
Abstract
Background:
The association between participating in sport and osteoarthritis is not fully understood.
Purpose:
To investigate the association between osteoarthritis and participating in sports not listed in previous reviews: American football, archery, baseball, bobsleigh, curling, handball, ice hockey, shooting, skeleton, speed skating, and wrestling.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
We searched 4 electronic databases and hand searched recent/in-press editions of relevant journals. The criteria for study selection were case-control studies, cohort studies, nested case-control studies, and randomized trials with a control group that included adults to examine the effect of exposure to any of the included sports on the development of osteoarthritis.
Results:
The search returned 6197 articles after deduplication. Nine studies were included in the final review, covering hip, knee, and ankle osteoarthritis. There were no studies covering archery, baseball, skeleton, speed skating, or curling. The 6 sports included in the review were analyzed as a collective; the results of the meta-analysis indicated that participation in the sports analyzed was associated with an increased risk of developing osteoarthritis of the hip (relative risk [RR] = 1.67 [95% confidence interval (CI), 1.15-2.41]; P = .04), knee (RR = 1.60 [95% CI, 1.23-2.08]; P < .001), and ankle (RR = 7.08 [95% CI, 1.24-40.51]; P = .03) as compared with controls. Meta-analysis suggested a significantly increased likelihood of developing hip osteoarthritis through participating in wrestling (RR = 1.78 [95% CI, 1.20-2.64]; P = .004) and ice hockey (RR = 1.70 [95% CI, 1.27-2.29]; P < .001), while there was no significant difference through participating in handball (RR = 2.50 [95% CI, 0.85-7.36]; P = .10). Likelihood of developing knee osteoarthritis was significantly increased in wrestling (RR = 2.22 [95% CI, 1.59-3.11]) and ice hockey (RR = 1.52 [95% CI, 1.18-1.96]; both P < .002). According to the meta-analysis, shooting did not have a significant effect on the RR of knee osteoarthritis as compared with other sports (RR = 0.43 [95% CI, 0.06-2.99]; P = .39).
Conclusion:
The likelihood of developing hip and knee osteoarthritis was increased for ice hockey and wrestling athletes, and the risk of developing hip osteoarthritis was increased for handball athletes. The study also found that participation in the sports examined, as a collective, resulted in an increased risk of developing hip, knee, and ankle osteoarthritis.
Osteoarthritis is the most common form of arthritis and one of the leading causes of pain and disability worldwide. 5,10,19,23,31,49,70,91 It is a chronic condition with a range of disorders that result in functional and structural failure of synovial joints, with a loss and erosion of articular cartilage, meniscal degeneration, subchondral bone alteration, a synovial inflammatory response, and bone and cartilage overgrowth. 43,100 Osteoarthritis is characterized by pain, stiffness, impaired function and range of movement, plus reduced quality of life, which contributes to functional disability. §
The cause of osteoarthritis remains largely unknown, although substantial progress has been made over recent decades. 88,90 Previous research 8,9,11,29,51,52,89 has identified several risk factors such as joint injury, muscle weakness, hormonal factors, nutrition, obesity, occupational activity level, and mechanical stress or loading of the joints. Similarly, factors such as age, sex, ethnicity, and genetics have been shown to influence osteoarthritis. 30,35,46,52,90,100
Several national guidelines have encouraged exercise as a frontline intervention in the management of osteoarthritis. 17,81,101 This is based on the principle that exercise can increase joint stability and flexibility plus reduce pain, thus optimizing functional capacity and independence. 81 Previous research has supported this by showing that exercise significantly improves pain and function. 17,81,101 Additionally, sport and exercise have demonstrated global health benefits, such as bone health, cardiovascular function, energy metabolism, insulin action, and psychological status. 56,63,65,81,97 Similarly, sports and exercise provide pleasure and entertainment for many people. 11 Unfortunately, vigorous physical activity has been found to increase the risk of injury, including joint injuries that can damage joint structures such as menisci, ligaments, and articular cartilage. 11,13,18
The association between participating in sport and osteoarthritis is not fully understood. Tran et al 89 conducted a systematic review into the relationship of osteoarthritis and the 32 most popular sports in England by participation. They found that overall sports participation increased the risk of developing osteoarthritis, but the risk differed by individual sports. We can conclude that the relationship between sports participation and osteoarthritis remains complicated, and further research is needed to develop the field. However, the review did not include some popular and Olympic sports—namely, American football, archery, baseball, handball, wrestling, shooting, bobsleigh, curling, ice hockey, skeleton, or speed skating. Similarly, there has been no other systematic review exploring the effects of these sports.
