
Abstract
Background:
Patient-reported outcome measures are important to determine outcomes after orthopaedic procedures. There is currently no standard for outcome measures in the evaluation of patient outcomes after proximal hamstring repair.
Purpose:
To identify and evaluate outcome measures used after proximal hamstring repair.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was performed to identify all English-language articles assessing outcomes after proximal hamstring repair in PubMed, Embase, CINAHL via EBSCOhost, MEDLINE via OvidSP, and Web of Science between 2000 and 2019. After duplicates were removed, studies were selected using eligibility criteria established by the authors. Image reviews, anatomic/histology studies, literature reviews, surgical technique reports, systematic reviews, narrative reviews, case studies, and studies with <5 patients were excluded. Extraction, synthesis, and analysis of outcome measure data were performed using Microsoft Excel. Quality assessment of included studies was performed using Methodological Index for Non-Randomized Studies criteria.
Results:
After duplicate articles were removed, a total of 304 unique articles were identified and 27 met the inclusion criteria. The mean number of patients with proximal hamstring repairs per study was 40. The most frequently reported outcome measures were return to sport (14/27; 51.9%), custom survey/questionnaire (13/27; 48.1%), and isokinetic hamstring strength testing (13/27; 48.1%). Six of the 10 most commonly used outcome measures were validated and included Lower Extremity Functional Scale, 12-Item Short Form Health Survey, visual analog scale for pain, Perth Hamstring Assessment Tool (PHAT), Single Assessment Numeric Evaluation, and Tegner Activity Scale. Of those, PHAT was the only validated outcome measure designed for proximal hamstring repair.
Conclusion:
There is currently no consensus on the best outcome measurements for the evaluation of patients after proximal hamstring repair. We recommend an increased commitment to the use of return to sport, isokinetic strength testing, Lower Extremity Functional Scale, and PHAT when assessing such injuries. Future studies should aim to define the most reliable methods of outcome measurement in this patient population through consistent use of tools that are clinically relevant and important to patients and can easily be employed in a variety of clinical scenarios.
Proximal hamstring avulsions result from forceful eccentric muscle contractions or excessive passive lengthening, which occurs with sudden hyperflexion of the hip with an extended knee (eg, maximum sprinting, hurdling, and water skiing). 4,11 Avulsion injuries often involve the biceps femoris–semitendinosus conjoint tendon and semimembranosus tendon at the ischial tuberosity. These injuries can be classified as complete or incomplete avulsions with or without retraction. 10 When a proximal hamstring tear occurs, patients typically report hearing a loud “pop,” followed by immediate debilitating pain and bruising of the posterior aspect of the thigh. 4 Patients are unable to continue activity at the time of injury and have difficulty moving because of weakness, pain, and limb buckling. 4 Partial or complete avulsions of the proximal hamstring tendons can cause significant and long-term problems, such as ongoing pain when seated, sciatica-type symptoms, functional impairment, and an inability to participate in sporting activities. 4 Compartment syndrome is a less common but serious complication. 1,32 These injuries can be separated into acute, those that present for surgical repair within 4 weeks of injury, or chronic.
Magnetic resonance imaging or ultrasound can be used to confirm an injury to the proximal hamstring tendons. 1 Magnetic resonance imaging more clearly defines the site of the injury, especially in relation to the sciatic nerve. 1 Strains and partial tears with minimal retraction (<2 cm) are often treated nonoperatively, with a combination of physical therapy, nonsteroidal anti-inflammatory drugs, and activity modification. 4,10,29 Complete tears involving all 3 tendons and retraction >2 cm have improved outcomes when operatively treated. 13
Patient-reported outcome measures (PROMs) or clinical outcome measures (COMs) for proximal hamstring injuries, such as patient satisfaction surveys and isokinetic hamstring strength testing, are frequently used to evaluate outcomes after operative management of these injuries. Outcome measures are an important clinical tool in the evaluation of treatment results, as they allow for the objective and subjective comparison of patients. The effective implementation of postoperative outcome measures can provide physicians with valuable information regarding surgical outcomes based on patient demographics, mechanism or chronicity of injury, or type of procedure performed. However, there is currently no consensus on which outcome measures should be used after proximal hamstring repair. Previous studies investigating proximal hamstring repair have used outcome measures that were nonspecific, nonvalidated, or both. 10 This poor standardization and lack of validated, injury-specific tools to assess these patients are possible hindrances to future research and evaluation of novel surgical techniques. 9 The purpose of this study was to conduct a systematic review of the literature to identify and evaluate outcome measures used for proximal hamstring repair of acute and chronic proximal hamstring injuries.
