
Abstract
Background:
Meniscal allograft transplantation (MAT) is a viable option for patients experiencing unicompartmental knee pain after total or subtotal meniscectomy. Nonetheless, caution is recommended when suggesting this procedure in the presence of knee osteoarthritis (OA) because of the higher risk of poor survival and outcomes.
Purpose/Hypothesis:
The purpose was to document the long-term survival of MAT performed as a salvage procedure in patients with knee OA. The hypothesis was that MAT would significantly reduce pain and increase the function of the affected joint at a long-term follow-up compared with the preoperative condition, with a low number of failures and knee replacement surgeries.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 47 patients (37 men and 10 women) with symptomatic knee OA (Kellgren-Lawrence grades 2 or 3) treated with MAT were evaluated at baseline, 5 years, and a minimum 10-year final follow-up (11.1 ± 1 years) using the Lysholm score, the visual analog scale for pain, the Knee injury and Osteoarthritis Outcome Score subscales, and the Tegner score. A total of 44 patients had undergone previous surgeries. Patient satisfaction, revision surgeries, and failures were also recorded.
Results:
A statistically significant improvement was observed in all clinical scores from the baseline assessment to the final follow-up. The Lysholm score improved significantly from 46.4 ± 17.2 at the preoperative assessment to 77.7 ± 20.4 at the intermediate follow-up (P < .001), with a significant decrease at the final follow-up (71 ± 23.3; P = .018). A similar trend was reported for the visual analog scale scale for pain, Knee injury and Osteoarthritis Outcome Score, and Tegner score, with no complete recovery to the previous sports activity level. A total of 33 patients required concurrent procedures, such as anterior cruciate ligament reconstructions, osteotomies, and cartilage procedures. Five patients underwent reoperation and were considered surgical failures, while 15 patients presented a clinical condition of <65 of the Lysholm score and were considered clinical failures. Among these, 4 patients were considered both surgical and clinical failures.
Conclusion:
MAT surgery has proven to be a valid option for improving pain and function even in OA joints (Kellgren-Lawrence grades 2 or 3), yielding satisfactory results despite a worsening clinical outcome in the long-term follow-up. Therefore, based on the data from this study, orthopaedic surgeons may consider recommending MAT as a salvage procedure even in knees affected by early to moderate OA, while advising patients that the need for combined interventions could potentially reduce graft survival.
The meniscal fibrocartilage performs an essential function in preserving the biomechanical and biological environment of the knee joint. The reason for this important role lies in the ability to transmit and distribute the load in the knee, 53 representing a secondary stabilizer to the antero-posterior translation of the joint in unstable knees.27,51 Indeed, numerous studies have shown that meniscal deficiency due to traumatic injury or tissue loss after meniscectomy can persistently subvert joint homeostasis,25,56 with subtotal or total meniscectomy increasing the risk of secondary osteoarthritis (OA) changes.31,45 Radiographic abnormalities are present in many patients at midterm follow-up.24,45 Accordingly, in recent years, increasing attention has been paid to meniscal preservation,20,27 although meniscectomy remains commonly performed in cases of nonrepairable meniscal tear.2,32 These findings have prompted the search for solutions to restore meniscal tissue and function, improve symptoms, and prevent the progression of joint degeneration. 12
Meniscal allograft transplantation (MAT) proved to be an effective option in several studies. Preclinical studies demonstrated the potential chondroprotective effects of meniscal transplantation, which appeared to slow down—albeit not to complete cessation—joint degeneration in patients compared with those who had undergone meniscectomy.16,36 Biomechanical studies also demonstrated an improvement in the contact area and peak local contact pressures with MAT compared with total meniscectomy.13,27,37 MAT was also shown to reduce tibial translation and anterior cruciate ligament (ACL) stress because of its function as a secondary stabilizer.27,29,60 However, it is still not clear whether this procedure prevents or slows down cartilage degeneration, consequently delaying knee arthroplasty surgery.1,24,45,54,55 Moreover, although several studies have demonstrated the good results of MAT in young patients with otherwise healthy knees,6,26,35,57 the application of MAT as a salvage procedure in OA joints remains controversial. Although OA has been associated with worse clinical outcomes and a higher failure rate in some studies,23,41 other studies have documented satisfactory results with long-term follow-ups, even in knees with severe cartilage damage.48,52
This study aimed to document the long-term survival of MAT performed as a salvage procedure in patients with knee OA. The hypothesis was that MAT would significantly reduce pain and increase the function of the affected joint at a long-term follow-up compared with the preoperative condition, with a low number of failures and knee replacement surgeries.
Methods
Patient Selection
The treatment was approved by the local ethics committee and internal review board of the Rizzoli Orthopaedic Institute (Bologna, Italy), and all patients gave their informed consent. All MAT procedures were performed by the senior author (S.Z.) at the Rizzoli Orthopaedic Institute between 2004 and 2012. Patients were screened and assessed for eligibility according to the following inclusion criteria: medial or lateral MAT procedure; age between 18 and 60 years; and Kellgren-Lawrence grades (KL) 2 and 3. The exclusion criteria were as follows: follow-up periods of <10 years and KL grades 1 and 4. Other exclusion criteria included infectious, neoplastic, metabolic, and inflammatory diseases. Indications for MAT were unicompartmental pain in the presence of a total or subtotal “functional” meniscectomy (ie, meniscal degeneration due to previous trauma) or in the setting of revision of ACL reconstruction when the meniscal deficiency was believed to be a contributing factor for primary ACL failure. A concurrent corrective osteotomy was performed in patients who had >5° of malalignment. In patients with focal Outerbridge grade 4 chondral lesions <2 cm2, microfractures were performed, whereas in cases of larger focal Outerbridge grade 4 lesions, a scaffold was implanted.
Surgical Technique
Fresh-frozen (–80°C) nonirradiated and nonantigen–matched allografts were implanted. The age of the donors ranged from 15 to 35 years. Anthropometric parameters 21 were used to establish the correct size of the graft. The transplantation was performed arthroscopically without bone plugs, with soft tissue fixation and transtibial tunnels. 15 The remnant of the native meniscus was removed up to the menisco capsular zone. A tibial tunnel aimed at the posterior horn insertion was prepared above the planned osteotomy line to secure the suture at the posterior meniscal horn level to the anterior tibial cortex. The prepared graft was inserted with a Kelly clamp into the joint after passing a shuttle suture through the posterior tunnel. By pulling the shuttle suture, the graft was located in the correct position and fixed to the capsule with “all-inside” stitches (either Fast-Fix, Smith & Nephew, or Truespan, Depuy Synthes). The first suture was positioned at the junction between the posterior horn and body to immediately stabilize the graft in the correct position. The shuttle suture of the MAT was retrieved and tied against the tibial cortex to fix the graft's posterior horn. No outside-in fixations were used. The anterior horn of the MAT was fixed with a second anterior tibial tunnel (Figure 1).
Arthroscopic view of the meniscal allograft transplantation procedure with soft tissue fixation.
Afterward, the surgeon performed the required concurrent procedures. In cases of varus deformity, a lateral closing-wedge, high tibial osteotomy was performed; contrarily, in the case of valgus deformity, a medial closing-wedge osteotomy of the distal femur was performed unless previous surgeries made the option for open wedge osteotomies preferable. A single-bundle, over-the-top, ACL reconstruction associated with lateral extra-articular tenodesis using a hamstring tendon autograft or an Achilles allograft for revision procedures was performed in patients with an ACL tear. 62 In addition to MAT, arthroscopic or open cartilage procedures were also performed in patients with chondral lesions. 44 Further details on meniscal sizing, surgical steps of MAT, and concurrent procedures are provided in previous studies.14,62 After checking for knee and MAT stability, the skin was closed, and a compressive bandage and a full-extension brace were placed.
