (1) the selection of the study groups, (2) the comparability of the groups, and (3) the ascertainment of either the exposure or the outcomes of interest. Each study was given a score (maximum of 8 points). In particular, a study was scored as having sufficient duration of follow-up if the mean follow-up time reached 5 years. A study was scored as having adequate follow-up if the rate of loss to follow-up was <20% in 2 years. A score of 0 to 3 points indicated a study with a high risk of bias (HR), 4 to 6 points indicated moderate risk of bias (MR), and 7 to 8 points indicated low risk of bias (LR).
Data Extraction
Data from the included studies were initially extracted by 1 reviewer (Y.Z.L.) and subsequently reviewed by a second reviewer (D.W.Y.). Extracted data included author and year, study design, level of evidence, follow-up time, patient characteristics (age, sex, body mass index [BMI], left or right knee, medial or lateral meniscus, tobacco use, previous knee surgeries), concomitant procedures (chondral lesions and cartilage repair or regeneration, ACL reconstruction, and osteotomy), surgery details (surgical technique, graft type), survivorship rate, allograft failure criteria, and complications.
Best-Evidence Synthesis
A best-evidence synthesis was performed using the algorithm developed by van Tulder et al, 41 which incorporates both methodologic quality of included studies and statistical outcomes. Strong evidence was provided by ≥2 LR studies and by generally consistent findings within all studies (≥75% of the studies reported consistent findings), moderate evidence was provided by 1 LR study and ≥2 MR or HR studies or by ≥2 MR or HR studies and by generally consistent findings in all studies (≥75%), limited evidence was provided by ≥1 MR or HR studies or 1 LR study and by generally consistent findings (≥75%), conflicting evidence was provided by conflicting findings (<75% of the studies reported consistent findings), and no evidence was provided when no studies could be found.
Results
Search Strategy
We identified 5958 potentially relevant studies, and after removing duplicates, 3601 remained. After screening of the title and abstract, 179 studies remained to be further assessed (Figure 1). A total of 18 studies met the inclusion criteria and were included in this systematic review. # Appendix Table A1 provides a summary of the studies included.

Flow diagram of identification, screening, and selection of studies. MAT, meniscal allograft transplant.
Characteristics of the Included Studies
We included 3 prospective cohort studies, 3 retrospective cohort studies, and 12 case series.# The characteristics and main findings of all of the included studies are summarized in Appendix Table A1. We excluded the repeated cohort, leaving the total number of included patients as 1920. The mean follow-up time was 6.0 years (range, 2.1-11.2 years). The 5-year survival rate ranged from 75% to 96% and the 10-year survival rate from 45% to 89.4%.
Risk of Bias of Included Studies
Of the 18 included studies, 6 studies 4,20,30,37,39,40 were rated as LR, 9 studies as MR, 2,9,14,18,22,28,29,36,43 and 3 studies as HR. 15,34,42 The agreement between the 2 reviewers was 98%. Quality assessment scores on the NOS for included studies are presented in Appendix Table A2.
Heterogeneity
Most studies included consecutive patients receiving MAT. ** Most studies excluded patients with advanced arthrosis, diffuse cartilage loss, and subchondral bone exposure. 2,15,22,28,29,30,34,36 A total of 3 studies 15,22,34 excluded patients with mild or severe cartilage damage, 1 study 2 excluded patients with malalignment, 1 study 28 excluded patients with malalignment and severe cartilage damage, 1 study 42 included only military patients, 1 study 29 included only patients with severe cartilage damage, and 1 study 9 included only patients with lateral MAT. Most studies reported MAT patients in their 20s and 30s. †† One study 37 included older patients, with an average age of 46.9 years. The allograft preservation method and surgical fixation technique varied among studies. The definition of MAT failure was mainly conversion to knee arthroplasty and removal of the allograft.# Several studies also considered low patient-reported outcome scores (Lysholm score <65) as indicating allograft failure (Appendix Table A1). 17,36,39,43
Considerable heterogeneity of the studies precluded pooling data and conducting a meta-analysis. Hence, a qualitative analysis was performed, according to the principle of best-evidence synthesis.
