
Abstract
Background:
Although clavicle fractures are a common sports injury, there are limited studies on the incidence and causes of clavicle fractures among winter sports athletes.
Purpose:
To evaluate the characteristics and injury mechanisms associated with clavicle fractures among patients evaluated at a Colorado ski resort.
Study Design:
Descriptive epidemiology study.
Methods:
This was a retrospective descriptive analysis of patients with clavicle fractures at the Denver Health Winter Park Medical Center during the 2012-2013 to 2016-2017 ski seasons. Chart review was performed on the patient cohort to confirm clavicle fracture diagnosis and to evaluate factors associated with clavicle fracture.
Results:
A total of 393 clavicle fractures (6.2% of total clinic visits) occurred during the study period, corresponding to an overall clavicle fracture incidence of 8.4 per 100,000 participant-visits. The mean patient age was 26.4 years (range, 5-73 years). The majority were middle-third fractures (85.5%), occurring mainly in men (87.3%). More than half of the fractures were comminuted (54.5%) and occurred in snowboarders (55.0%). The most common mechanism of injury was a fall onto snow while skiing or snowboarding (92.4%). Women sustained more clavicle fractures while skiing compared with snowboarding (82.0% vs 18.0%; P < .001), while men sustained more fractures while snowboarding compared with skiing (60.3% vs 39.7%; P < .001).
Conclusion:
Clavicle fractures are relatively common, but there are scant incidence data for clavicle fractures in mountain sports. Consistent with prior studies, clavicle fractures were more common in younger patients and men. The most common anatomic fracture location was the midclavicle. A greater proportion of clavicle fractures among men were sustained during snowboarding and among women during skiing.
Keywords
Clavicle fractures make up between 2.6% and 10% of all fractures across all sports 3,5,10,13,25,30 and are common skiing and snowboarding injuries. One study at a ski clinic in Taos, New Mexico, found a clavicle fracture rate of 7.1 per 100,000 mountain visits in skiers and snowboarders over the course of 2 winter sports seasons. 23 Prior population studies have cited a clavicle fracture incidence in the United States ranging from 21.8 to 91 per 100,000 person years, 6,10 with a worldwide incidence ranging between 17.4 and 91 per 100,000 person years. 3,6,9 –11,13,18 Overall, younger men are most likely to fracture the clavicle, 3,11,28,29 but some studies have found a bimodal age distribution of injury with a second peak in older patients. 3,11,18 The most common mechanism of injury is direct trauma to the shoulder or clavicle, 3,6,11,13,18,25,30 and athletic injuries account for around half of all clavicle fractures. 6
The clavicle is a curved bone that connects the upper arm with the axial skeleton, functioning to stabilize the glenohumeral joint. 5,6,30 It is anatomically divided into medial (proximal), middle (midshaft), and lateral (distal) thirds. 30 The medial portion is supported at the sternoclavicular joint, while the distal portion is reinforced by the acromioclavicular joint 13 ; therefore, the middle third of the clavicle is most vulnerable to fracture without the additional anatomic muscular and ligamental support. 13,30 This aligns with prior findings that the middle third is the most common region of the clavicle to sustain fractures. 3,5,6,13,18,25,30
There are epidemiologic data available regarding clavicle fractures in the United States and countries throughout the world; however, there are a paucity of incidence data available specifically regarding clavicle fracture among mountain sports. Much of the prior data for winter mountain sports were collected from self-reports, ski patrol, or outside trauma centers and focus on overall incidence of all injuries. 22 The aim of this study was to examine characteristics, injury mechanisms, and clavicle fracture types that were evaluated at the Denver Health Winter Park Medical Center mountainside clinic in Winter Park, Colorado, during the 2012-2013 to 2016-2017 ski seasons.
Methods
Setting and Study Population
This retrospective descriptive epidemiological study was conducted using data from the 2012-2013 to 2016-2017 ski seasons at the Denver Health Winter Park Medical Center. The study population included people who sustained a clavicle fracture at Winter Park Resort while skiing or snowboarding and who were evaluated at the Denver Health Winter Park Medical Center (a community clinic and level 5 trauma center) at the base of the resort. Individuals injured on the mountain are brought down via toboggan by ski patrol and referred to the clinic for further care if deemed necessary. Moreover, individuals who can ski or snowboard down on their own accord are either first evaluated by ski patrol and then are triaged similarly or evaluated directly at the clinic.