Postoperative Rehabilitation
Patients used a full-extension brace for the first month and were allowed to remove it 3 times a day to perform a passive and gradual range of motion restoration up to a maximum of 90° of flexion for the first 2 weeks. After 15 days, graduated recovery of active complete range of motion was expected. From the first week, patients started a muscle enforcement program with isometric exercises. No weightbearing, with use of crutches and brace, was allowed during the first postoperative month. After 1 month, when the active complete range of motion was recovered, gradual abandonment of the crutches was allowed to regain full weightbearing and autonomy.
Patient Evaluation
Patients were clinically evaluated preoperatively and prospectively at a midterm follow-up of 5 years and a long-term follow-up of ≥10 years (mean ± SD, 11.1 ± 1 years). All patient characteristics and surgical details were obtained from the medical charts of those who were considered eligible. Specifically, age, sex, side, medial or lateral meniscal involvement, time since first and last meniscectomy, and previous procedures were obtained. Details of surgical intervention and concurrent procedures were extracted as well. Clinical parameters were rated using the Lysholm score, a 0 to 100 visual analog scale (VAS) for pain scale, and the Knee injury and Osteoarthritis Outcome Score (KOOS). The activity level was recorded using the Tegner score.
50
Details of sports activity and level performed before the onset of knee symptoms and just before the MAT procedure were also recorded. At every follow-up, details of sports involvement, such as type and level of sport, time to return to sports (RTS), and reason for possible sport abandonment or level decrease, were also investigated. According to Hamrin Senorski et al,
17
a knee-strenuous activity was considered if the Tegner score was
The subsequent further surgical procedures and their timing were noted during the follow-up period. The operation was considered failed in case of revision surgery because of persistent symptoms, including meniscectomy, meniscal suture, total knee arthroplasty, and unicompartmental knee arthroplasty. In addition to surgical failures, poor Lysholm scores (<65 points) were considered clinical failures. 9
Statistical Analysis
All continuous data were expressed as mean ± SD; categorical variables were expressed as proportions or percentages. The Shapiro-Wilk test was performed to test the normality of continuous variables. The Levene test was used to assess the homoscedasticity of the data. Repeated measures analysis of variance was performed to compare the scores at different follow-up times. The 1-way analysis of variance test was performed to determine the between-group differences of continuous and normally distributed and homoscedastic data; the Mann-Whitney test was used otherwise. The general linear model was performed as a multivariate analysis on the outcomes at the last follow-up with the score as dependent variable; sex, knee side, graft side, smoking status, previous surgery, concurrent surgery, concurrent ACL (primary and revision surgery), concurrent cartilage (microfractures, cheiloplasty, shavings, osteochondral scaffold implantations, and osteochondral allograft transplantations), concurrent osteotomy as fixed effects; and age, body mass index (BMI), and KL grade as covariates. The Spearman rank correlation was used to assess correlations between numerical scores and continuous data; the Kendall Tau correlation was used to determine correlations between ordinal scores and continuous data. The Pearson chi-square exact test was performed to investigate relationships between grouping variables. The Kaplan-Meier survival analysis was performed to check the survival to failure; the log-rank test was used to assess the influence of treatments on survival. The Cox survival analysis was used as a multivariate analysis for the survival analysis to failure. For all tests, P < .05 was considered significant. All statistical analysis was performed using SPSS Version 19.0 (IBM Corp).
Results
Patient Characteristics
A total of 48 patients were eligible; 1 patient was lost to follow-up, leaving 37 men and 10 women available for the study investigation (Figure 2). Demographic characteristics and surgical details obtained through the medical records are detailed in Table 1.
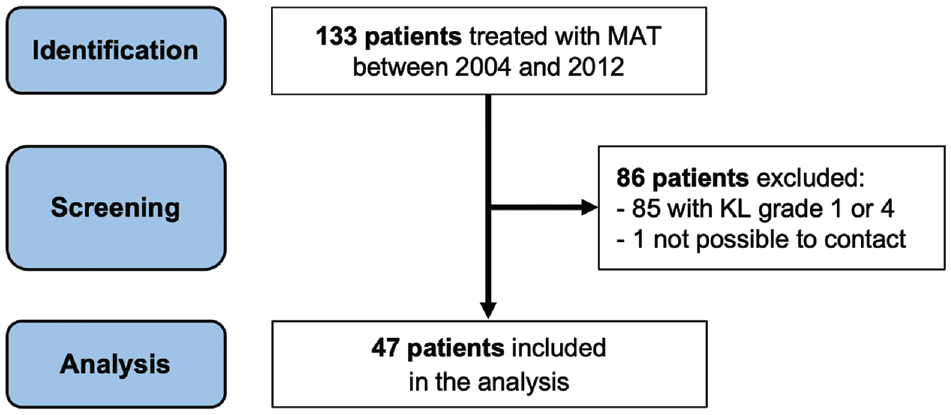
Flowchart of the included patients. KL, Kellgren-Lawrence grade; MAT, meniscal allograft transplantation.
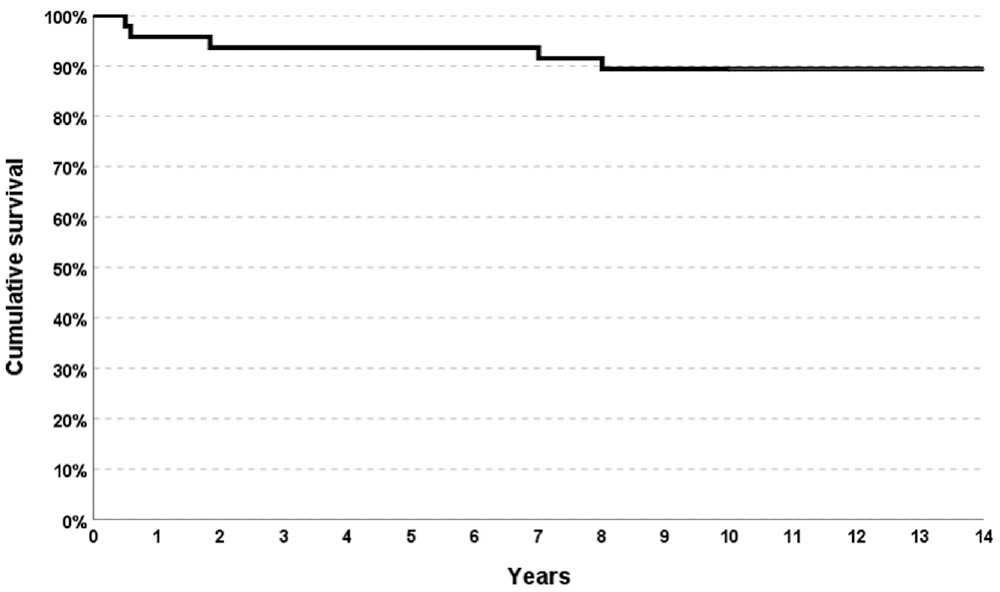
Patient Characteristics a
Data are expressed as mean ± SD (range) or n (%). BMI, body mass index; KL, Kellgren-Lawrence grade; MAT, meniscal allograft transplantation.