Prognostic Factors
A total of 20 prognostic factors were identified and shown to be associated with survivorship of meniscal allograft.# Table 1 shows the strength of evidence for prognostic factors included in best-evidence synthesis.
Influence of Determinants on Survivorship of Meniscal Allograft a

a Data are presented as the number of studies for a given risk of bias and the associated reference numbers. BioCleanse manufacturer, Regeneration Technology Inc. ACL, anterior cruciate ligament; HR, high risk of bias; LR, low risk of bias; MR, moderate risk of bias.
Age at MAT
We found conflicting evidence that age affected survivorship of meniscal allograft. A total of 3 studies, 18,37,40 including 2 LR studies 37,40 and 1 MR study, 18 reported that older age at the time of MAT decreased survivorship. A further 4 studies 20,28,29,42 showed no association. Most studies reported outcomes of young and middle-aged patients††; however, 1 study 37 reported that 46.1% of patients were aged >50 years.
Patient Sex
Strong evidence was found that sex did not affect survivorship of the meniscal allograft. The 7 studies 18,20,29,30,37,40,42 that assessed this factor reported no statistically significant association between sex and survivorship.
Body Mass Index
There was moderate evidence that BMI did not affect survivorship of the meniscal allograft. The 2 studies that assessed BMI of the included patients reported values of 24.9 (range, 16.9-35.7) 40 and 24.2 ± 3.7. 18 Both studies reported no statistically significant association between BMI and survivorship in multivariate analysis, suggesting that BMI might not be an independent factor.
Side Affected
We found strong evidence that right or left knee does not affect survivorship of meniscal allograft. The 3 studies 15,20,40 that assessed this factor reported no statistically significant association between side and survivorship.
Knee Compartment
There was strong evidence that knee compartment does not affect survivorship of meniscal allograft. One LR study 39 reported that a medial MAT with ACL deficiency was associated with an increased risk for meniscal allograft failure. Another study reported that the hazard ratio of lateral (vs medial) meniscal allograft was 0.24 (95% confidence interval, 0.07-0.84) in a Cox regression model. 30 A total of 7 studies, 18,20,22,28,37,40,43 including 3 LR studies, 20,37,40 reported no statistically significant association between knee compartment and survivorship.
Tobacco Use
We noted moderate evidence that tobacco use does not affect survivorship. Two studies 40,42 found no association between tobacco use and survivorship.
Time from Previous Meniscectomy
Limited evidence was available regarding whether time from previous meniscectomy would affect survivorship of meniscal allograft. One study 18 reported that time from previous meniscectomy to MAT did not affect the survivorship.
Severity of Cartilage Damage
Strong evidence was found indicating that severity of cartilage damage significantly affected survivorship of meniscal allograft. A total of 4 studies, 4,18,20,40 including 3 LR studies, 4,20,40 reported that severe cartilage damage was associated with lower survivorship compared with mild damage. Bloch et al 4 found that the failure rate for mild lesions (International Cartilage Regeneration & Joint Preservation Society [ICRS] grade ≤3A) was 4.6%, whereas in patients with more severe lesions (ICRS grade >3B-C on a single side), the failure rate was 12.5% at 3-year follow-up. Mahmoud et al 20 reported that 100% of patients with Outerbridge grade 0 to II had intact MAT at an average follow-up of 10.6 years, whereas those with an Outerbridge grade III or IV had 74.2% survival at an average follow-up of 7.1 years. Van Der Straeten et al 40 reported that survivorship was 43% at 24 years in patients with Outerbridge grade <III and 6.6% in patients with Outerbridge grade ≥III, with an odds ratio of 3.7.
One study 28 compared patients with a cartilage damage score of 2B and 3 on the Cincinnati knee rating system against those without cartilage damage and found no significant difference in survivorship. The same study reported that osteochondral allograft transfer was associated with lower survivorship compared with no osteochondral allograft transfer.
One study 37 reported no difference in survivorship between patients with advanced osteochondral lesions (Outerbridge grade III vs IV). This study was excluded from best-evidence synthesis because of significant heterogeneity of patient selection.