Only injured patients ultimately evaluated at the clinic and who received a diagnosis of clavicle fracture through physician evaluation and plain radiography were included in the study. Patients who refused medical care or were not evaluated at the clinic were not included. Patients injured during other activities (eg, sledding, tubing, cross-country skiing, slipping on ice in the parking lot) were likewise excluded. All study protocols and procedures were approved by an institutional review board.
Data Collection
Injury information was collected from the clinic via retrospective medical chart review. For the 2012-2013 and 2015-2016 ski seasons, 2 research assistants (L.P., P.R.A. [professional research assistant]) reviewed scanned handwritten clinic notes. In the 2016-2017 season, Denver Health Winter Park Medical Center upgraded to a full electronic health record system, making data available through online queries. If a patient sustained multiple injuries, the first listed diagnosis (the most clinically important in the physician’s opinion) was used for analysis unless the patient sustained head trauma (excluding superficial injuries such as abrasions) or a fracture.
All charts were reviewed individually. Each radiograph was interpreted by 2 of the authors (L.O., M.K.) and compared with the formal radiology read. Only 17 fractures were not interpreted by the radiologist beyond the simple explanation of clavicle fracture; these were reviewed and categorized by 2 authors (L.O., M.K.). Generally speaking, degree of displacement, angulation, or shortening of fractures were not reported by the radiologist and were calculated by the lead author (L.O.). Degrees of angulation and displacement were calculated using the patient radiographs with the largest degrees of angulation and displacement, respectively. Shortening was measured utilizing the cortex-to-corresponding-cortex method. 15 Fractures were categorized into medial, mid-, and lateral clavicle. Lateral fractures were categorized based on Neer classification. 17 In addition to injury information, age, sex, residence (Colorado vs out of state or foreign), injury mechanism, and disposition were obtained from clinic records. Self-reported ability level, slope difficulty on which the injury occurred, and use of rented/borrowed versus owned equipment were collected from ski patrol records (only available for patients who were evaluated by ski patrol first). Disposition was categorized as transferred to another facility or discharged home. Transferred patients included those sent to another medical facility via ambulance or helicopter and those who were instructed to seek immediate further medical care but chose to transport themselves. The number of participant visits (for calculation of clavicle injury rate) corresponded to the number of unique scanned passes or tickets per day.
Statistical Analysis
All analyses were performed in SPSS Version 26 (IBM). Before analysis, data were inspected for quality, distribution, and missingness. Clinic records from the last week of 2015-2016 were not scanned into the electronic health record and were therefore unavailable. Means and standard deviations were calculated for continuous variables and frequencies and percentages for categorical variables. Statistical comparisons were made using independent t tests for continuous variables and Pearson chi-square for categorical variables. Negative binomial regression was used to estimate injury rates over time. P <.05 was considered statistically significant (α = .05).
Results
During the study period, there were 393 clavicle fractures (6.2% of total clinic visits), corresponding to an overall clavicle fracture incidence of 8.4 per 100,000 participant visits. The mean age of the patients was 26.4 ± 14.5 years (range, 5-73 years). The majority of clavicle fractures occurred in men (87.3%) and as a result of snowboarding (55.0%). Table 1 summarizes the characteristics of patients with clavicle fractures categorized by sport. Most patients were not from the state of Colorado (63.1%). The overall clavicle fracture rate did not change during the study period (P = .22) (Figure 1). Most clavicle fractures were sustained among younger snowboarders and skiers (Figure 2A) and among younger men (Figure 2B).
Characteristics of Patients With Clavicle Fractures Categorized by Sport a

a Data are reported as n (%). Bolded P values indicate statistically significant differences between the study groups (P < .05).

Clavicle fracture count categorized by sex and sport with rates per 100,000 participants over time. The overall trend in rates was not statistically significant (P = .22).