Research investigating the association between participating in popular sports, such as American football and baseball, and osteoarthritis has been advocated by Wolf and Amendola, 98 stating that there is no good evaluation of rates of osteoarthritis in popular sports such as American football and baseball. The importance was emphasized by previous research suggesting that participating in American football increases the frequency of degenerative changes in multiple joints, 12,68,74 possibly attributed to injuries. 11 Previous research has suggested that baseball pitchers have higher risks of osteoarthritis of the shoulder and elbow. 1,7 Likewise, previous research has stated that American football, baseball, handball, and ice hockey are all sports with high estimated intensity of joint impact and torsional loading; as a result, these are sports predicted to raise the risk of osteoarthritis, 11,13,24,51,55,62,90 which emphasizes the importance of these sports being examined. Participating in wrestling may increase the risk of premature osteoarthritis because of the high body mass and heavy weight training, which cause excessive loading on the weightbearing joints. 51,52 Previous studies have found that American football, baseball, handball, wrestling, bobsleigh, ice hockey, short-track speed skating, and skeleton are associated with a high risk of sustaining an injury, 3,21,22,26,27,72,73 thus making them all potential high-risk factors for developing osteoarthritis given that joint injuries have been identified as a risk factor for osteoarthritis. 8,9,89
Consequently, the current systematic review aimed to examine the association between osteoarthritis (all joints) and participation in sports not included in previous reviews: American football, archery, baseball, handball, wrestling, shooting, bobsleigh, curling, ice hockey, skeleton, and speed skating. We hypothesized that there would be no difference in association of osteoarthritis among sports.
Methods
The current review adopted recommendations by the Cochrane Collaboration 41 and those published in the American Journal of Sports Medicine. 39 The study’s protocol was registered on the PROSPERO database (CRD42017057561).
Search Strategy
Four electronic databases were searched: Embase via OvidSP, SPORTDiscus via EBSCOhost, PEDro via Physiotherapy Evidence Database, and MEDLINE via OvidSP (see Table 1 for search terms). Searches were not limited by date or language. These database searches were augmented by hand searching citations in identified reviews and the contents of recent/in-press editions of relevant journals published December 2016, January 2017, February 2017, March 2019, April 2019, and May 2019 (American Journal of Sports Medicine, British Journal of Sports Medicine, Journal of American Medical Association, Journal of Bone and Joint Surgery, and Osteoarthritis and Cartilage). This review did not consider gray literature. Translators were sought for non-English references. The searches took place February 2017 and were updated May 2019, and results were imported into and deduplicated using EndNote X7 (Thomson Reuters).
Search Terms for Ovid MEDLINE

Study Selection
Two reviewers used the prespecified inclusion and exclusion criteria to independently assess each reference using a 3-stage process. The first stage was to review titles; the second, to review abstracts; and the third, to review the full text of potentially eligible articles. The studies that met the inclusion criteria on full-text assessment were included in the final review. Discrepancies about articles were settled by discussion between the reviewers or by consultation with a third author (T.B.-S., O.S.I, R.G.P., or K.L.E.).
Eligible studies were case-control studies, cohort studies, nested case-control studies, and randomized trials that included adult participants (aged ≥18 years); measured exposure to any form of the sports of interest (American football, archery, baseball, bobsleigh, curling, handball, ice hockey, shooting, skeleton, speed skating, or wrestling) at any level; had a comparator group; and evaluated any of the following outcomes: diagnosis of osteoarthritis, radiographic markers of osteoarthritis, arthroplasty of any joint, self-reported chronic pain, and associated disability. Comparator groups could incorporate exposure to other sports, untrained participants without regular sporting exposure, or military cohorts.
Studies were excluded if the sport could not be identified independently owing to participants’ exposure to a combination of sports or if the time between exposure to the sport of interest and the outcome was inadequate (a minimum of 1 year). Retrospective cohorts, defined as those in which previous exposure to the sport of interest was established at recruitment, were eligible. Animal studies, studies that involved amputees of the limb that was affected by osteoarthritis, case series (with no comparator), and case reports were excluded.
Data Extraction
This study adhered to the PRISMA checklist (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). A single reviewer (T.B.S.) used a prepiloted extraction form to extract data, which were checked by a second reviewer (K.L.E.). When a study was found multiple times, the most recent results for each outcome were extracted. When a study comprised >1 comparator, each was reviewed.
The following data were extracted: sport in which individuals participated, level at which participants performed, sample size, age, sex, anatomic joints assessed, follow-up period, diagnosis of osteoarthritis, and prevalence of osteoarthritis. The performance level was dichotomized as elite or nonelite. As there is no 1 definition of “elite” across these multiple sports, this review classified elite as either national- or international-level sporting activity or professional participation in the sport.
Data Synthesis
All eligible studies were included in a narrative synthesis, organized by study design, sport, joint, and outcome. Measurement effects were expressed as relative risk (RR) with 95% confidence intervals (CIs). For studies 38,60 that did not present their results as RR, the RR was calculated.
Because of the observational nature of cohort studies, a random effects model was conducted using the Mantel-Haenszel method of weighting. 61 All rates entered were crude (unadjusted). We did not account for missing data. Meta-analyses were performed using Review Manger (Version 5.3), 15 for all sports collectively by joint and then by individual sport.