The mean age at treatment was 43.5 ± 9 years, with a mean BMI of 25.8 ± 4.3. A total of 44 patients underwent several different procedures previously as follows: meniscectomies (27 medial cases and 21 lateral cases); 1 collagen meniscal implant (Stryker Corp); primary ACL reconstruction (13 cases), and 2 ACL revisions; primary posterior cruciate ligament reconstructions (2 cases); medial collateral ligament retensioning according to the Hughston technique (2 cases); arthroscopic debridement (10 cases); arthroscopic arthrolysis (1 case); arthroscopic lateral release for patellar instability (1 case); cartilage procedures (2 microfractures and 4 shavings); osteotomies (3 high tibial osteotomies and 3 distal femoral osteotomies); 1 hardware removal; and fracture syntheses (2 proximal tibias and 1 distal femur). Additional procedures were needed in 33 patients as follows: 2 meniscectomies; 4 primary ACL reconstructions; 2 ACL revisions; osteotomies (10 closed high tibial osteotomies, 2 open high tibial osteotomies, 4 closed distal femoral osteotomy, and 1 open distal femoral osteotomy); cartilage procedures (9 microfractures, 2 shavings, 2 osteochondral scaffold implantations [Maioregen], and 2 osteochondral allograft transplantations); and 5 cheiloplasty for patellar osteophyte removal.
Most of the patients (83%) would undergo the same surgical procedure again if needed. When asked, “Would you undergo the same surgical procedure again if needed?” 39 out of 47 responded, “Yes.”
Survival Analysis
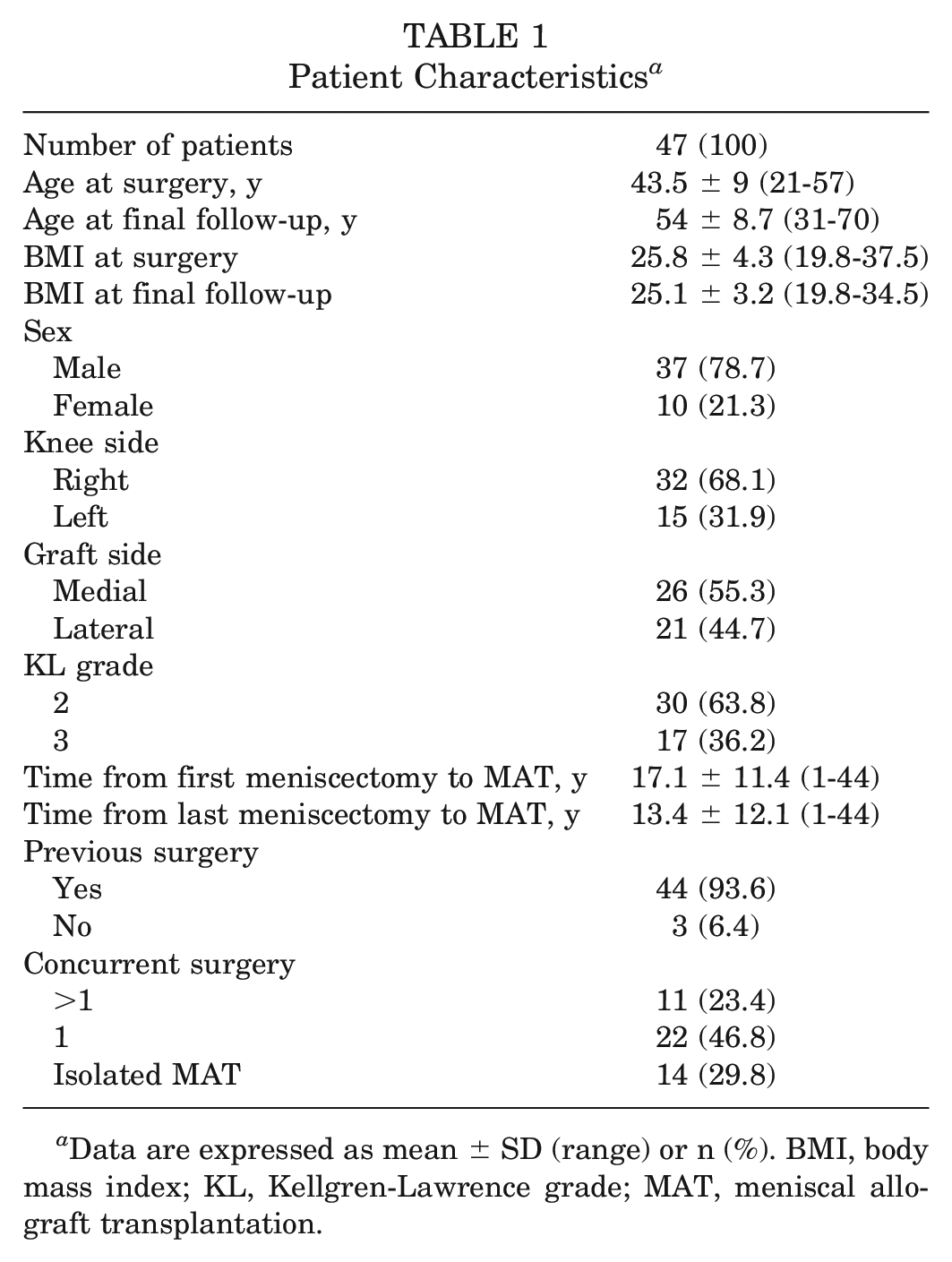
Five patients (10.6%) experienced surgical failures, 4 presenting a clinical condition of <65 of the Lysholm score. Three patients (6.4%) underwent meniscal procedures: 2 were arthroscopically treated with MAT repair (all-inside sutures) at 7 months postoperatively, and 1 had subtotal meniscectomy due to trauma after 22 months. The other 2 patients (4.3%) underwent total knee replacement surgery after 7 and 8 years, respectively. The surgical survival rate was 93.6% at 5 years and 89.4% at 10 years (Figure 3).
The Kaplan-Meier survival curve for surgical failure.
A multivariate analysis was performed with surgical failure as the dependent variable, time to surgical failure as the independent variable, and the following variables as predictors: sex (P = .911), graft side (P = .799), age (P = .969), BMI (P = .820), KL grade (P = .698), time from first meniscectomy to MAT (P = .738), time from last meniscectomy to MAT (P = .867), concurrent surgery (P = .981), concurrent ACL (P = .947), concurrent osteotomy (P = .966), concurrent cartilage (P = .971), knee side (P = .971), VAS preoperative score (P = .970), Lysholm preoperative score (P = .894), Tegner preinjury score (P = .979), Tegner preoperative score (P = .983), and the subscales of KOOS—Symptoms preoperative score (P = .997), Pain preoperative score (P = .971), Sport and Recreation preoperative score (P = .972), Activities of Daily Living preoperative score (P = .972), and Quality of Life preoperative score (P = .910). No predictors of surgical failure were identified with univariate and multivariate analysis. In addition, no survivorship differences were reported based on the relevant variables.
Treatment failed clinically in 15 patients. In particular, the survival rate from clinical failure was 87.2% at 5 years and 68.1% at 10 years (Figure 4A). The number of concurrent surgeries influenced the clinical failures: patients who needed >1 procedure concurrent with MAT had worse mean subjective scores (poor Lysholm) than the others at the final follow-up (P = .018) (Figure 4B).