Methods
A systematic review was performed of all English-language published studies evaluating proximal hamstring injuries managed operatively between January 1, 2000, and April 31, 2019. Following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, a broad literature search was performed using PubMed, Embase, CINAHL via EBSCOhost, MEDLINE via OvidSP, and Web of Science databases on May 1, 2019. Three keywords and their related synonyms were used in the search: proximal (“origin” and “ischial tuberosity”), hamstring (“hamstring muscle[s],” “biceps femoris,” “femoral biceps,” “semimembranosus,” “semitendinosus,” and “hamstring tendon[s]”), and repair (“surgery,” “surgical repair,” “operative treatment,” “surgical treatment,” and “procedure”) (Appendix Table A1). The Boolean command “OR” was used to combine the synonyms, and the categories were linked using the Boolean command “AND.” The terms were identified in the title or abstract, and no restrictions were set in the search field.
Inclusion/Exclusion Criteria
Studies were included if they (1) involved confirmed diagnosis and surgical repair of a proximal avulsion of the biceps femoris, semimembranosus, semitendinosus, or any combination thereof; (2) employed a PROM or COM system; (3) included ≥5 patients; and (4) included acute, chronic, or both acute and chronic proximal hamstring injuries. Studies were excluded if they were image reviews, anatomic/histology studies, literature reviews, surgical technique reports, systematic reviews, narrative reviews, case studies, or articles for which an English full text was unavailable.
Data Collection
Articles were screened via title or abstract to determine inclusion or exclusion status. Duplicate studies were removed. Abstracts were screened by 2 reviewers (A.P.-C. and T.E.R.) to create a list of all outcome measures. Relevant studies then underwent full-text review. All included studies were reviewed by a minimum of 2 authors. After full-text review of the 27 selected articles, the reference sections were reviewed to identify any other relevant citations and the article that introduced each outcome measure, if available.