Risk of Bias
The Newcastle-Ottawa scale was used to assess the risk of bias for each eligible observational study. 96 Each study was independently assessed by 2 reviewers (T.B.S., O.S.I.). Discrepancies in ratings were resolved through consensus or consultation with a third author (K.L.E.). The results were determined using the thresholds for conversion of the Newcastle-Ottawa Scale to standards per the Agency for Healthcare Research and Quality (poor, fair, or good). 94 Risk of bias was not used as a basis to exclude studies. The possibility of publication bias cannot be excluded. Funnel plots were not undertaken because there were too few studies in the meta-analysis. 85
Heterogeneity
Statistical heterogeneity was measured using the I 2 statistic, where I 2 >75% indicated considerable heterogeneity; 50% to 75%, substantial heterogeneity; and <50%, limited heterogeneity. 40,77
Results
The search strategy results according to the PRISMA guidelines 67 are summarized in Figure 1. The search strategy resulted in 6197 deduplicated potentially eligible citations. After review of titles, abstracts, and full texts, the search culminated in 9 eligible studies, which were included in the full review.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of search results.
Study Characteristics
Study characteristics are summarized in Table 2. All 9 studies in the present review were retrospective cohort studies and were located in Canada, Finland, France, Sweden, Switzerland, and the United States. Of the 9 studies, 4 examined ice hockey (covering hip, knee, and ankle osteoarthritis) 47,51,87,90 ; 2, American football (knee, ankle, foot) 68,92 ; 2, handball (hip, knee) 53,90 ; 2, shooting (hip, knee) 47,52 ; 2, wrestling (hip, knee, ankle) 47,51 ; and 1, bobsleigh (hip). 63 Three of the 9 studies examined multiple sports: handball and ice hockey 90 ; wrestling and ice hockey 51 ; shooting, wrestling, and ice hockey. 47 Consequently, 6 of the 11 previously unreviewed sports (ice hockey, wrestling, handball, shooting, American football, bobsleigh) were included in this review; no study examined the effects of the remaining 5 sports (archery, baseball, curling, skeleton, or speed skating).
Table 2. Characteristics of the Included Studies a

a EOS, elite other sports; ICD, International Classification of Diseases; M, military; O, other.
b Mean age cited where reported.
Five (56%) studies assessed single joints: 2 hip 53,63 and 3 knee. 52,68,87 The remaining 4 (44%) studies examined multiple joints: hip and knee 47,90 ; ankle and foot 92 ; and hip, knee, and ankle. 51 No other joints were examined.
Five studies 47,51,52,63,90 included former elite athletes of other sports as the comparators, 2 of which had comparators from the military. 47,51 Six studies had comparator groups who had never played the focus sport 53,68,87,92 or were healthy and/or untrained (both had former elite comparators). 63,90
There was no outcome common to all 9 studies. Three studies cited a diagnosis of osteoarthritis: physician diagnosis, 90 self-reported questionnaire that included items on physician-diagnosed osteoarthritis, 47 and International Classification of Diseases codes used to form the diagnostic categories of osteoarthritis. 51 The other 6 studies 52,53,63,68,87,92 measured markers of osteoarthritis on radiographs. No studies reported on arthroplasty of any joint, self-reported chronic pain, or associated disability.
The mean age of participants, where indicated, ranged from 23 years 92 to 70 years. 47 The follow-up period ranged from none (ie, cross-sectional data 53,87,92 ; but with at least 12 months between exposure and outcome owing to the retrospective nature of the cohort) to 20 years. 51,68 Sample sizes of the studies ranged from 34 football players 68 to 3452 athletes, 51 with 3 of the 9 studies citing small samples (<100). 53,63,68 Of the 9 studies, 8 reported data only on male participants. Accordingly, for this review, just the male data were utilized from the study including male and female participants. 87
Risk of Bias
All studies for each focus sport were deemed good according to the Agency for Healthcare Research and Quality selection categories (Appendix Table A1).
Meta-analysis
The first meta-analysis considered all 6 sports by osteoarthritis site/joint (hip, knee, and ankle; foot was not included, as only 1 study 92 examined this site) (Figure 2). Results indicated that exposure to focused sports was associated with a higher RR of developing osteoarthritis of the hip (RR = 1.67 [95% CI, 1.15-2.41]; P = .007), knee (RR = 1.60 [95% CI, 1.23-2.08]; P < .001), and ankle (RR = 7.08 [95% CI, 1.24-40.51]; P = .03) as compared with the controls.

Relationship between sport and (A) hip osteoarthritis, (B) knee osteoarthritis, and (C) ankle osteoarthritis. M-H, Mantel-Haenszel.
Next, the meta-analyses considered each sport in turn (except bobsleigh, as there was only 1 study 63 on this sport).