Clavicle fracture count by (A) sport and age and (B) sex and age.
Characteristics of clavicle fractures are summarized in Table 2. The most common mechanism of injury was a fall onto the snow while skiing or snowboarding (92.4%). The majority (85.5%) were midclavicle fractures (Figure 3).
Clavicle Fracture Characteristics Categorized by Sex and Sport a
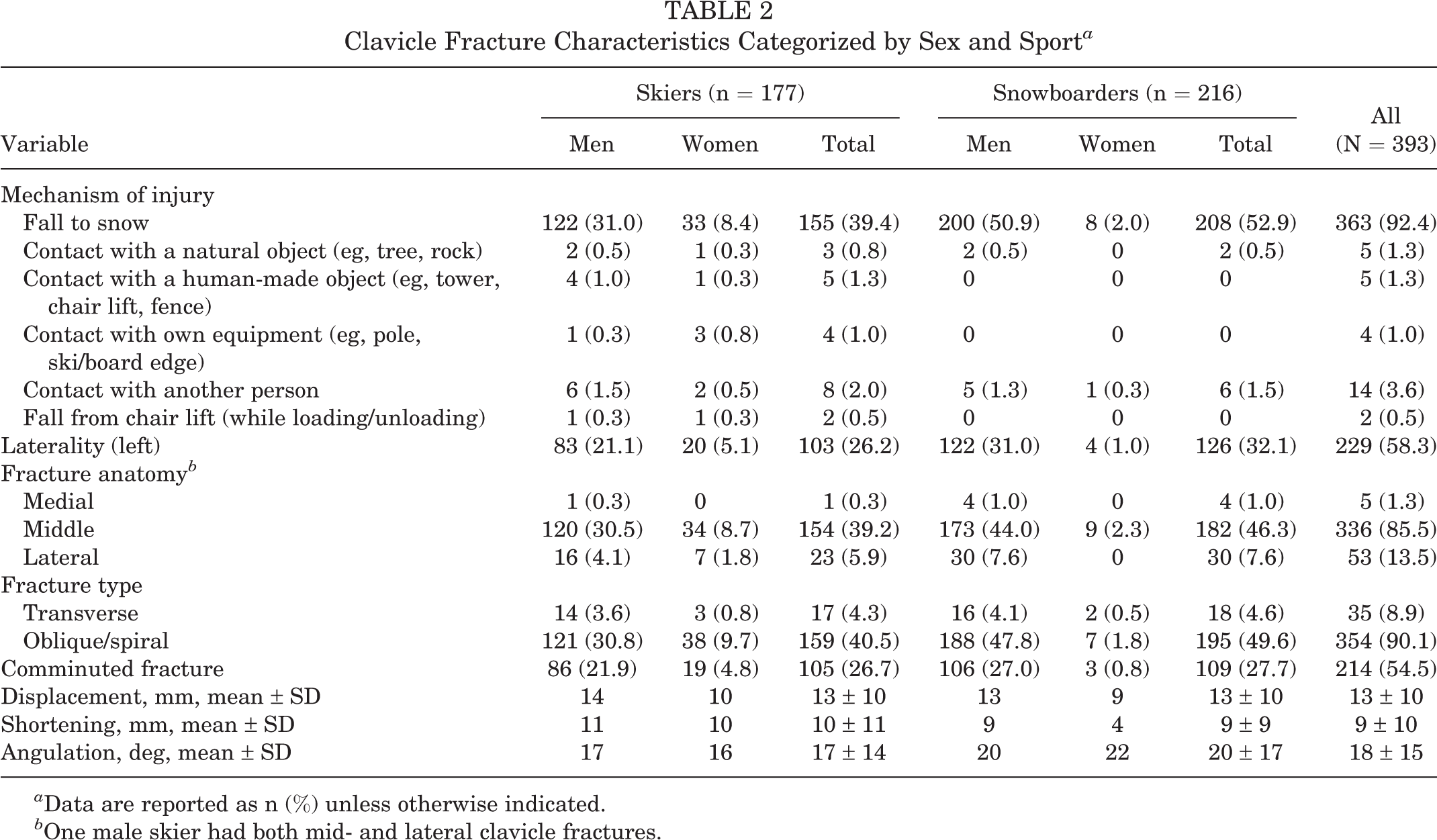
a Data are reported as n (%) unless otherwise indicated.
b One male skier had both mid- and lateral clavicle fractures.