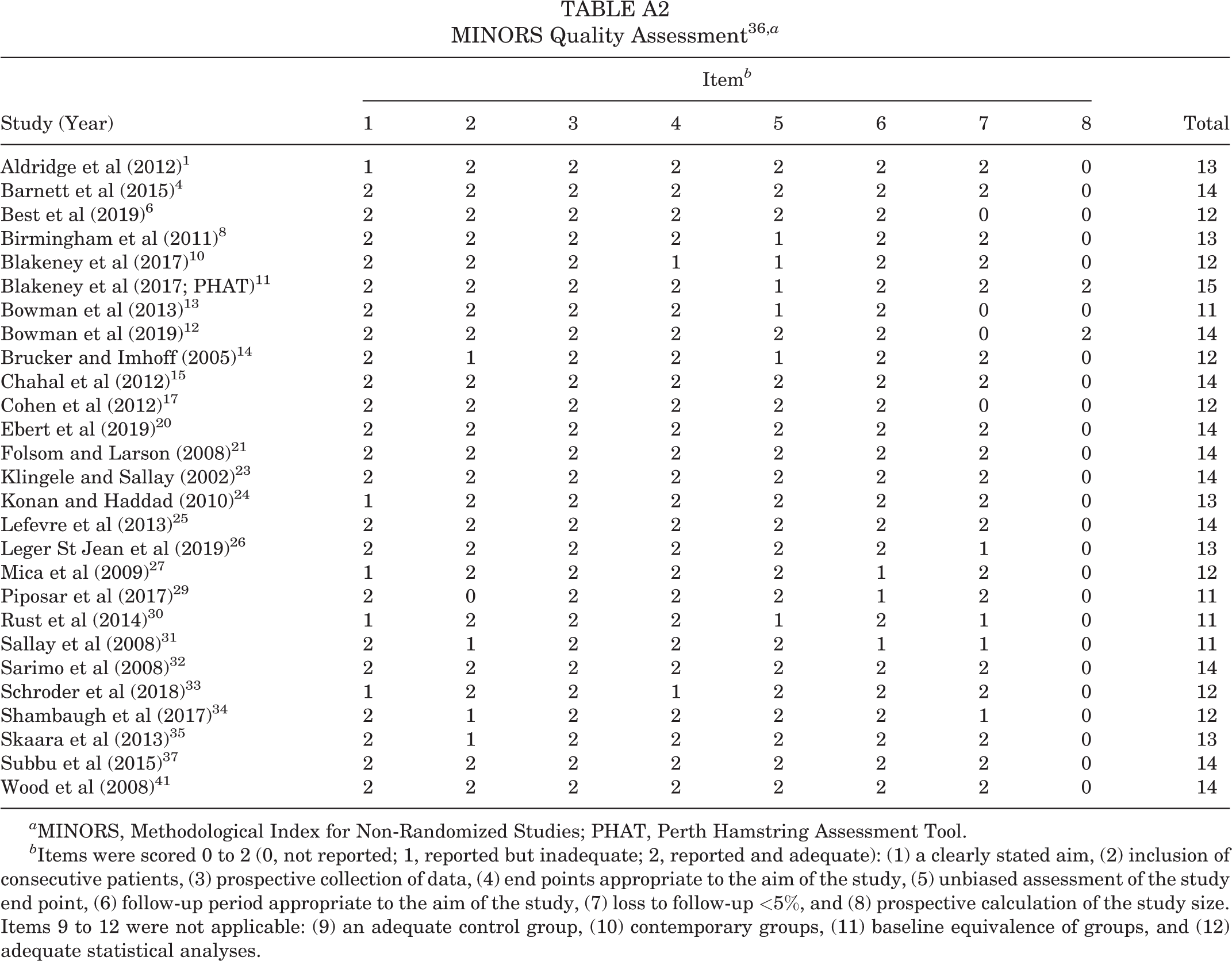
All study data were extracted, synthesized, and recorded using an electronic database program (Excel Version 16.0; Microsoft Corp). Information about specific outcome measures was acquired from the original article and/or Google search and included acronym, intended measurement concept, number of items, and score. Quality assessment of the studies was performed using Methodological Index for Non-Randomized Studies (MINORS) (Appendix Table A2). 36 There are 12 items on the MINORS checklist; items are given a score of 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate). 36 The ideal score is 24 for comparative studies and 16 for noncomparative studies, like those in this review. 36 Synthesized data were presented using descriptive statistics.
Bias
Bias was not evaluated in the individual studies because the goal was to assess the outcome measures used in all published literature.
Subanalyses
The mean number of outcomes measured was based on all included studies. Mean age and follow-up were assessed using weighted means with the number of patients in each study. The journal impact factor (<3 vs ≥3) and total number of outcome measures were compared using an unpaired t test (α = .05). The cutoff for an impact factor of 3 was used, as it is the closest whole number halfway between 0 and our maximum impact factor. Furthermore, higher-level journals tended to have impact factors >3. Impact factors were extracted from the 2019 Journal Citation Report, published by Clarivate Analytics. 16
Results
The initial literature search yielded 2368 studies. After removal of duplicates and review of titles, 2064 studies were excluded. An additional 268 studies were excluded after abstract review. Of the 36 remaining studies, 4 were excluded because an English translation was not available, and 5 articles could not be obtained, leaving 27 for inclusion in the systematic review (Figure 1). One article by Shambaugh et al 34 discussed operative and nonoperative management of proximal hamstring repair; however, only data