Ice Hockey
The ice hockey data were examined by joint. The hip data (RR = 1.70 [95% CI, 1.27-2.29]; P < .001; I 2 = 12%) showed a significantly increased risk of developing hip osteoarthritis than did the comparators (including elite other sports, military, and other comparator groups; limited heterogeneity) (Figure 3A). When this analysis was repeated to limit the comparator group to “military” and “other” only (ie, excluding those from elite other sports), differing results were achieved (RR = 1.76 [95% CI, 0.72-4.33]; P = .22; I 2 = 81%), with no significant difference between the individuals exposed to ice hockey and controls, albeit with considerable heterogeneity (Figure 3B). For knee osteoarthritis, the results showed a higher risk of knee osteoarthritis for the ice hockey group (1.52 [95% CI, 1.18-1.96]; P = .001; I 2 = 0%) (Figure 3C). Sensitivity analysis (without elite other sports comparators) indicated a slightly larger effect size (RR = 1.64 [95% CI, 1.26-2.13]; P = .0002; I 2 = 0%) (Figure 3D). There were no separate ankle or foot meta-analyses for ice hockey.

Forest plots assessing the risk of hip osteoarthritis after participation in ice hockey (elite and nonelite) as compared with a control group: (A) sports in control group and (B) no sports in control group. Forest plots assessing the risk of knee osteoarthritis after participation in ice hockey (elite and nonelite) as compared with a control group: (C) sports in control group and (D) no sports in control group. M-H, Mantel-Haenszel.
Wrestling
The wrestling data were examined by joint. The hip data showed an increased risk for the wrestling group (RR = 1.78 [95% CI, 1.20-2.64]; P = .004; I 2 = 0%) (Figure 4A). Sensitivity analyses (without elite other sports comparators) indicated a larger effect size, albeit not statistically significant and with considerable heterogeneity (RR = 2.43 [95% CI, 0.52-11.34]; P = .26; I 2 = 90%) (Figure 4B). For knee osteoarthritis, the data showed a higher risk for the wrestling group (RR = 2.22 [95% CI, 1.59-3.11]; P < .001; I 2 = 0%) (Figure 4C). Sensitivity analyses demonstrated similar results but with higher (substantial) heterogeneity (RR = 2.51 [95% CI, 1.39-4.53]; P = .002; I 2 = 52%) (Figure 4D). No separate ankle or foot meta-analyses were performed for wrestling.
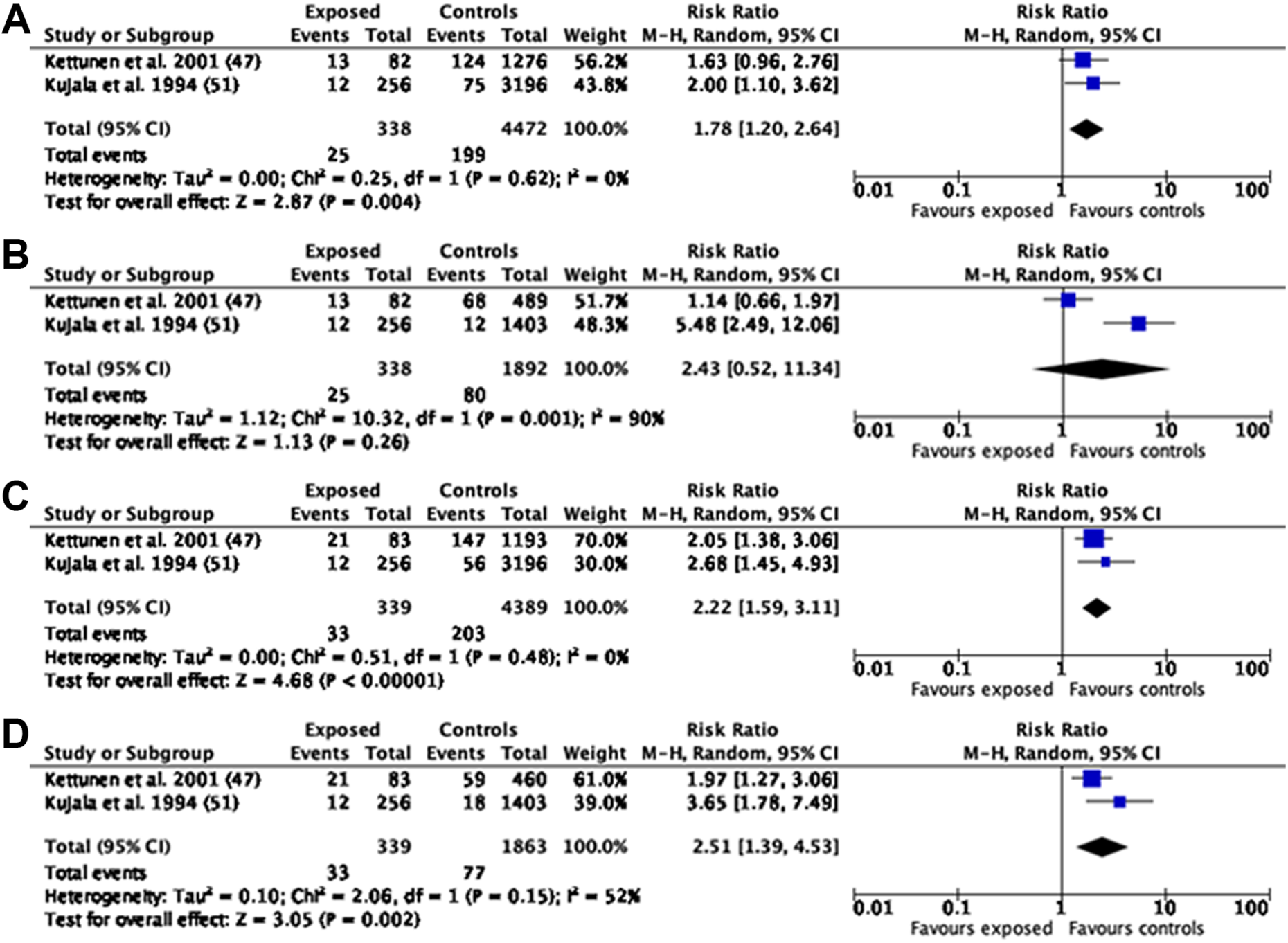
Forest plots assessing the risk of hip osteoarthritis after participation in wrestling (elite and nonelite) as compared with a control group: (A) sports in control group and (B) no sports in control group. Forest plots assessing the risk of knee osteoarthritis after participation in wrestling (elite and nonelite) as compared with a control group: (C) sports in control group and (D) no sports in control group. M-H, Mantel-Haenszel.