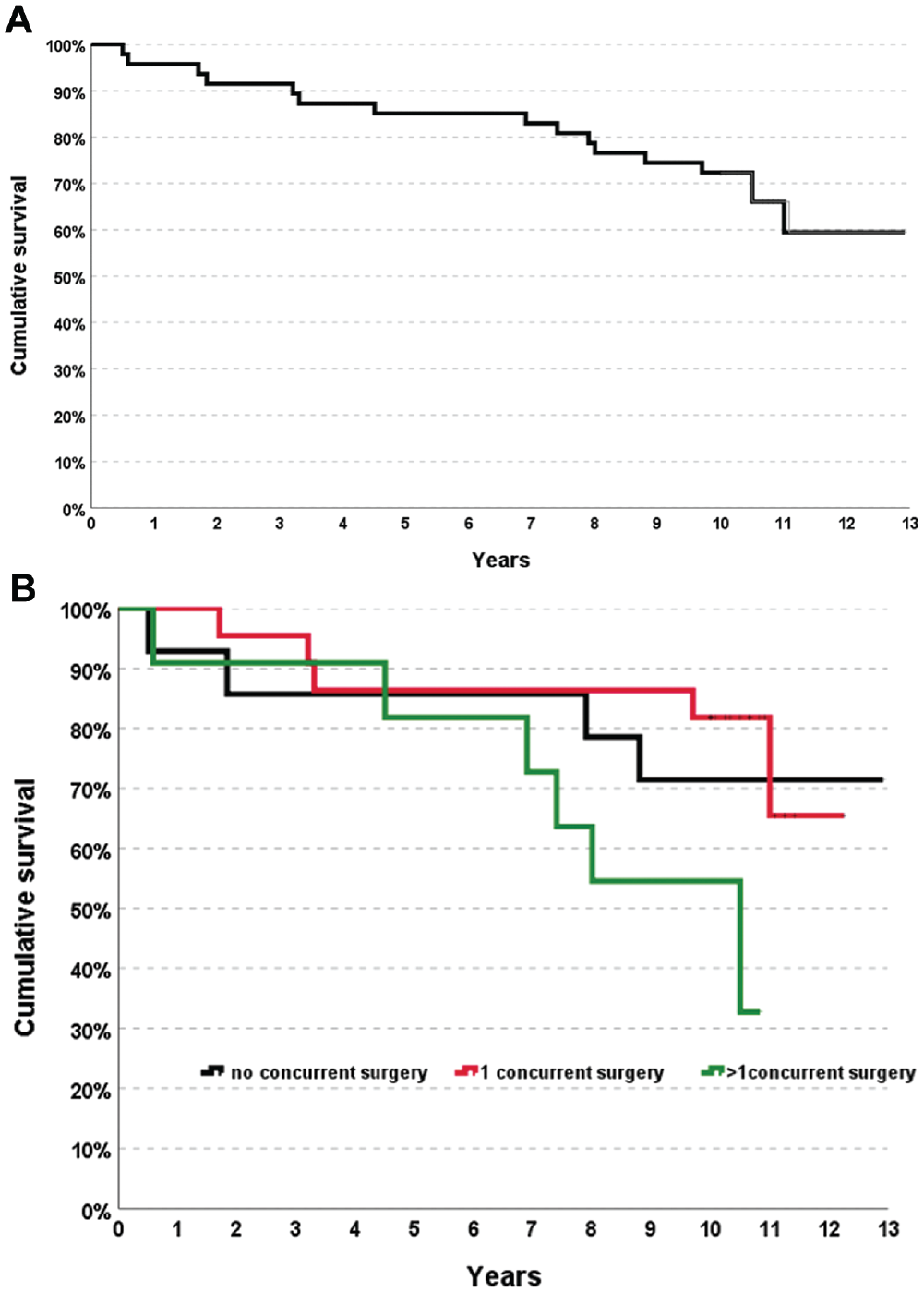
(A) The Kaplan-Meier survival curve for clinical failure. (B) The influence of the number of concurrent surgeries on the clinical failures.
Clinical Outcomes
A statistically significant improvement in all clinical scores was documented from the basal evaluation to the final follow-up. The VAS for pain showed a significant improvement from a baseline score of 72.5 ± 22.6; P < .001) to a 5-year score of 29.9 ± 29.5; P < .001), with a significant worsening of 17 points at the final follow-up (47.2 ± 30.7; P < .001), which remained significantly better than the basal score (P < .001) (Figure 5).
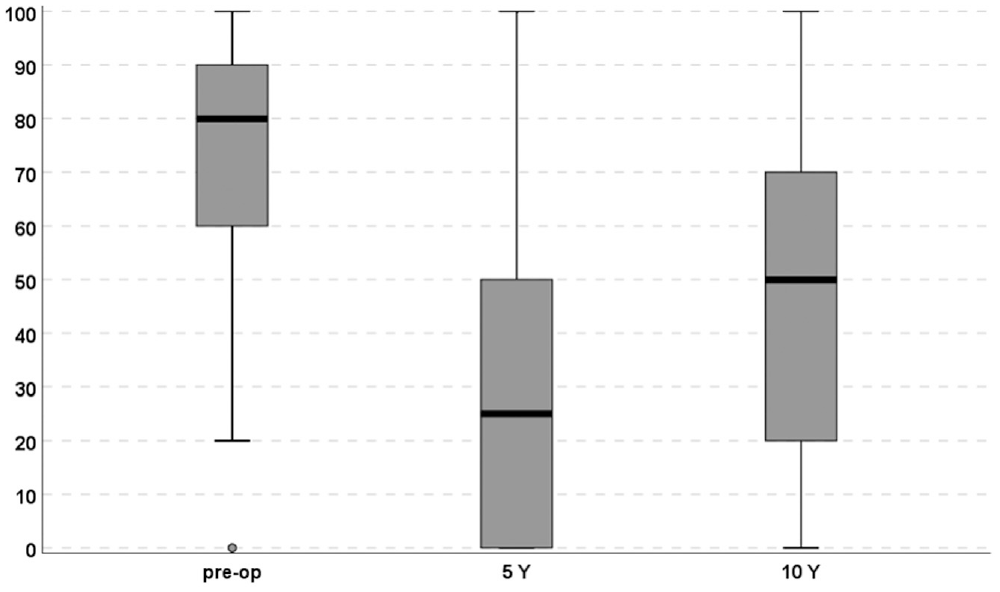
The patient's subjective pain was reported using the visual analog scale score during the follow-up clinical examination. The trend showed a statistically significant improvement at the midterm follow-up, but this result was not maintained at the final follow-up. pre-op, preoperative.
The mean Lysholm score improved significantly from the preoperative score of 46.4 ± 17.2 to 5 years (77.7 ± 20.4; P < .001) and from preoperative to 10 years (71 ± 23.3; P < .001). The decrease from 5 years to the final follow-up was statistically significant (P = .018) (Figure 6).
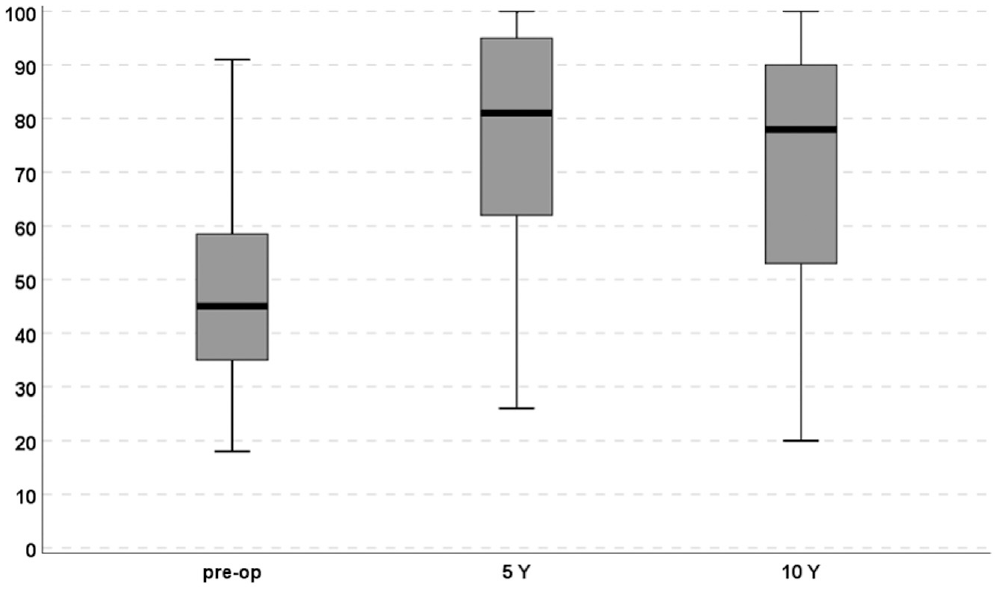
The trend of the Lysholm score showed a statistically significant improvement at any follow-up from the basal score. The slight decrease from 5 to 10 years was significant (P = .018). pre-op, preoperative. Y, years.