from patients treated operatively were included in analysis. Quality assessment of studies per the MINORS criteria demonstrated a mean score of 12.9 (range, 11-15). Given the nature of the clinical research, all included studies had a reduced quality assessment score owing to a lack of control groups, patient groups representative of the general population, and in-depth statistical analysis of data, making their ideal score 16. The largest discrepancies in quality assessment score resulted from patients lost to follow-up and organization of the research study, such as a clear statement of study aims or inclusion and exclusion criteria. While no study had an ideal score, resulting MINORS scores indicated low risk of bias in the majority of studies. Tables 1 and 2 detail the 27 studies reporting on 1080 patients and the outcome measures used. §
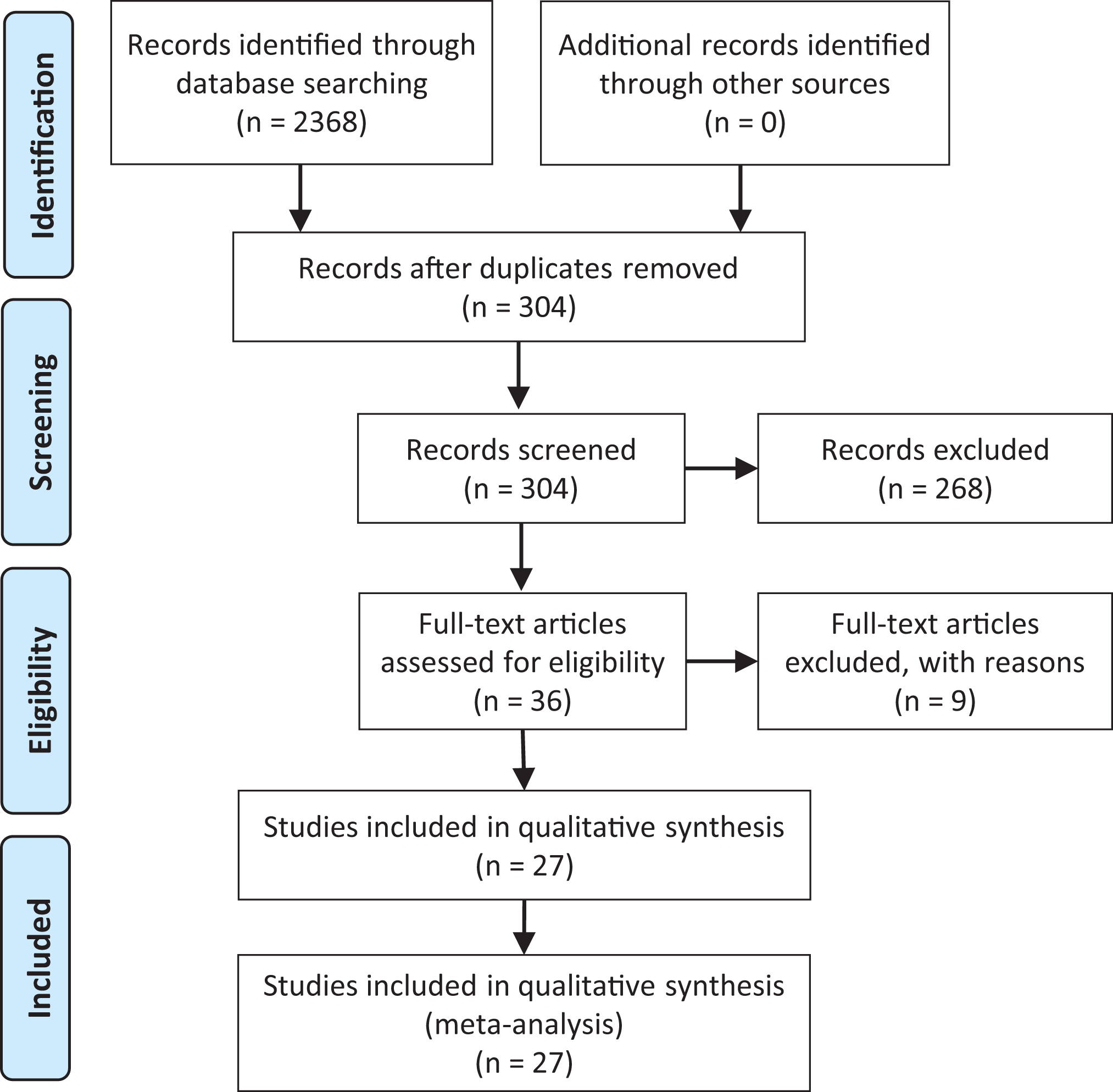
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) search strategy and selection of articles.
Characteristics of Included Studies a

a Dashes indicate not reported. AKE, active knee extension; c-LEFS, custom Lower Extremity Functional Scale; c-Marx, custom Marx Activity Scale; GMWT, Groningen Meander Walking Test; iHOT-12, International Hip Outcome Tool–12; KJOC, Kerlan-Jobe Orthopaedic Clinic; LEFS, Lower Extremity Functional Scale; Marx, Marx Activity Scale; M/F, male/female; MRI, magnetic resonance imaging; PHAT, Perth Hamstring Assessment Tool; PHIQ, Proximal Hamstring Injury Questionnaire; RTS, return to sports; SANE, Single Assessment Numeric Evaluation; SF-12, 12-Item Short Form Health Survey; TAS, Tegner Activity Scale; UCLA, University of California, Los Angeles; VAS, visual analog scale for pain.
b Median.
Patient and Follow-up Information for the Included Studies

a Number of studies with information necessary for calculation.
The mean number of patients per study was 40 (range, 6-132), with a mean weighted patient age of 42.8 years (range, 29-59.1). The mean follow-up was 37.2 months (range, 20-68.4), and 26 studies cited patient sex: 44.2% female (449/1016) and 55.8% male (567/1016).