Cartilage Kissing Lesions
Conflicting evidence was found regarding whether full chondral lesions on both sides of a compartment (kissing lesions) had lower survivorship of meniscal allograft than did a single lesion. Two studies, 4,18 including 1 LR study, 4 reported that full chondral lesions on both sides increased the risk for meniscal transplant failure compared with a full chondral lesion on a single side. One MR study 29 showed no association.
Size of Cartilage Lesion
There was limited evidence that the size of a cartilage lesion did not affect the risk for meniscal transplant failure. The study that assessed this factor found no association. 29 The study reported that a chondral defect size >6 cm2 did not decrease survivorship compared with a defect <6 cm2 in the 18 patients undergoing MAT with full-thickness chondral defects who received autologous chondrocyte implantation.
Concomitant Osteotomy
Strong evidence was found that concomitant osteotomies to correct malalignment did not decrease survivorship of meniscal allograft compared with normal alignment. A total of 6 studies, 4,14,18,29,37,42 including 2 LR studies, 4,37 reported that osteotomy did not affect outcomes. One LR study 40 showed that osteotomy was associated with lower survivorship.
Concomitant ACL Reconstruction
We noted strong evidence that ACL reconstruction did not affect survivorship of meniscal allograft. Two LR studies 4,40 reported that ACL reconstruction had no association with survivorship at a follow-up of 3 to 6 years. Another study 42 reported that reconstruction of the ACL or posterior cruciate ligament increased the risk of failure; this was not included in the best-evidence synthesis because the effects of ACL and posterior cruciate ligament reconstruction were analyzed together.
Tibial Subchondral Bone Marrow Lesion
There was limited evidence that tibial subchondral bone marrow lesions affected survivorship of meniscal allograft. One HR study 34 reported that tibial subchondral bone marrow lesion did not affect survivorship.
Arthroscopic Versus Open Procedure
We found moderate evidence that arthroscopic or open surgery did not affect survivorship of meniscal allograft. Two studies, 9,40 including 1 LR study, 40 reported no statistically significant association between arthroscopy and survivorship.
Surgical Technique and Skills
Limited evidence was found regarding whether implantation technique and surgeon skills were associated with survivorship. Factors included nonanatomic versus anatomic horn position placement, suture fixation of soft tissue only versus bony plug fixation, and low-volume surgeons. 2,15,42
Graft Factors
Limited evidence was found that graft factors such as allograft sizing (undersizing vs matched sizing vs oversizing), 36 sterilization technique (none vs BioCleanse; RTI Surgical), 29 and graft preservation method (fresh-frozen vs viable allograft) 40 affected outcomes.
Discussion
This systematic review aimed to summarize the evidence concerning prognostic factors for meniscal allograft survivorship. Despite the significant heterogeneity in study design, patient population, and outcome definitions, several prognostic factors were found to be predictive of MAT survivorship. There was strong evidence that severe cartilage damage was associated with poor survivorship. Sex, BMI (<36), knee compartment, surgical side, tobacco use, concomitant ACL reconstruction, osteotomy, and arthroscopic versus open surgery were not found to influence survivorship. We found conflicting evidence that older age (perhaps age >35 years) or full-thickness chondral kissing lesions may decrease MAT survivorship. The time from previous meniscectomy, size of the cartilage lesion, presence of a tibial subchondral bone marrow lesion, use of suture fixation or bony plug technique, surgeon skill, and graft preservation method had limited evidence.
The most important finding of this study was that severe cartilage lesions significantly decreased graft survivorship. Full-thickness chondral lesions had at least 3 times higher rate of meniscal allograft failure than did partial-thickness chondral lesions, although the cartilage damage was repaired using different strategies at the time of MAT. Surgeons should consider whether it is cost-effective to perform MAT on older patients with severe full-thickness chondral damage because those patients would have a higher failure rate. For patients with mild to moderate cartilage damage, attention should be paid to protection of articular cartilage in order to prolong meniscal allograft survivorship.