The analysis of the KOOS score showed a significant improvement in each item from basal evaluation to final follow-up (P < .001). A similar trend was demonstrated with the Tegner score, which showed a significant improvement from the basal value of 2.4 ± 1.7 to 3.9 ± 1.8 at 5 years (P < .001) and 3.4 ± 1.7 at the final follow-up (P = .165). However, the activity level before the onset of symptoms (5.7 ± 1.9) was not reached at any follow-up (Figure 7).
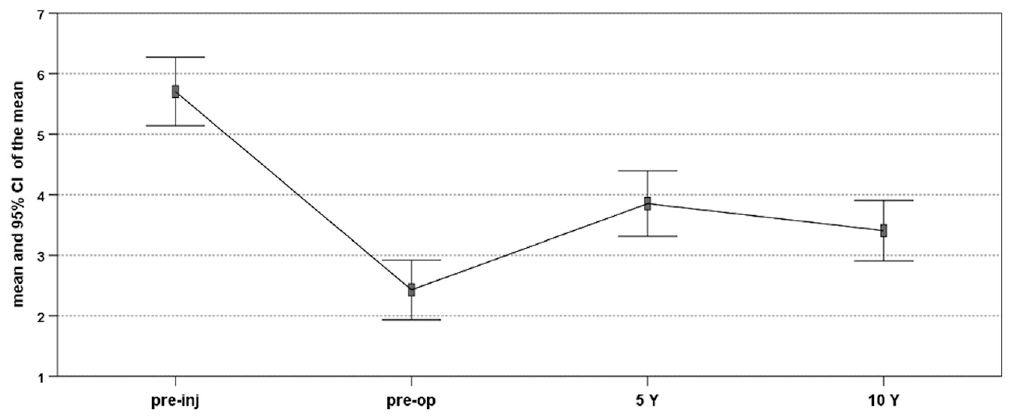
The trend of the Tegner activity scale shows the mean sport level at any follow-up. The slight decrease from 5 to 10 years was not significant (P = .165). pre-inj, preinjury; pre-op, preoperative. Y, years.
At the final follow-up, the global knee subjective function and satisfaction were 56.6 ± 27.3 and 64.7 ± 30.3, respectively, and 40 out of 47 patients (85.1%) said they would undergo surgical treatment again if necessary.
Further analysis was performed to evaluate the parameters that might influence the clinical results. No significant correlation was found between clinical outcomes and patient sex, side, age, smoking, BMI, and KL grade preoperatively, and previous and concurrent surgeries, except for the Tegner score, which decreased in smoking patients at 10 years and in women compared with men at each follow-up (Table 2).
Correlations Between Clinical Outcomes and Patients’ Characteristics a
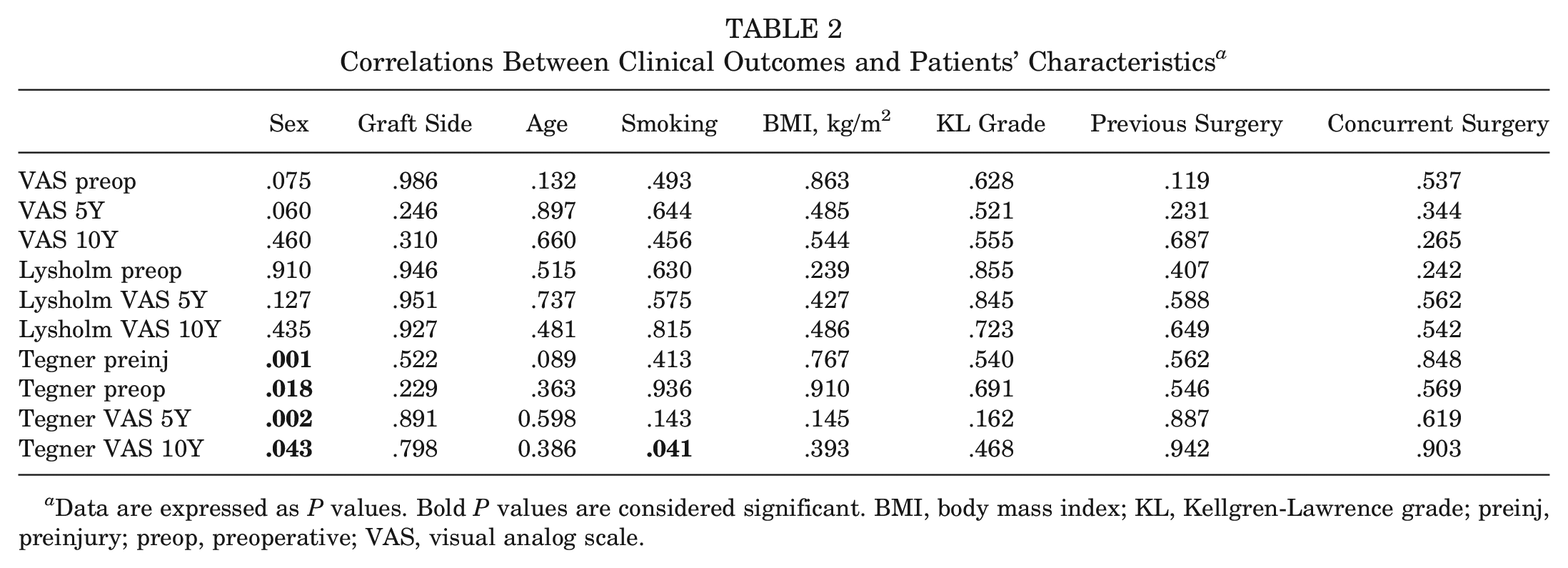
Data are expressed as P values. Bold P values are considered significant. BMI, body mass index; KL, Kellgren-Lawrence grade; preinj, preinjury; preop, preoperative; VAS, visual analog scale.
Subgroup Analysis
A subgroup analysis was conducted between 2 groups of patients according to the OA grade (KL 2 group and KL 3 group) (Table 3). A different trend in the 2 groups was reported at the 10-year follow-up: the KL 2 group showed a significant improvement in the VAS score at any follow-up (P < .001), but the improvement from 5 to 10 years was not significant in the Lysholm score (P = .225). Conversely, in the KL 3 group, the VAS score did not improve significantly from baseline to 10 years (P = .111), while the Lysholm score showed a trend for improvement from 5 to 10 years (P = .084). Despite these aspects, the analysis showed no significant differences in basal demographic characteristics, except for age (P = .032), clinical score improvement, survivorship (Figure 8), satisfaction, and function between the groups. Therefore, the OA grade did not influence the outcome at the final follow-up.