Outcome Measures
Thirty outcome measures were identified (Table 3): 17 (56.7%) PROMs and 13 (43.3%) COMs. On average, 4.1 (range 1-11) outcome measures were used per study. Of 27 articles, 14 (51.9%) used return to sport (RTS); 13 (48.2%), a custom survey/questionnaire; and 13 (48.2%), isokinetic strength testing (Table 2). §
Reporting of Outcome Measures (N = 27 Studies) a
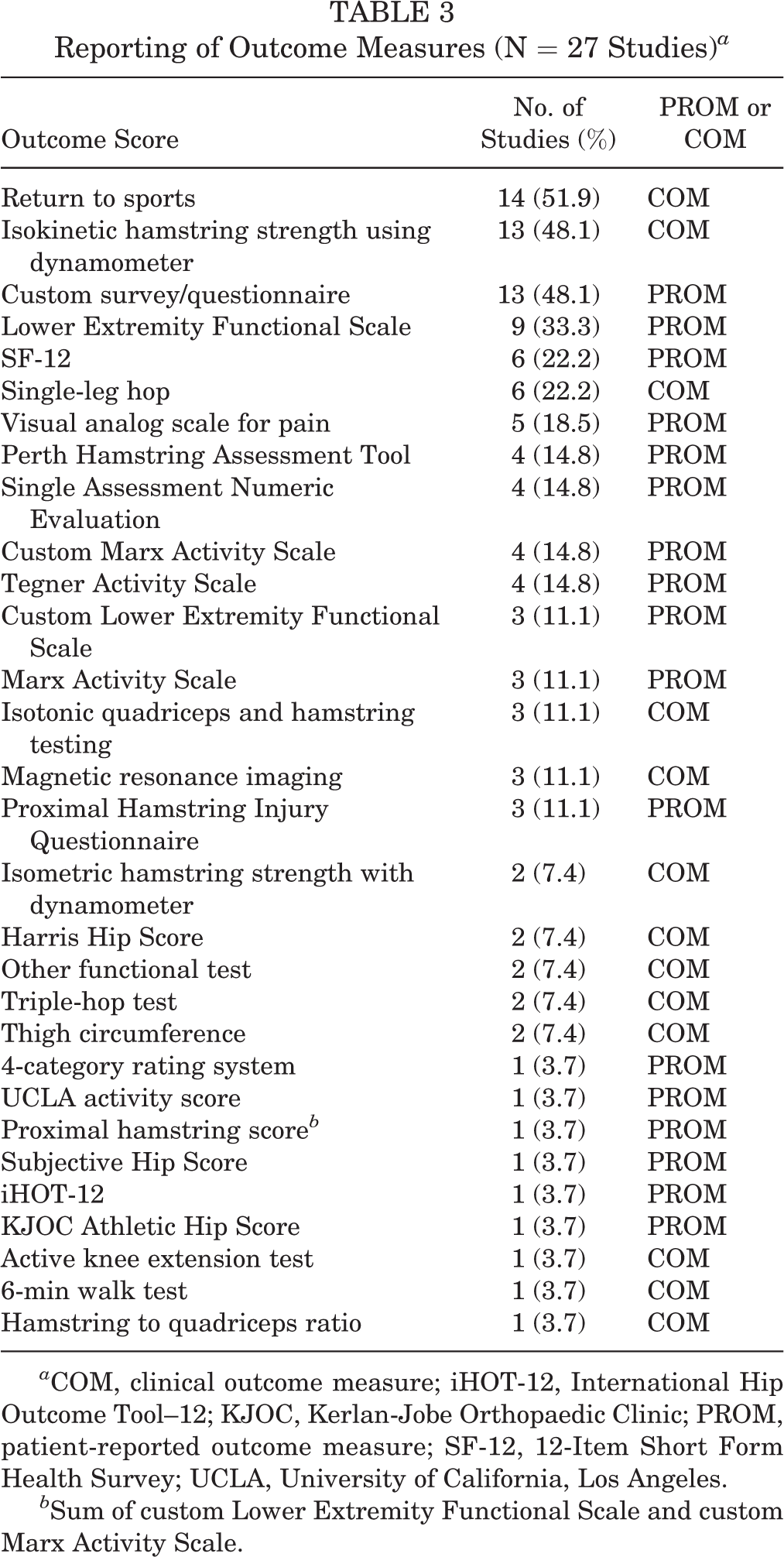
a COM, clinical outcome measure; iHOT-12, International Hip Outcome Tool--12; KJOC, Kerlan-Jobe Orthopaedic Clinic; PROM, patient-reported outcome measure; SF-12, 12-Item Short Form Health Survey; UCLA, University of California, Los Angeles.
b Sum of custom Lower Extremity Functional Scale and custom Marx Activity Scale.