Besides the degree of the chondral lesions, the location and the size of the chondral lesions were of concern. Diffuse cartilage loss and narrowed joint space have been considered absolute contraindications to MAT. Some studies 20,28 excluded patients with kissing lesions. Two studies 4,18 reported that full chondral lesions on both sides increased the risk for meniscal transplant failure compared with a full chondral lesion on single side. However, the effect of the chondral lesion size on survivorship is rarely reported. One case series, 29 involving 18 patients undergoing MAT with full-thickness chondral defects who received autologous chondrocyte implantation reported that a chondral defect size >6 cm2 did not decrease survivorship compared with a chondral defect <6 cm2. This study also reported that kissing lesions did not influence survivorship. Because of the patient selection method and sample size, it was hard to draw a meaningful conclusion from this case series.
Biochemical and biomechanical changes occur just after meniscectomy, and cartilage degeneration happens gradually. 1,21 There is no clear, strong evidence to support the use of MAT to halt the progression of OA. 35 However, radiographic progression of arthrosis is reduced in knees after MAT compared with meniscus-deficient knees. 17 Two studies 33,43 found that delayed implantation after meniscectomy was related to worse clinical outcomes over time. Zaffagnini et al 43 reported that a longer period of time between the first meniscectomy and MAT was associated with an increased postoperative visual analog scale score for pain (4.1 points every 10 years; P = .0147). Another study 12 reported that immediate prophylactic MAT led to more satisfactory subjective results, less joint degeneration, and lower muscle strength deficits when compared with delayed MAT with a mean time of 35 months. Further studies examining the long-term chondral protection provided by MAT and the superiority of immediate MAT are needed.
We found strong agreement that patients with ACL deficiency and an absent medial meniscus might benefit from MAT at the time of ACL reconstruction to improve joint stability and prevent failure of either component. 10 The ACL and the medial meniscus are important stabilizers of the knee and directly affect each other. Therefore, a meniscal graft is expected to protect the ACL and vice versa. 10 In a meta-analysis and systematic review, Lee et al 19 found no significant difference in clinical outcomes between isolated MAT and combined MAT and ACL reconstruction. Our systematic review found strong evidence from 2 LR studies that ACL reconstruction did not decrease the survivorship of meniscal allograft in the midterm. 4,40 However, it is well-known that ACL reconstruction is not an adequate intervention to prevent posttraumatic knee OA. It has been reported that 51.6% of patients had developed OA at 20 years after surgery. 6 Thus, the long-term influence of ACL reconstruction on the survivorship of meniscal allograft requires further investigation.
Another key finding of the current systematic review was that strong evidence was found suggesting that concomitant osteotomy did not decrease the survivorship of MAT compared with isolated MAT. All of the studies included in this review corrected malalignment during MAT, and the majority of them reported no significant difference between isolated MAT and MAT combined with osteotomy. 4,14,18,29,37,42 The inclusion criteria for MAT were relatively strict regarding chondral status, suggesting that the corrected alignment achieves similar outcomes to normal alignment. Most studies lacked a subgroup analysis of malalignment type (varus or valgus), did not quantify severity of malalignment, and did not match varus or valgus type to the medial or lateral MAT. 4,14,18,29,42 Because the malalignment type is associated with the biomechanics of the knee compartment, further studies are needed to determine whether malalignment type is truly associated with failure of the specific side of the meniscus.
In the current systematic review, conflicting evidence was found for the predictive value of age on survivorship of meniscal allograft. We noted considerable methodologic heterogeneity among the studies. We found that 5 studies 20,28,29,37,40 considered age as a binary variable with different cutoff points, whereas 3 studies 15,18,42 considered age as a continuous variable. A total of 3 studies 18,30,40 controlled confounding factors and concluded that older age had a negative effect on MAT survivorship, whereas 4 studies 20,28,29,42 reported no association between age and MAT failure, none of which excluded confounding factors. Although the conclusions were contradictory among the studies, data suggest that age is an important issue and should be considered: all studies demonstrated an odds ratio or hazard ratio >1, except for 1 study 29 with insufficient data. Noyes and Barber-Westin 28 estimated that patients aged >30 years at the time of surgery were 1.08 times more likely to experience failure at 5-year follow-up; 1.02 times, at 10-year follow-up; and 2.07 times, at 15-year follow-up (not statistically significant). Mahmoud et al 20 suggested that patients aged >35 years at the time of surgery had a 1.23 times higher failure rate compared with those aged <35 years, at a mean follow-up of 8.6 years (not statistically significant). Van der Straeten et al 40 reported that patients aged ≥35 years had a 2.3 times higher failure rate compared with patients aged <35 years (P = 0017). Stone et al 37 reported that patients aged >50 years were 2.90 times more likely to experience failure compared with those aged <50 years, with the mean follow-up of 5.8 years. Lee et al 18 estimated that the failure rate increased by 2.48 times for every 10 years of age. We roughly estimated that patients aged >35 years had around 2 times higher failure rate than did those aged <35 years.