Handball
The handball hip osteoarthritis data showed no statistically significant risk for handball players (RR = 2.50 [95% CI, 0.85-7.36]; P = .10; I 2 = 80%) (Figure 5A). Sensitivity analyses indicated the opposite, with handball players at a significantly increased risk (RR = 2.73 [95% CI, 1.14-6.52]; P = .02; I 2 = 69%) (Figure 5B). Both analyses demonstrated high heterogeneity (considerable and substantial). No knee, ankle, or foot meta-analyses were performed for handball.

Forest plots assessing the risk of hip osteoarthritis after participation in handball (elite and nonelite) as compared with a control group: (A) sports in control group and (B) no sports in control group. M-H, Mantel-Haenszel.
Shooting
There was a higher risk for developing knee osteoarthritis in the comparator group than in the group participating in shooting, but this was not statistically significant and had substantial heterogeneity (RR = 0.43 [95% CI, 0.06-2.99]; P = .39; I 2 = 72%) (Figure 6). No sensitivity analyses were undertaken, as all comparators were from elite other sports. No hip, ankle, or foot meta-analyses were performed for shooting.

Forest plot assessing the risk of knee osteoarthritis after participation in shooting (elite and nonelite) as compared with a control group (including sports). M-H, Mantel-Haenszel.
American Football
There were no meta-analyses performed owing to insufficient eligible studies.
Discussion
Risk of Osteoarthritis From the Included Sports
The current systematic review evaluated the evidence of differing sports association with osteoarthritis at different joints of the body. We found that collectively participation in the sports in this review (ice hockey, wrestling, handball, shooting, American football, and bobsleigh) was associated with a higher risk of developing osteoarthritis of the hip, knee, and ankle when compared with controls (Figure 2). The highest risk was for ankle osteoarthritis (with data from ice hockey, wrestling, and American football) (RR = 7.08 [95% CI, 1.24-40.51]), with the hip and knee at similar levels of risk (RR = 1.67 [95% CI, 1.15-2.41]; RR = 1.60 [95% CI, 1.23-2.08], respectively; P < .05).
When data were broken down by sport, wrestling and ice hockey were associated with an increased risk of developing knee osteoarthritis when compared with controls (other sports and no other sports), as well as with a higher risk of hip osteoarthritis versus controls including other sports. However, wrestling and ice hockey were not associated with a significant risk of developing hip osteoarthritis compared with controls with no sports. Handball was associated with hip osteoarthritis when compared with controls with no other sports, but the opposite was true when the controls included other sports, with no significant difference between handball players and controls. Shooting participants did not have a statistically significant risk of knee osteoarthritis (RR = 0.43 [95% CI, 0.06-2.99]; P = .39).
Risk of Hip Osteoarthritis From the Included Sports
The meta-analysis substantiated the individual study findings, which showed participation in handball, ice hockey, and wrestling produces an increased risk of developing hip osteoarthritis (when the controls included sports for wrestling and ice hockey and no sports for handball). 47,51,53,90 One reason could be that handball, ice hockey, and wrestling are all sports that involve high impact and torsion of the lower limbs 90 and, as past research has stated, high-impact sport athletes are at higher risk of developing hip osteoarthritis as compared with participants in low- or nonimpact sports. 11,13,23,43 Specifically, high-impact sports, often with sudden and repeated impacts on the hip joint without suitable proprioception and muscle absorption, may lead to minor hip injuries and can result in muscle fatigue and groin pain, possibly leading to stiffening and osteoarthritis of the hip. 45,90 Another reason for the higher risk of developing hip osteoarthritis could be due to femoroacetabular impingement, which has been associated with early-onset osteoarthritis of the hip. 59 Femoroacetabular impingement is more prevalent in athletes, especially those in high-impact sports 2,4 and sports that require end-range movements of hip flexion, adduction, and internal rotation, such as ice hockey. 59 A previous study 34 has demonstrated that individuals who experience knee or hip injuries are more likely to develop hip osteoarthritis. Similarly, past research has indicated that soft tissue knee injuries are a factor in developing hip osteoarthritis, as the injuries may lead to muscle dysfunction in the thigh, which, according to the muscle dysfunction hypothesis, would then affect the development of hip osteoarthritis. 80 However, data from Tveit et al 90 do not support this hypothesis owing to the study finding no significant influence of a previous soft tissue knee injury on the prevalence of hip osteoarthritis.