Validated Outcome Measures
Of the 10 most frequently used outcome measures, 6 (60%) have been validated: Lower Extremity Functional Scale (LEFS), 12-Item Short Form Health Survey (SF-12), visual analog scale for pain (VAS), Perth Hamstring Assessment Tool (PHAT), Single Assessment Numeric Evaluation (SANE), and Tegner Activity Scale (TAS). Of the 6 validated outcome measures, LEFS has the greatest number of items (n = 20), while SANE, TAS, and VAS have the least number of items (n = 1) (Table 3). PHAT is the only validated outcome measure designed to evaluate patients with proximal hamstring ruptures pre- and postoperatively (Table 4). 10,11
Characteristics of Most Used Validated Outcome Measures After Proximal Hamstring Repair

Journal Impact Factor
When articles in journals with an impact factor <3 were compared with those with an impact factor ≥3, there was a statistically significant difference in mean sample size (21.5 vs 45.4, respectively; P = .01). There was no statistically significant difference between these groups by number of outcome scores reported, mean follow-up, or mean age of patients (Table 5).
Influence of Journal Impact Factor

No statistically significant difference was found in mean age, impact factor, or mean sample size between studies that used <4 outcome measures and those with ≥4 (Table 6) and the journal in which they were published. Thus, the use of more or fewer outcome measures was not associated with publication in a journal with a higher impact factor. Of the studies, the most frequently used number of outcome measures in the assessment of proximal hamstring repair was 2 (Figure 2).
Comparison of Number of Outcome Measures Used


Number of outcome measures reported by included studies.
Discussion
A lack of consistency in the use of outcome measurements makes it difficult to gather sufficient data and extrapolate study results that could be used to improve patient management. This study demonstrates substantial variability and inconsistency of outcome measures used after proximal hamstring repair.
In the 27 articles reviewed, 30 outcome measures were reported, including COMs and PROMs, but with no consensus or recommendations regarding the best measurements for evaluating outcomes. § The most-used validated outcome measures were PHAT, LEFS, SF-12, VAS, SANE, and TAS. 7,11,18,28,39,40 PHAT was the only validated outcome measure designed to evaluate proximal hamstring tendon repair. 11 When comparing articles in journals with an impact factor <3 and ≥3, we found no statistically significant difference in the number of outcome scores reported, patient-follow up, or mean age of patients. However, studies published in journals with a higher impact factor included a larger number of patients (45.4) than those with a lower impact factor (21.5). This relationship was statistically significant (P = .01) and demonstrates the increased power of a study that has a greater number of patients and the likelihood that those studies are published in a more reputable journal.
Most studies used a combination of COMs and PROMs, as is common practice in outcome measures after orthopaedic procedures. Of the 27 studies, 6 (22.2%) reported difficulty when choosing an outcome measure to use because, at that time, there was no outcome tool designed for the assessment of proximal hamstring injuries. 3,4,8,13,26,31 Other studies (4/27; 14.8%) discussed their use of a nonvalidated questionnaire and the limitations that come with this method of evaluating patient outcomes. 8,13,26,38 Van der Made et al 38 published a systematic review of patient outcomes after surgical repair of proximal hamstring avulsions. This review comprised 13 studies (387 participants) in which all patients underwent surgical repair of proximal hamstring avulsion. The authors found good subjective outcomes in these patients with incomplete restoration of function and level of activity, but they noted that the heterogeneity of outcome measures used in clinical practice limited their results and ability to accurately and consistently study patient outcomes.
In a post hoc analysis, Chahal et al 15 reviewed 13 patients who underwent surgical repair for complete proximal hamstring avulsions. Postoperative outcomes were measured using SANE, VAS, Proximal Hamstring Injury Questionnaire, LEFS, Harris Hip Score (HHS), and TAS. Of these 6 outcome measures, HHS was the only COM. The authors determined that the HHS and LEFS had a robust ceiling effect, meaning that a large proportion of their patients received a maximum score. This led the authors to believe that these outcome measures could not reliably differentiate among patients postoperatively with varying levels of hamstring injury or recovery. 15,27
Clinical Outcome Measures
COMs were more frequently used than PROMs, as the results indicate; specifically, RTS and isokinetic strength testing were among the top 3 most commonly used outcome measures after these injuries. RTS is limited by its definition and requires further study before it can serve as a consistent measurement of outcomes after proximal hamstring repair. The use of RTS as an outcome measure is also limited by the fact that many patients are not part of an athletic or highly active population. This outcome may not be applicable to patients who participate in lower-demand activity and are injured outside of athletic activity. However, RTS is useful in the ease at which it can be implemented and its relatedness to postoperative patient expectations. Isokinetic strength testing serves as an objective measurement providing quantitative data for interpretation by clinicians. Isokinetic muscle testing quantifies the return of strength in the injured extremity as compared with the uninvolved extremity, often testing for knee extension and flexion at 180 deg/s and 60 deg/s. 21 This measurement has been shown to be a reliable tool in the evaluation of strength after knee flexor injuries. 22
When using a nonvalidated PROM such as a questionnaire, clinicians usually complement the PROM with a COM, such as isokinetic testing, to evaluate the accuracy of the nonvalidated PROM. Birmingham et al 8 studied functional outcome after repair of proximal hamstring avulsions in 23 patients with acute or chronic injury. They used Spearman correlations between components of their nonvalidated questionnaire and isokinetic testing to determine if their objective test correlated well with the patient-reported questionnaire, and they found that repair yielded good subjective and objective functional results in these patients.