Age is related to the development of chondral lesions. However, 3 studies 18,37,40 demonstrated that age was an independent factor for meniscal allograft survivorship in a multivariate analysis with correction of the cartilage effect. Given various factors, from cell viability to metabolic activity and degeneration, 11,32,38 survivorship of the allograft in older patients would not be expected to be comparable with that in younger patients. In the 18 included studies, only 1 study 37 reported allograft survivorship of middle-aged and older patients. In that study, the mean age was 46.9 years (range, 14.1-73.2 years), and 46.1% of patients were aged >50 years. The risk of allograft failure increased by 1.061 (95% confidence interval, 1.007-1.117) per year. 37 According to a Cox proportional hazards model, patients aged >50 years were 2.90 times more likely to experience failure compared with those aged <50 years. 37 Older patients usually do not demand the same high levels of sporting functionality as do younger patients. Often, meniscectomy achieves no better outcomes compared with physical therapy alone for symptomatic meniscal tears in patients with mild to moderate OA. 13 Whether it is necessary or cost-effective to perform MAT in patients aged >50 should be further studied.
Other patient characteristics, including sex, BMI, side affected, knee compartment, and tobacco use, showed moderate or strong evidence that the given factor did not influence the survivorship of the meniscal allograft. The BMIs of the reported patients were a mean of 24.9 (range, 16.9-35.7) 40 and a mean ± standard deviation of 24.2 ± 3.7, 18 far from the criteria of obese. Obesity is definitely related to knee OA 16 and would theoretically decrease the survivorship of the meniscal allograft.
Surgical and graft factors were identified as prognostic factors, but we could not find enough materials to draw a strong conclusion. We found that whether MAT was open or arthroscopic did not affect survivorship. Arthroscopic techniques would theoretically minimize soft tissue damage, scarring, and the risk of infection while allowing direct visualization to assess cartilage lesions with greater accuracy, 9 whereas open procedures may allow for more anatomic positioning or better fixation. Faivre et al 9 reported similar survivorship and clinical outcomes for open soft tissue fixation and arthroscopic bone tunnel groups, but the arthroscopic group had a higher extrusion rate. Merkely et al 23 reported that open bridge-in-slot techniques had a lower extrusion rate than arthroscopic technique, whereas De Coninck et al 7 found less extrusion with arthroscopic surgery compared with open surgery. The extrusion rate might be different among the techniques, including soft tissue fixation and bone fixation. Cadaveric studies have reported that bone block fixation achieved better load transmission over soft tissue fixation and transosseous fixation. 3,5 However, the clinical significance of meniscal extrusion after MAT remains controversial. 27 Typically, with native meniscus, extrusion means that the meniscus does not function; however, extrusion usually occurs in the meniscal body but not at the root. As a result, function of the meniscus might not be completely lost. We found limited evidence that the surgical technique used to fix a meniscal allograft does not affect survivorship. Further investigation is needed to determine which technique achieves superior clinical outcomes in term of allograft survivorship.
Limitations
To the best of our knowledge, this is the first systematic review concentrating specifically on the predictors of meniscal allograft survivorship. The first, and major, limitation is that we could provide only rough estimations of the effect sizes of the prognostic factors. This was because of substantial heterogeneity in patient selection, surgical technique, definition of subgroups, and definition of failure in the included studies. Many prognostic factors were reported by only a small portion of the included studies. The effect of the prognostic factors was poorly reported in many studies, which provided only P values or a descriptive summary without any data. Thus, a meta-analysis could not be performed.