The increased risk of developing hip osteoarthritis from handball participation has been attributed to joint loading, as during play it has been measured above the physiologic limits of cartilage. 54 This is due to handball placing heavy mechanical loads on the hip joint because the sport requires rapid stoppages, accelerations, and cutting movements. Performing these actions in rapid succession is a major component of competitiveness but heightens the effects of weightbearing. 53,54 The accumulation of heavy loads may decrease the range of movement of a joint, which is a typical sign of osteoarthritis. 13,47,53,86,93 Consequently, handball seems to cause overload to cartilage in the hip, contributing to its degeneration. 53 Kujala et al 51 likewise stated that the high prevalence of hip osteoarthritis in wrestlers could be due to the heavy weight training associated with this sport, which causes excessive loading of the weightbearing joints. The higher RR for wrestlers to develop hip osteoarthritis could be explained by nonphysiologic rotational or mediolateral loading and injuries among wrestlers. 47
The current study found no significant difference in the risk of sustaining hip osteoarthritis from wrestling and ice hockey participation when the controls included no sports and handball participation when the controls included sports. One reason for this could be the global health benefits, including bone health, that sports and exercise provide. 52 Similarly, exercise can increase joint stability and flexibility as well as reduce pain, thus optimizing functional capacity. 75
Owing to an insufficient number of studies, the present work was unable to run analyses to examine the association of shooting and bobsleigh participation with hip osteoarthritis. However, the results from Kettunen et al 47 and Marti et al 63 suggested that shooting and bobsleigh athletes, respectively, have a reduced risk of developing hip osteoarthritis. Specifically, Kettunen et al reported that 4 of 51 shooters had hip disability, as compared with 133 of 1440 controls, which equates to an RR of 0.85 (95% CI, 0.33-2.21). Marti et al noted that 3 of 9 bobsledders had hip disability, as opposed to 19 of 50 controls, equating to an RR of 0.88 (95% CI, 0.33-2.36). According to previous research, the low risk of shooters developing hip osteoarthritis is due to the low risk of sustaining an injury from the sport. 98 In contrast, bobsleigh is a sport with a high risk of sustaining injuries, but a large proportion affect the head or neck. 27 However, a reason why the current review found bobsleigh athletes have a low risk of developing hip disability may be that only 1 study examined this sport and this study had a rather small sample size of 59 participants, 9 of whom were bobsledders. Consequently, this study may have had low statistical power, thereby negatively affecting the likelihood of a nominally statistically significant finding actually reflecting a true effect. 14
Risk of Knee Osteoarthritis From the Included Sports
This review found that wrestling and ice hockey participation produces an increased risk of developing knee osteoarthritis. These findings are consistent with those of past studies 24,47,78,87 showing that wrestling and ice hockey produce a higher risk of developing knee osteoarthritis. However, given the insufficient studies examining American football and handball, the current work was unable to conduct a meta-analysis involving these sports. However, results from Moretz et al 68 and Tveit et al 90 suggested that both sports would produce an increased risk of developing knee osteoarthritis. Specifically, Moretz et al indicated that 11 of 23 American football players developed knee osteoarthritis, as opposed to 1 of 11 controls (RR = 5.26 [95% CI, 0.77-35.77]). Tveit et al noted that 30 of 141 handball players developed knee osteoarthritis as compared with 262 of 1781 controls (RR = 1.45 [95% CI, 1.03-2.03]). Athletes in these sports may have higher risks, as noted before, because of injuries, as previous research 18,69,75,102 has stated that individuals who sustain knee injuries have an increased risk of developing knee osteoarthritis. Likewise, it has been suggested that individuals who participate in team sports, such as American football, ice hockey, and handball, have a heightened risk of developing knee osteoarthritis in part because of knee injuries sustained during these sports. 13,47,55,76,90 All of these findings are supported by previous research that has reported American football, wrestling, ice hockey, and handball are sports in which participants have a high risk of sustaining an injury. 3,21,22,26,27,73 This is supported by Moretz et al, who found that American football players who had a knee injury were more susceptible to developing knee osteoarthritis than were players without a knee injury whereas American football players who did not experience a knee injury were no more likely to develop knee osteoarthritis than were the controls. American football, ice hockey, and handball are all sports that involve high levels of impact and biomechanical forces on the joints, 11,13,24,78 which are risk factors for developing knee osteoarthritis. 11,24,29,78 Another reason for these findings could be that past studies have shown that higher-level athletes—albeit in professional soccer and not a variety of sports—have a higher proportion of varus knee alignment than does the general population. 33 This is important, as varus knee alignment has been shown to increase the risk of developing osteoarthritis 44,79 ; thus, the numerous studies with elite athletes in the present review could have created a selection bias. Comparatively, American football and wrestling have a higher percentage of individuals with a greater body mass index (overweight and obese) than do other sports, such as soccer, basketball, and baseball, 99 which may increase the risk of developing osteoarthritis through causing excessive loading on the weightbearing joints. 51,52
According to earlier research, the increased likelihood of developing knee osteoarthritis through participating in wrestling may be due to the heavy weight training associated with the sport as well as because of the nonphysiologic rotational or mediolateral loading and injuries among wrestlers. 47
This review showed that, as before, controls were more likely to develop knee osteoarthritis than were shooters, with an RR of 0.43 (95% CI, 0.06-2.99). This result is probably due to the low risk of sustaining an injury from shooting. 98 However, this was not significant (P = .39) and may be attributed to the variability among the studies, which was high (I 2 = 72%).