Patient-Reported Outcome Measures
Among the 10 most-used outcome measures that were identified, PHAT, LEFS, SF-12, VAS, SANE, and TAS, are validated PROMs. 7,11,18,28,39,40 The most frequently used PROM was custom survey/questionnaire. PHAT is one of the few validated outcome measures tailored to proximal hamstring tendon repair, as opposed to measures that apply to a broad scope of lower limb or musculoskeletal injuries. 11 PHAT was used in 4 studies 6,10,11,20 ; however, 2 of these were written by the same author, 10,11 which creates a risk of bias.Further research is needed to determine if PHAT should be implemented widely to evaluate outcomes in patients after proximal hamstring repair.
In 2013, Bowman et al 13 studied the outcomes of 14 patients with partial tears of the proximal hamstring. Each patient was treated with open debridement and primary tendon repair after failure of nonoperative management. In the evaluation of these patients, the authors utilized LEFS and the Marx Activity Scale PROMs to study the results of surgical repair. Additionally, they generated a custom Marx Activity Scale and custom LEFS score adapted from previously validated questionnaires. Bowman et al 13 reported no subsequent surgery and no disability in activities of daily living in the operative extremity in any of their patients. This study demonstrates satisfactory functional outcomes, return to activity, and a low complication rate in patients undergoing proximal hamstring tendon repair. This study is one of a few articles in this review that did not use a COM; the authors discussed this as a limitation to their study.
The current study demonstrates the lack of uniformity in the measurement of outcomes in patients with proximal hamstring injuries. The 27 studies included in this review demonstrated significant variability in both number and type of outcome measures used. COMs were more frequently used than PROMs, with RTS and isometric strength testing being the most commonly used outcome measurements among the 27 studies. The most frequently used patient-reported tool was custom survey/questionnaire, while the most frequently used validated PROM was LEFS.
Based on the results of this review, the following outcome measures seem most accurate in evaluating patients after proximal hamstring repair: RTS and isokinetic strength testing (COMs) and PHAT (PROM). RTS serves as a COM that is easily utilized in practice. Additionally, RTS is a functional outcome that is often important to patients in the postoperative period. Isokinetic strength testing has been shown to accurately evaluate recovery in proximal hamstring injuries. It can also serve as a second objective COM in the evaluation of these patients. 22 PHAT is one of few recently developed and validated outcome measurements designed for proximal hamstring injuries. This survey provides a score based on functional outcomes that considers pain scores at rest and during daily activity and return to activities, such as sitting, driving a car, running, and ability to play full sport. Additionally, LEFS is a reliable patient-centered measurement commonly used by studies in this review. It is the most frequently used PROM behind custom surveys, implying that physicians should be able to apply it to common clinical practice. Chahal et al 15 proposed that LEFS may possess a ceiling effect; however, this study involved a small patient population (13 patients) and may not have been adequately powered to show a statistically significant effect. Further evaluation of patient outcomes using LEFS will help to provide a better understanding of its internal validity; however, results of prior studies demonstrate some question regarding its utility in the evaluation of proximal hamstring injuries. If combined and implemented uniformly, use of RTS, isokinetic strength testing, PHAT, and perhaps LEFS could provide more insight in the management of hamstring injuries. In recent years, the Patient-Reported Outcomes Measurement Information System (PROMIS) tools from the US National Institutes of Health have been employed to evaluate orthopaedic injuries. Specifically, PROMIS has been used to evaluate outcomes of shoulder and knee injuries with the goal of providing a well-studied standardized PROM. 2,5,19 However, these tools have not been used to evaluate outcomes after proximal hamstring injuries. Future research should evaluate different PROMIS tools for their validity and ease of implementation in the evaluation of proximal hamstring injuries.