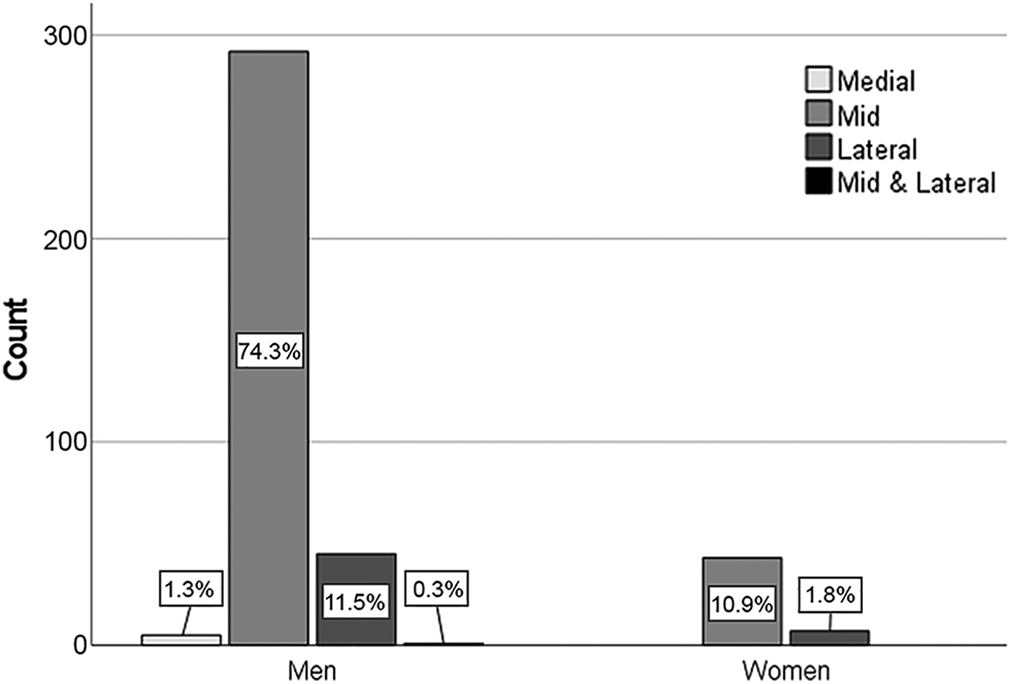
Clavicle fracture count by anatomic category and sex. All categories sum to 100%.
Among those with lateral clavicle fractures (n = 53), type 2A Neer classification was the most common (n = 23; 43.4%), followed by type 5 (n = 11; 20.8%), type 1 (n = 9; 17.0%), type 3 (n = 7; 13.2%), and type 2B (n = 3; 5.7%). More than half of clavicle fractures were comminuted (54.5%). Most fractures were oblique/spiral (90.1%). Only 19 (4.8%) of the fractures were intra-articular. There was only 1 (0.3%) patient with an open clavicle fracture, and only 5 (1.3%) patients needed to be transferred to a higher level of care facility. A small number of fractures were nondisplaced (n = 36; 9.2%), with no shortening (n = 92; 23.4%) and without angulation (n = 27; 6.9%).
There were no differences between women and men in anatomic location of the clavicle fracture (P = .88). Women more frequently sustained clavicle fractures while skiing compared with snowboarding (82.0% vs 18.0%; P < .001), while men were more likely to sustain an injury as the result of snowboarding (60.3% vs 39.7%; P < .001) (Figure 4).

Clavicle fracture count by sports type and sex.