Risk of Ankle Osteoarthritis From the Included Sports
The current study was unable to conduct meta-analyses regarding the ankle for individual sports because of an insufficient number of eligible studies. However, results from Kujala et al 51 and Vincellete et al 92 suggested that ice hockey and American football, respectively, produce an increased risk of developing ankle osteoarthritis. Notably, Kujala et al reported that 3 of 163 ice hockey players had developed ankle osteoarthritis as compared with 6 of 3289 controls, which produced an RR of 10.09 (95% CI, 2.55-39.98). Vincellete et al noted that 55 of 59 American football players developed ankle osteoarthritis compared with 3 of 50 controls, producing an RR of 15.54 (95% CI, 5.18-46.64). These findings could again be attributed to injury risk, with previous research finding that American football and ice hockey players have high risks of sustaining injuries. 21,22,27 Previous studies 42,48 have stated that the foot and ankle are the most common sites for chronic and acute injuries in physically active individuals and athletes. The reason is that the ankle plays an important role in supporting body mass and adjusting the movement while walking or exercising the lower body. 48
In contrast, results from Kujala et al 51 suggested that controls are at a greater risk of developing ankle osteoarthritis than are wrestlers, finding that 0 of 256 wrestlers had developed ankle osteoarthritis as compared with 9 of 3196 controls for an RR of 0.65 (95% CI, 0.04-11.22). Past research 3,21,48,73 has cited high rates of injury in wrestling. However, the current review found controls were more likely to develop ankle osteoarthritis than were wrestlers. It is possible that this finding may be because of only 1 study examining wrestling’s association with developing ankle osteoarthritis—similar to what the present study demonstrated for bobsleigh and hip osteoarthritis. Thus, it is possible the study had low statistical power. 14
The current review found relatively few studies examining ankle osteoarthritis, probably because it is relatively rare, with just 1% of the general population having it. 50 Consequently, the prevalence of ankle osteoarthritis has not been studied as broadly as has knee osteoarthritis. 50,66
Health Benefits of Sport and Physical Activity
Despite the current study demonstrating that participating in some sports is associated with an increased risk of developing osteoarthritis, sports participation still provides health benefits, such as bone health, cardiovascular function, energy metabolism, insulin action, and psychological status 56,63,65,81,97 ; thus it can be argued that despite the higher risk of developing osteoarthritis, the overall health benefits of an active lifestyle outweigh the potential negative effect of developing osteoarthritis.
Strengths and Limitations
The studies in the review and meta-analysis were of good quality, as identified using the Newcastle-Ottawa scale, yet still had limitations. One limitation was their sample sizes. The study by L’Hermette et al 53 had relatively few handball players, 20 of 59 participants; comparably, the study of Marti et al 63 included a sample size of 59 athletes, 9 of whom participated in bobsleigh. The studies of Kujala et al 52 and Kettunen et al 47 also had a limited number of participants for each group of sports, which compromised the sufficient statistical power of the previously mentioned studies. 14,28,64 Specifically, statistical power is affected by differing variables, 1 of which is the sample size. 14,16
All the data in the review were based on male participants for the sports included, thus neglecting female participants and the association of the differing sports and osteoarthritis with female participants. Given that female participants are more susceptible to osteoarthritis than are male participants, this emphasizes the importance for research into the association for female participants. ∥
The studies in the review used differing methods for diagnosing osteoarthritis, which makes it difficult to compare results. 25 The various methods for diagnosing osteoarthritis may produce differing results, as radiologic signs of osteoarthritis can occur without clinical symptoms. 25 Kettunen et al 47 used self-reported diagnosis in their study, which can be affected by recall bias 50 and may result in the data being imprecise, thus exposing the study to a high level of bias. This is supported by earlier systematic reviews that found radiographic methods provided higher prevalence rates than did self-report methods. 6,50,82,83