Subgroup Analysis Between KL Grades 2 and 3 a
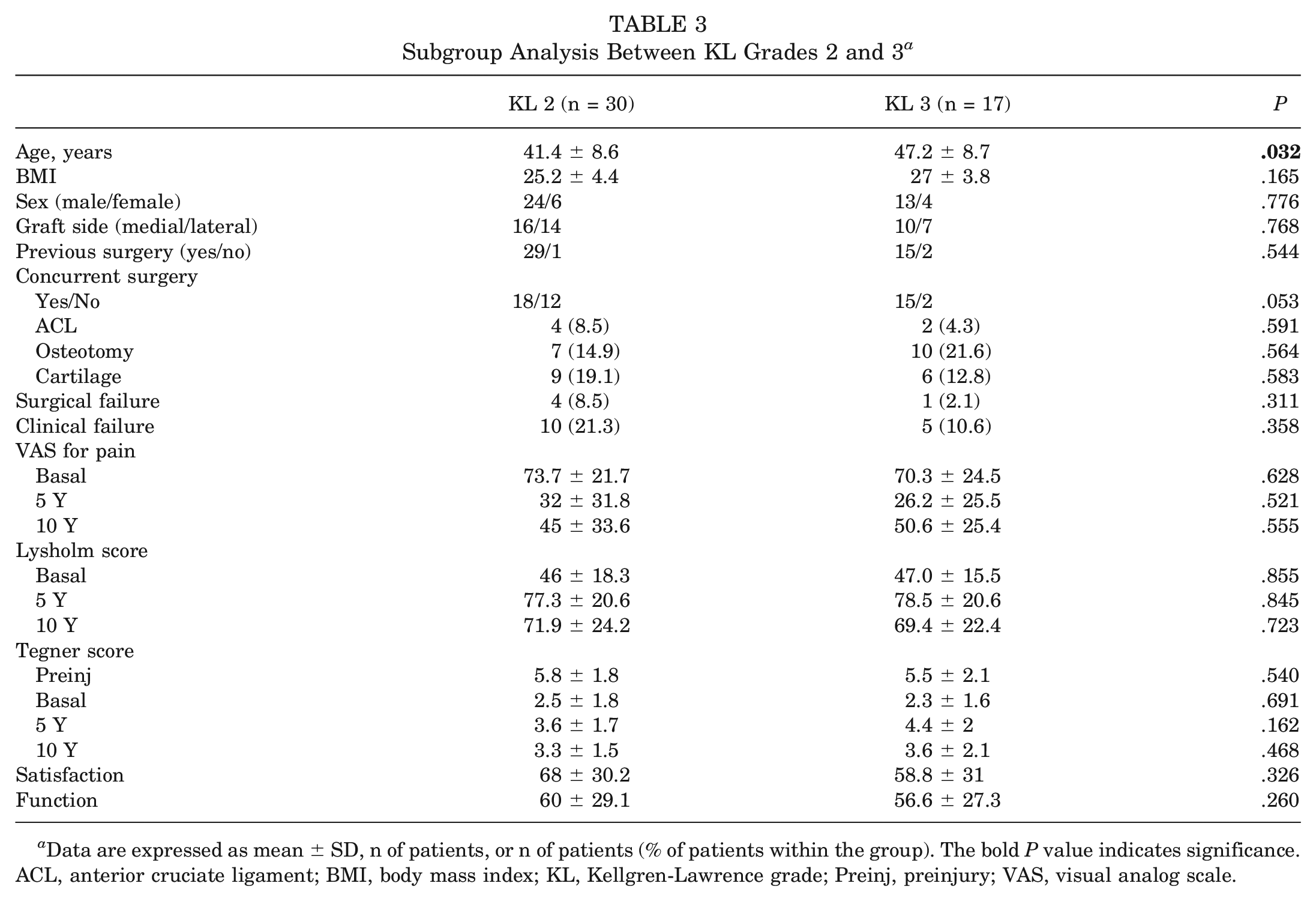
Data are expressed as mean ± SD, n of patients, or n of patients (% of patients within the group). The bold P value indicates significance. ACL, anterior cruciate ligament; BMI, body mass index; KL, Kellgren-Lawrence grade; Preinj, preinjury; VAS, visual analog scale.
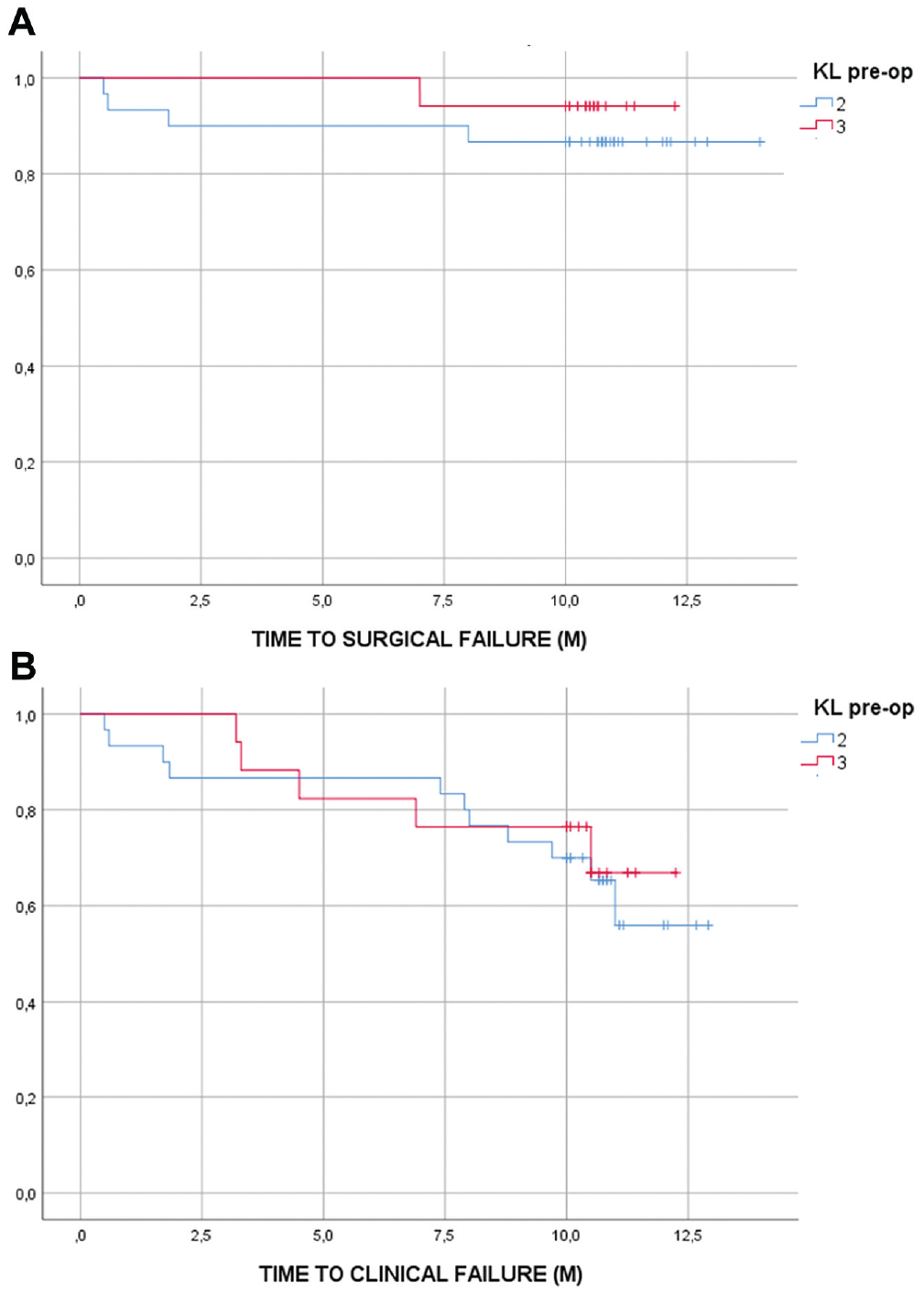
(A and B) The subgroup analysis between the KL 2 group and the KL 3 group did not show a statistically significant difference in surgical and clinical survivorship (P = .422 and P = .698, respectively). KL, Kellgren-Lawrence grade; (M), months; pre-op, preoperative.