Discussion
This study found that 393 clavicle fractures were sustained over the study period, resulting in an incidence of 8.4 per 100,000 participant visits to the resort. It is likely that our study underestimates the true incidence, as it captures only those who came to the clinic for medical care. However, as the mountainside clinic is the only trauma facility within approximately 32 km (20 miles), 19 it is likely that these data include the majority of clavicle fractures sustained at the resort. Our findings are consistent with prior epidemiologic data from a ski clinic in Taos, New Mexico. 23 Rust et al 23 found a clavicle fracture rate of 7.1 per 100,000 mountain visits, a rate that included both skiers and snowboarders during the second half of the 2006-2007 to 2009-2010 seasons. Our findings showed that clavicle fractures accounted for 6.2% of the total injuries, which is slightly higher than other mountain sports data showing that clavicle fractures accounted for 3.6% of total injuries of skiers and snowboarders. 1 This difference could be due to different study designs, as the data in the study of Basques et al 1 were from a national database rather than a slopeside ski clinic. Other contributing factors could include the distance of the trauma centers from the slopes or the patients’ experience levels, as this information was not available. 1 Our findings do align with prior studies, however, when the total injuries are stratified into skiing and snowboarding. Our study found that clavicle fractures in skiers made up 2.8% of total injuries as compared with prior findings of 2.2%, 1 while clavicle fractures in snowboarders were 3.4% of total injuries compared with 0.8% to 5% noted in other studies. 1,8,14,31
Consistent with prior clavicle fracture data, we found that the midclavicle was the most commonly fractured portion of the bone. 3,5,6,13,18,25 In our study, midclavicle fractures accounted for approximately 85% of all clavicle fractures. Previous studies have found that between 69% and 82% of fractures occur in the midclavicle. 13 Two studies found that medial and lateral clavicle fractures occur with higher frequency as patients' ages increase. 13,18 According to the Snowsports Industries America (SIA) Participation Report from 2014-2015, only 2% of snowboarders and 7% of alpine skiers were 55 years of age or older. 26 Therefore, assuming that the majority of skiers and snowboarders were younger than 60 years of age, this could explain why our study reported a lower percentage of medial and lateral fractures than prior studies. 26
Also similar to prior population and mountain sports studies, 6,10,13,28,29 younger men were most likely to fracture the clavicle, with a median age of 21 years and an 87.3% male majority. There are several reasons why this may have occurred. First, young men may be more likely to participate in risk-taking activities such as higher speeds, aerial maneuvers, and the use of substances such as alcohol and marijuana 24 while skiing and snowboarding. Furthermore, younger skiers and snowboarders may be more likely to be beginners. 19 Our study additionally did not find a bimodal age distribution of fracture, as reported in many non–snow sports studies. As discussed above, this may be a consequence of older individuals accounting for a smaller proportion of skiers and snowboarders.
Snowboarders sustained 55% of the clavicle fractures, with men accounting for 96% of those snowboarding injuries. In a study by McCall and Safran, 16 snowboarders were overall more likely to sustain an injury compared with skiers. In our study, we found that a much larger number of male snowboarders sustained a clavicle fracture compared with female snowboarders. In addition, we found that more women fractured their clavicle while skiing as opposed to snowboarding. Based on prior studies, it is not surprising that snowboarders were more likely to injure the clavicle as snowboarders injure the upper extremities more frequently than skiers. 4,8,14,16,19,27 This is likely because the lower extremities are strapped in and do not eject the athlete during a snowboarding fall as they do in skiing, leading to more direct falls onto the upper extremities or the upper axial skeleton. According to the SIA Participation Report from 2014-2015, male snowboarders make up about 24% of the total downhill snow sports participants and 60% of the snowboarding participants nationally. 26 However, they account for a much larger percentage of the clavicle fractures in our study. Kim et al 14 found a similar proportion, with 94% of clavicle fractures occurring in men while snowboarding, whereas men made up only 69% of all other snowboarding injuries. Theories for this trend again include increased risk-taking behaviors and more beginner-level athletes in this population. Yamauchi et al 31 found that beginners were at higher risk of snowboarding injury. Pierpoint et al 19,20 found, in the same patient cohort, that 38.9% of snowboarders identified as beginners and 69.6% as either beginners or intermediates.