Second, none of the studies included were randomized controlled trials: 3 were prospective cohort studies, 2,4,30 3 were retrospective cohort studies, 15,18,34 and 12 were case series. ‡‡ A prospective controlled study design is the best way to determine prognostic factors. Retrospective studies were useful to some degree and thus were included in the analysis. Given the lack of studies investigating some of the prognostic factors, we had to include case series to allow a more comprehensive assessment of this topic, which definitely diminished the strength of the conclusion. The influence of confounders was not corrected in 10 studies. §§ Given the prevalence and strong effect on survivorship of cartilage damage, the reliability of the studies would be weakened.
Third, some of the prognostic factors we identified were inadequately reported, including time from previous meniscectomy, size of chondral lesion, presence of a tibial subchondral bone marrow lesion, and surgical and graft factors. Thus, we cannot draw conclusions regarding these factors, which limits the strength of this systematic review.
Fourth, follow-up time ranged from 2.14 to 11.2 years. The mean follow-up time in 8 studies was <5 years. 4,15,18,22,30,34,42,43 We analyzed differences in prognostic factors among short-, mid-, and long-term studies but could not find meaningful results. The effect of some factors (eg, age) may be more significant in long-term follow-up or as patients reach the age of 50 years. Thus, the effect of the prognostic factors on long-term survivorship cannot be fully revealed.
Conclusion
Severe cartilage damage decreased the survivorship of MAT. Concomitant ACL reconstruction and osteotomy for malalignment had no relationship to survivorship. Many determinants showed conflicting and limited evidence. Older age may be of interest and should be further studied.
Footnotes
Notes
Final revision submitted November 6, 2020; accepted January 2, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the China National Scientific Foundation (grants 31670982, 51920105006, 81630056) and the National Key Research and Development Program of China (grant 2018 YFF0301100). C.A.L. has received honoraria from Vericel and Fidia Pharma USA; educational payments from Sequoia Surgical and Arthrex; consulting fees from KCI USA; and hospitality payments from Smith & Nephew, Aesculap Biologics, and RTI Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Newcastle-Ottawa Scale Score of Included Studies From 2 Reviewers
| First Author (Year) | Study Design | Scale Item a | Score | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| A | B | C | D | E | F | G | H | |||
| Stevenson (2019) 36 | Case series | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 5 |
| 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 5 | ||
| Bloch (2019) 4 | Cohort study | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 6 |
| 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 7 | ||
| Mahmoud (2018) 20 | Case series | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | ||
| Kim (2018) 15 | Cohort study | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 3 |
| 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 3 | ||
| Saltzman (2018) 34 | Cohort study | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 3 |
| 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 3 | ||
| Lee (2017) 18 | Cohort study | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 6 |
| 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 6 | ||
| Zaffagnini (2016) 43 | Case series | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 6 |
| 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 6 | ||
| Van Der Straeten (2016) 40 | Case series | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 | ||
| Parkinson (2016) 30 | Case series | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 7 |
| 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 7 | ||
| Noyes (2016) 28 | Case series | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 6 |
| 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 6 | ||
| Waterman (2016) 42 | Case series | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 3 |
| 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 3 | ||
| Ogura (2016) 29 | Case series | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 5 |
| 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 5 | ||
| Kazi (2015) 14 | Case series | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 4 |
| 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 4 | ||
| Faivre (2014) 9 | Case series | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 6 |
| 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 5 | ||
| McCormick (2014) 22 | Case series | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 4 |
| 0 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 4 | ||
| Abat (2013) 2 | Cohort study | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 6 |
| 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 6 | ||
| Stone (2010) 37 | Case series | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||
| van Arkel (2002) 39 | Case series | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 | ||
a Item key:
A: Representativeness of the exposed cohort (1 = truly representative of the average population in the community)
B: Selection of controls (1 = drawn from the same community as the exposed cohort)
C: Ascertainment of exposure (1 = secure record [eg, surgical records] or structured interview)
D: Prospective study (1 = yes)
E: Control for additional factors (1 = study controls for any additional factor)
F: Assessment of outcome (1 = independent blind assessment or record linkage)
G: Sufficient follow-up duration (1 = yes)
H: Adequacy of follow-up (1 = complete follow-up [all patients accounted for] or patients lost to follow-up unlikely to introduce bias [small number lost])