Limitations
There are several limitations to this study. While a thorough literature review utilizing 6 databases was performed, it is possible that if more databases had been searched, additional articles may have been identified. Several studies were conducted by the same institution, which may introduce bias. Furthermore, studies interpreting the use of outcome measurements are often affected by publication bias, as data regarding poor outcome measurements are not widely reported. The variability in definition of RTS makes it difficult to use this as a reliable measure of outcome after proximal hamstring repair. Custom surveys and questionnaires in this study were nonvalidated since they were developed by physicians and/or researchers in individual studies. Finally, no comments were made on the severity of injuries cited in the studies. It is unclear if some COMs and PROMs were used more often because of their accuracy in evaluating recovery from injuries of a particular severity. To this point, there was no difference in the evaluation of acute versus chronic proximal hamstring injuries in studies that examined both. Therefore, we were unable to draw conclusions regarding the differences in the evaluation of these injuries. Greater detail regarding injury severity and chronicity may be helpful in defining which outcome measurement tools are more effective for different types of hamstring injuries.
Conclusion
There is currently no consensus on outcome measurements that should be used in the assessment of patient satisfaction and surgical outcomes after proximal hamstring repair. Among the most frequently used in the literature are RTS (COM), custom surveys (PROM), and isokinetic strength testing (COM). Of the PROMs specific to proximal hamstring injury, only PHAT is validated. Our recommendation is an increased commitment to the use of isokinetic strength testing and RTS as standard COMs, when applicable, and LEFS and PHAT as PROMs in evaluation of proximal hamstring repair. Future studies should assess the time points in patient recovery and the functional parameters that define RTS in the context of proximal hamstring injuries. Researchers should also seek to identify differences in the evaluation of acute versus chronic injury and partial- versus full-thickness proximal hamstring tears. Additionally, research should evaluate the pragmatism of each outcome measure when implemented in clinical practice. Finally, the accuracy and quality of these individual outcome measures should continue to be assessed in an attempt to gather a consensus on the best tools used in the setting of proximal hamstring repair.
Footnotes
Final revision submitted November 12, 2020; accepted December 14, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.K.M. has received education payments from Arthrex Inc, Alon Medical Technology, and Quest Medical; nonconsulting fees from Arthrex Inc; and hospitality payments from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Notes
Appendix
MINORS Quality Assessment 36 ,a
| Item b | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study (Year) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Total |
| Aldridge et al (2012) 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 13 |
| Barnett et al (2015) 4 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 14 |
| Best et al (2019) 6 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 12 |
| Birmingham et al (2011) 8 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 0 | 13 |
| Blakeney et al (2017) 10 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 0 | 12 |
| Blakeney et al (2017; PHAT) 11 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 15 |
| Bowman et al (2013) 13 | 2 | 2 | 2 | 2 | 1 | 2 | 0 | 0 | 11 |
| Bowman et al (2019) 12 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 14 |
| Brucker and Imhoff (2005) 14 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 0 | 12 |
| Chahal et al (2012) 15 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 14 |
| Cohen et al (2012) 17 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 12 |
| Ebert et al (2019) 20 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 14 |
| Folsom and Larson (2008) 21 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 14 |
| Klingele and Sallay (2002) 23 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 14 |
| Konan and Haddad (2010) 24 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 13 |
| Lefevre et al (2013) 25 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 14 |
| Leger St Jean et al (2019) 26 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 0 | 13 |
| Mica et al (2009) 27 | 1 | 2 | 2 | 2 | 2 | 1 | 2 | 0 | 12 |
| Piposar et al (2017) 29 | 2 | 0 | 2 | 2 | 2 | 1 | 2 | 0 | 11 |
| Rust et al (2014) 30 | 1 | 2 | 2 | 2 | 1 | 2 | 1 | 0 | 11 |
| Sallay et al (2008) 31 | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 0 | 11 |
| Sarimo et al (2008) 32 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 14 |
| Schroder et al (2018) 33 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 0 | 12 |
| Shambaugh et al (2017) 34 | 2 | 1 | 2 | 2 | 2 | 2 | 1 | 0 | 12 |
| Skaara et al (2013) 35 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 0 | 13 |
| Subbu et al (2015) 37 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 14 |
| Wood et al (2008) 41 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 14 |
a MINORS, Methodological Index for Non-Randomized Studies; PHAT, Perth Hamstring Assessment Tool.
b Items were scored 0 to 2 (0, not reported; 1, reported but inadequate; 2, reported and adequate): (1) a clearly stated aim, (2) inclusion of consecutive patients, (3) prospective collection of data, (4) end points appropriate to the aim of the study, (5) unbiased assessment of the study end point, (6) follow-up period appropriate to the aim of the study, (7) loss to follow-up <5%, and (8) prospective calculation of the study size. Items 9 to 12 were not applicable: (9) an adequate control group, (10) contemporary groups, (11) baseline equivalence of groups, and (12) adequate statistical analyses.