Of the fractures evaluated, the vast majority were displaced, over half were comminuted, and about 90% were oblique. There is constant debate over the best management, operative versus nonoperative, of clavicle fractures. 21 More data are needed to recommend initial surgical management, 21 and currently, nonsurgical treatment is preferred in the absence of comminution, shortening, or severe displacement. 30 This begs the question of whether more of these fractures ultimately required surgical intervention as the majority were displaced and comminuted. Yet, there is a large degree of variability for measuring clavicle angulation, shortening, and displacement between practitioners without a standardized method of measuring shortening. 2,12 The mean displacement was 13 ± 10 cm with shortening at 10 ± 11 cm. Although many were displaced, shortened, and/or comminuted, based soley on this information, the radiographic features of each fracture would not necessarily qualify the patient for surgery. It is more likely that surgeons would individually review each case and interpret the imaging together with the remainder of the clinical picture. A follow-up study of the final management and outcomes of this cohort could be helpful in determining whether there is any correlation between the imaging and surgical management.
This study has several limitations as it is retrospective and limited by chart review as well as the documentation of the practitioners in the clinic. The radiographs were interpreted by 2 authors and compared with the formal radiologist interpretation. The formal summary by the radiologist often did not cite degree of displacement, angulation, or shortening. The initial chart review grouped injuries by first diagnosis, so it is possible that some clavicle fracture diagnoses may have been missed if this was not the most significant injury sustained when the patient was evaluated at the clinic. 19,20 It is likely that the final values are an underestimate as patients were not included in the study if they refused medical care, were evaluated at an outside facility, or were evaluated only by ski patrol. Many injured patients were from out of state or out of the country. It is possible that similar individuals were not evaluated at the clinic because of concern for cost of medical care. In addition, it should be noted that our study calculates incidence based on participant visits to the resort rather than total exposure time on the slopes. The study lacks external validity for the general population as it included only those who would be able to afford to travel to Winter Park and those physically able to ski or snowboard.
This is one of the few studies to calculate incidence of clavicle fractures treated at a mountainside clinic. It expands upon existing literature by including 5 seasons with a large patient cohort and also stratifies patients into fracture type, sex, injury mechanism, and residence. We feel that the study is an accurate sample of the number of injuries, as the clinic is the only medical center within 32 km (20 miles) of the resort. Importantly, we determined the most likely demographics to sustain clavicle fractures on the mountain. As these fractures are common in both mountain sports and the general population, this study can hopefully be a stimulus for developing prevention strategies. Studies have been conducted on protective gear, including helmets and wrist guards, for other common injuries. 19 While protective equipment may not be practical to reduce the risk of clavicle fracture, it is possible that preventive educational intervention (eg, using appropriate equipment and terrains suitable for skill level) could be helpful. 7,27 As noted above, further studies from this patient cohort could be used to determine which of these patients ultimately required surgical management and whether injuries on the mountain led to more surgeries than those in the general population. Follow-up data could help to prognosticate the need for surgical management when providing patient education at the initial patient visit. This could be important not only from a morbidity standpoint but also as it relates to medical costs.
Conclusion
Clavicle fractures are common, but little data are published on the incidence of these fractures in mountain sports. The incidence of clavicle fractures at the Denver Health Winter Park Medical Center (ski clinic) was 8.4 per 100,000 participant visits to the ski resort. Midclavicle fractures were the most common. The most likely demographics to sustain clavicle fractures were younger patients, snowboarders, and men. Interestingly, male snowboarders accounted for a very large proportion of clavicle fractures as compared with female snowboarders. Few fractures were nondisplaced, and greater than half were comminuted. This study adds winter mountain sports clavicle fracture incidence to the existing data, and these data can be used to direct fracture-prevention strategies. A follow-up prospective study would be helpful to evaluate management and outcomes in this patient cohort.
Footnotes
Acknowledgment
The authors thank the Denver Health Winter Park Medical Center and all team members involved in data collection and interpretation.
Final revision submitted December 7, 2020; accepted January 25, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Colorado Denver (submission ID: CRV005-2).