Another analysis was performed between patients who underwent osteotomies (osteotomy group) and patients without any realignment concurrent procedures (nonosteotomy group). An intergroup difference was reported in the clinical scores (Table 4): the nonosteotomy group showed a statistical improvement at any follow-up for the VAS and the Lysholm score (P < .001), whereas the osteotomy group did not show a significant improvement from 5 to 10 year follow-up, both for the VAS score (P = .062) and the Lysholm score (P = .480). Finally, the multivariate analysis, using the general linear model, showed that the osteotomy group improved significantly in the Tegner score from baseline to 10 years compared with the nonosteotomy group (P = .027; η2 = 0.152). Despite these aspects, the analysis showed no significant differences in clinical outcomes between the 2 groups at 10 years. Therefore, the need for a concurrent osteotomy did not influence the clinical results at the final follow-up.
Subgroup Analysis Between the Nonosteotomy Group and the Osteotomy Group a
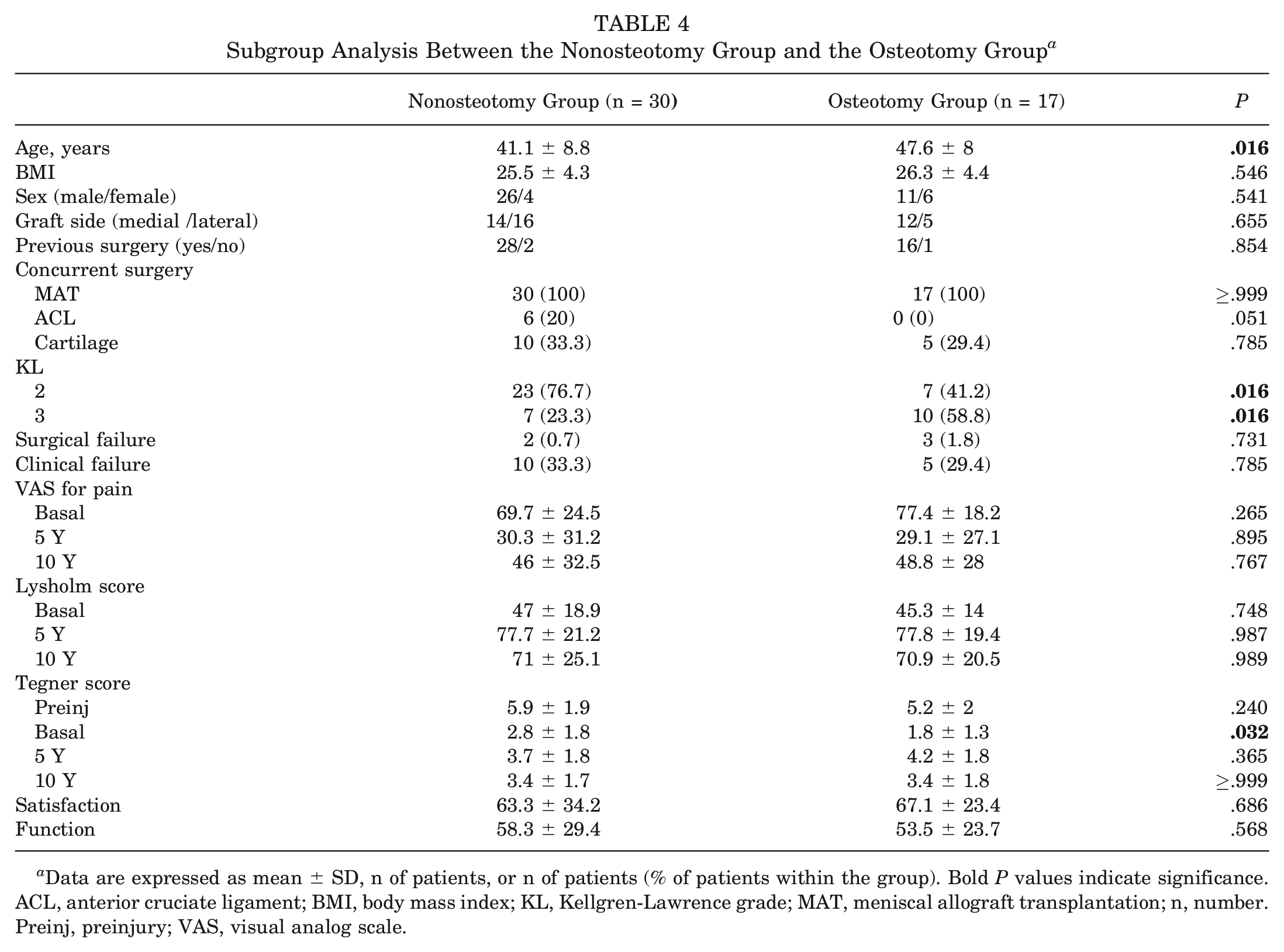
Data are expressed as mean ± SD, n of patients, or n of patients (% of patients within the group). Bold P values indicate significance. ACL, anterior cruciate ligament; BMI, body mass index; KL, Kellgren-Lawrence grade; MAT, meniscal allograft transplantation; n, number. Preinj, preinjury; VAS, visual analog scale.
Discussion
The main finding of this study is that MAT can provide good clinical outcomes over time and delay knee arthroplasty or other invasive treatments up to a long-term follow-up, even when used as salvage procedures in patients with knee OA.
Although traditionally considered to restore meniscal tissue and function in non-OA joints, MAT has been increasingly used in more challenging joints affected by multiple lesions and degeneration, with complex concurrent procedures showing good clinical results.30,61 However, the challenging OA environment may jeopardize treatment success over time. In this light, this study provides key data demonstrating the long-lasting clinical benefit of MAT when used in OA joints, postponing the need for more invasive procedures in most patients. A statistically significant improvement in all clinical scores was documented; the Lysholm score in particular showed a significant improvement exceeding the minimal clinically important difference threshold. 28 Therefore, the clinically significant improvement maintained at the long-term follow-up supports the usefulness and indication of MAT in patients with knee OA.
Also, RTS showed encouraging results considering the type of treated patient population— 76.6% of the patients practiced sports 10 years after transplantation, but only 12 patients (26%) returned to the same sports level as before the injury or onset of symptoms, and only 6 patients (13%) returned to knee-strenuous sports for the knee. 17 The need for concurrent osteotomy has improved the sports activity level from the baseline to the final follow-up compared with those who did not undergo this procedure. This finding should encourage surgeons to address all defects in a single surgical step when necessary. Finally, the analysis of correlations between patient characteristics and clinical outcomes has revealed that women had a lower activity level than men at each follow-up. The sex difference in RTS after MAT is a sparsely explored topic in the present literature, and patient groups with limited female representation are often examined.6,57 Contrarily, sex-related aspects have been evaluated in other studies on RTS after ACL reconstruction, where women were found to be less inclined to return to their preinjury level of sports with more psychological obstacles compared with men.3,49,58 Further comparative studies will be needed to assess the role of sex in RTS and after MAT on large patient cohorts.
It remains to be demonstrated whether the clinical benefit is related to a joint biomechanical environment that can address and slow down the joint degenerative processes. Nonetheless, the primary goal of patients seeking physician advice is to improve their symptoms and avoid more invasive procedures. To this aim, MAT proved successful, with only a minority of patients with failed treatment after more than a decade. Also, when failure analysis is not limited to patients undergoing further surgery, a broader clinical definition of clinical failures is included, and many patients benefit from this procedure. In fact, despite presenting a decrease in the clinical parameters at the latest follow-up, the survival rate remains considerable in light of the complex scenario addressed. Thus, while caution is warranted, especially in the most damaged joints requiring multiple surgeries— which showed a higher failure rate—these results suggest the possibility of broadening the original treatment indication, showing that patients with OA joints can also benefit significantly from MAT, at least in terms of clinical outcome.