No research met our inclusion criteria for some sports—namely, archery, baseball, curling, speed skating, and skeleton. This highlights the need for future research to examine the association of these sports and osteoarthritis. The importance is emphasized by previous research stating that athletes in baseball, bobsleigh, short-track speed skating, and skeleton have a high risk of sustaining injuries, 3,21,22,26,27,72,73 thus placing them at a potentially high risk of developing osteoarthritis, as joint injuries have been identified as a risk factor for osteoarthritis. 8,9,89 It is evident that there is limited research into all the sports in the review. As a result, future research could examine the association of these sports with osteoarthritis at differing joints and add to the limited knowledge regarding the association of participating in sports and osteoarthritis. As mentioned earlier, all the studies involved in the present review included male participants; consequently, future research could examine the association of the differing sports and osteoarthritis with female participants. Many studies 47,51,52,63,90 also had a control group that comprised former elite athletes. It is plausible that they may be at risk of osteoarthritis given their previous sports participation and injury. Thus, the level of exposure to sports among studies may have differed. However, their inclusion did make comparing the sports easier, owing to similarities in sports load. Only 3 studies included matched controls. 53,68,90
The review showed a lack of research in recent years, with just 1 publication in the last decade. Another limitation is that gray literature was not a part of the review. Consequently, the findings may reflect publication bias. This study comprised a small number of articles; as a result, it was not possible to use funnel plots to examine publication bias, as they are misleading and inaccurate with few studies. 88,95 The review presented unadjusted RRs in the meta-analysis, meaning that the RRs were not adjusted for cofounding factors, which is an important limitation to consider when interpreting the results. 95
Despite the limitations, various means were used to ensure the quality of this review. First, 4 electronic databases were searched using a thorough search strategy, and citations in identified reviews plus recent relevant journals were hand searched to limit the number of eligible articles missed. The number of eligible articles missed was reduced by using the search strategy again at a later date. Another strength is that the articles were all independently screened by 2 reviewers at each stage of screening. The articles were also quality assessed.
Conclusion
The current review found that participating in handball, ice hockey, and wrestling was associated with a greater risk of developing hip osteoarthritis. However, there was no significant difference for developing hip osteoarthritis for ice hockey and wrestling participants when compared with controls with no sports. Similarly, there was no significant difference in the risk for developing hip osteoarthritis for handball participants when compared with a control group that included other sports. The review also found that participation in ice hockey and wrestling was associated with an increased risk of developing knee osteoarthritis.
Footnotes
Acknowledgment
The authors acknowledge the assistance of Dr Douglas Grindlay in developing and producing the search strategy.
Notes
Final revision submitted November 18, 2020; accepted December 21, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported financially by the Centre for Sport, Exercise and Osteoarthritis Research Versus Arthritis (formerly the Arthritis Research UK Centre for Sport, Exercise and Osteoarthritis; grant 21595) and was supported by the NIHR Nottingham Biomedical Research Centre. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Risk of Bias: Results for the Included Studies a

| Newcastle-Ottawa Scale (Risk of Bias) b | ||||||||
|---|---|---|---|---|---|---|---|---|
| Selection | Comparability | Outcome | Total | |||||
| Study | Sport | B | C | E | F | G | H | |
| Tveit (2012) 90 | Ice hockey | * | * | ** | **** | |||
| Kujala (1994) 51 | Ice hockey | * | * | * | * | **** | ||
| Kettunen (2001) 47 | Ice hockey | * | * | ** | * | **** | ||
| Thelin (2006) 87 | Ice hockey | * | * | ** | * | ***** | ||
| Kujala (1994) 51 | Wrestling | * | * | * | * | * | ***** | |
| Kettunen (2001) 47 | Wrestling | * | * | ** | * | ***** | ||
| L’Hermette (2006) 53 | Handball | * | ** | * | **** | |||
| Tveit (2012) 90 | Handball | * | * | ** | **** | |||
| Kujala (1995) 52 | Shooting | * | * | * | * | **** | ||
| Kettunen (2001) 47 | Shooting | * | * | ** | * | **** | ||
| Moretz (1984) 68 | American football | * | ** | * | **** | |||
| Vincelette (1972) 92 | American football | * | ** | * | **** | |||
| Marti (1989) 63 | Bobsleigh | * | * | * | * | * | ***** | |
a Agency for Healthcare Research and Quality standard for each study: good (out of poor, fair, or good).
b A and D were not applicable. Items and ratings: (A) Representativeness of the exposed cohort. *Study truly representative of the average population in the community. (B) Selection of the nonexposed cohort. *Drawn from the same community as the exposed cohort. (C) Ascertainment of exposure. *Secure record (eg, surgical records) or structured interview. (D) Demonstration that outcome of interest was not present at start of study. *Yes. (E) Comparability of cohorts on the basis of the design or analysis. *Study controls for sport. *Study controls for any additional factor. (F) Assessment of outcome. *Independent blind assessment or record linkage. (G) Was follow-up long enough for outcomes to occur. *Yes. (H) Adequacy of follow-up of cohorts. *Complete follow-up—all subjects accounted for or subjects lost to follow-up unlikely to introduce bias (ie, small number lost).