Several studies6,23,53,62 have tried to address the potential of MAT to counteract the OA processes, with controversial findings. The documented clinical benefit has not been coupled with clear evidence proving the protective effects of MAT on articular cartilage, with a lack of high-level clinical studies. Moreover, the heterogeneity of patients’ demography, different inclusion and failure criteria, techniques, graft types, associated and previous procedures, revisions, and follow-ups complicate an adequate comparison, as highlighted by a recent systematic review. 46 In this series, patients aged between 21 and 57 years underwent >90 previous surgical procedures before MAT and >40 concurrent procedures with MAT. This inevitably complicates the assessment of the final clinical outcome, as well as its comparison with other studies, and quantifying the specific clinical benefits derived from the MAT procedure proves challenging. On the other hand, in a complex population affected by knee OA, it is important to address all existing defects, such as instability, malalignment, and cartilage injuries, to reduce the failure.42,62 Future studies will be required to analyze homogeneous patient groups for a more specific assessment of the effect of MAT on the final benefit.
The protective role of MAT remains at the center of the scientific discussion, as well as in the preclinical, ex vivo, and silico settings,33,40,59 although it remains difficult to directly quantify the mechanical-biological consequences of meniscal surgery in different patients. 40 Studies in animal models have suggested that medial MAT can minimize degenerative changes in tibial cartilage, even though biochemical changes still suggest degeneration after 6 months.4,19 The limited quality of MAT implanted may explain the partial results.4,19 A correlation between magnetic resonance imaging (MRI) and histological appearance has been demonstrated, with only a partial degree of allograft cell viability and vascular ingrowth in allograft explants. 22 These alterations cast doubts on the true capability of the transplants to provide chondroprotection. Other studies have compared the radiological results of MAT after meniscectomy versus meniscectomy without MAT in animal models. The authors reported that MAT may result in fewer degenerative changes than knees treated with meniscectomy only. 39 On the other hand, rabbit knees that had undergone immediate transplantation showed more degenerative changes in the medial femoral condyle at 1 year compared with 6 weeks after surgery, 1 suggesting the possibility to delay but not to prevent the progression of degenerative changes.1,10,39
Despite the controversial preclinical results and the limited clinical evidence on the protective properties of MAT, studies have shown acceptable survival rates in the clinical setting at long-term follow-up. In a series of 49 patients with moderate to severe cartilage damage (Outerbridge 3-4), Stone et al 48 documented a failure rate of 22.4% at a mean of 5.2 ± 4.4 years with a mean follow-up time of 8.6 ± 4.2 years. Kempshall et al 23 showed the results of 99 consecutive MATs in patients with low grade (group A) and high grade (group B) cartilage status at a mean follow-up of 2.9 years (range, 1.1-9.1 years). The survivorship of patients in group B was 78%, with a mean time to failure of 1.12 years. Verdonk et al 52 reported on a series of 100 patients treated with MAT, including patients with severe OA grade, with an overall failure rate of 21%. The mean cumulative survival time (11.6 years) was identical for the medial and lateral MATs at a mean follow-up of 7.2 years. The present study shows that a low reintervention and failure rate can be obtained even in OA joints.
This study also underlined another important factor that should be evaluated when considering MAT indication because not all patients benefited the same from this procedure. A correlation was found between the number of concurrent surgeries and the clinical failure rate. In particular, results were significantly worse when >1 concurrent procedures were performed. Of note, all patients with clinical failure at 10 years who underwent >1 concurrent procedures had received cartilage treatment, such as microfracture, cheiloplasty, and osteochondral scaffold implantation. This finding has also been reported in other studies investigating factors influencing the clinical outcome and showing that concurrent cartilage procedures are linked to worse clinical outcomes and failures.23,41 However, not all authors confirmed this aspect8,35,41,47: Saltzman et al 41 showed that the chondral damage treated with cartilage restorative procedures at the same time as MAT in a cohort of 91 patients might not affect the clinical outcome of MAT. The study reports short-term results; conversely, the present study shows an increase in clinical failures after the midterm follow-up, in addition to addressing more challenging joints. Therefore, the hypothesis is that combined MAT and cartilage procedures would give good short- and midterm results, but a reduction in long-term benefit could be expected for complex lesions requiring >1 concurrent procedures. In this series, 5 patients experienced surgical failures with a survival rate of 93.6% at 5 years and 89.4% at 10 years, with no differences in survival from surgical failure according to the relevant variables. In this regard, a recent systematic review on long-term MAT survival by Novaretti et al 34 showed a worse surgical survival rate compared with the findings of the present study. Extreme care must be taken when comparing failure rates between different series of MAT. As the criteria for failure are controversial, multiple criteria are used, including knee replacement, graft removal, poor clinical outcomes, and evidence of graft tears by MRI.
Another important aspect that could complicate the interpretation of the results when comparing different series of patients is the age at the time of treatment. According to a recent review, 34 the mean age of patients undergoing MAT is relatively low (33.1 years), which contrasts with this study (43.5 years). The higher mean age is probably related to the selection of patients with knee OA. Despite this difference, the results of this study showed that even patients with a mean age of 43.5 years and with knee OA can benefit from MAT, avoiding more invasive treatment options (unicompartmental or total knee arthroplasty) or at least postponing them significantly. This is an important result. When these procedures are performed in younger patients, there is a lower survival and satisfaction rate, 43 which may lead to the need to revise these procedures at a relatively young age. Therefore, the survival results reported in this study highlight the capability of MAT to act as a salvage procedure for this population, offering long periods of improvement in the patient's quality of life.
This study reports on an extensive series of patients treated for this specific indication, with results strengthened by a long-term follow-up. Still, this study also has some limitations. Many patients underwent a concurrent surgical procedure with MAT or a different previous surgery. This makes it difficult to discern how much of the improvement is derived from the MAT and how much from the concurrent procedure. However, this heterogeneous population represents the typical patient profile that is referred to high-level knee surgery centers, and the surgical approach should include different associated procedures to address all the underlying knee pathology. Moreover, this aspect reflects the real-world scenario, where the patient needing a meniscal biological replacement is complex and unlikely to fit well-defined criteria. An evaluation with radiological examinations (radiograph and MRI) at the subsequent follow-ups was not performed. However, previous studies have shown no correlation between the radiological finding and the clinical outcome or failure rate in several series. If, on one hand, the joint space narrowing and the meniscal extrusion have been demonstrated to be highly predictive of the need for future OA-related surgery, 5 several authors have reported the limitations of the use of these parameters as a surrogate for OA progression.7,18,35 In light of these aspects, clinical results and failure rates are the most significant outcomes to be evaluated for this specific cohort of challenging patients. More than the restoration of the stabilizing or chondroprotective function of the meniscus in the poor condition of the knee with OA, the possibility of recovering a satisfactory quality of life and of postponing the need for more invasive surgery are the key issues for these patients, who benefited from MAT transplantation. This is particularly important considering the risks associated with knee replacement at a young age, and the potential benefits of postponing prosthesis implantations from both the patient and the health care perspective.11,38
Conclusion
MAT surgery has proven to be a valid option for improving pain and function even in OA joints (KL grades 2-3), yielding satisfactory results despite a worsening clinical outcome in the long-term follow-up. Therefore, based on the data from this study, orthopaedic surgeons may consider recommending MAT as a salvage procedure even in knees affected by early to moderate OA, while advising patients whose need for combined interventions could potentially reduce graft survival.
Footnotes
Acknowledgements
Special thanks go to Elettra Pignotti for her help with the statistical analysis.
Submitted November 20, 2023; accepted March 22, 2024
One or more of the authors has declared the following potential conflict of interest or source of funding: S.Z. has received institutional support from Fidia Farmaceutici, Cartiheal, IGEA Clinical Biophysics, Biomet, and Kensey Nash; grant support from I+; and royalties from Springer outside the submitted work. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.