
Abstract
Background:
As regards anterior cruciate ligament (ACL) reconstruction (ACLR), graft diameter has been identified as a major predictor of failure in skeletally mature patients; however, this topic has not been well-studied in the higher risk pediatric population. Hamstring tendon autograft configuration can be adjusted to increase graft diameter, but tendon length must be adequate for ACLR. Historical parameters of expected tendon length have been variable, and no study has quantified pediatric ACL morphology with other osseous parameters.
Purpose:
To develop magnetic resonance imaging (MRI)–derived predictors of native ACL graft length in pediatric patients so as to enhance preoperative planning for graft preparation in this skeletally immature patient population.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
MRI scans of 110 patients were included (64 girls, 46 boys; median age, 10 years; range, 1-13 years). Patients with musculoskeletal diseases or prior knee injuries were excluded. The following measurements were taken on MRI: ACL length; sagittal and coronal ACL inclination; intercondylar notch width and inclination; and femoral condyle depth and width. Associations between these measurements and patient sex and age were investigated. Univariate linear regression and multivariable regression models were created for each radiographic ACL measure to compare R 2.
Results:
Female ACL length was most strongly associated with the depth of the lateral femoral condyle as viewed in the sagittal plane (R 2 = 0.65; P < .001). Other statistically significant covariates of interest included distal femoral condylar width, age, and coronal notch width (P < .05). For males, the ACL length was most strongly associated with the distal femoral condyle width as viewed in the coronal plane (R 2 = 0.70; P < .001). Other statistically significant covariates of interest for male ACL lengths were lateral femoral condyle depth, age, and coronal notch width (P < .05).
Conclusion:
In pediatric populations, femoral condylar depth/width and patient age may be valuable in assessing ACL size and determining appropriate graft dimensions and configuration for ACLRs. The use of this information to optimize graft diameter may lower the rates of ACL graft failure in this high-risk group.
Pediatric athletes represent a high-risk population as regards anterior cruciate ligament (ACL) reconstruction (ACLR) failure, with rates of retear significantly higher than that of adults. 4,6,8,13,17 The use of tendon autograft 24 and larger diameter grafts have been identified as significant variables shown to affect the retear rate in adolescent and adult populations undergoing ACLR. Hamstring graft diameter equal to or greater than 8.5 mm, 4,17,18,23,28 and even up to 10 mm, 29 have been associated with lower failure rate. As such, there has been substantial attention in the orthopaedic literature devoted to maximizing tendon diameter with multistrand configurations beyond the 4-strand hamstring autograft. Five-strand, 1,15 6-strand, 7,33 and even up to 8-strand 22 hamstring autograft configurations have been proposed to enable larger diameter grafts. However, with each progressive strand quantity, overall graft length is sacrificed. For example, to obtain a 4-strand ACL graft with a length of 6 cm, a total unfolded graft length of 24 cm is needed. However, to get the same 4-strand ACL graft to be 7 cm, a total unfolded graft length of 28 cm would be required. As such, adequate surgical preparation necessitates a comprehensive understanding of graft position, both within the bone tunnels and intra-articular length. The former may be controlled by a drilling technique or fixation method. The latter, however, is often a standardized value based on the patient’s individual anatomy and may be inadequately assessed on preoperative imaging of the distorted anatomy of an injured knee.
Cadaveric and imaging-based studies of the ACL in children are more limited, and some have looked at unique anatomic landmarks such as ACL position with respect to the physis, but studies looking at the linear dimension of the pediatric ACL are more limited. While considerable attention has been devoted to understanding this value in the adult knee, 3 few studies have assessed normative parameters of intra-articular length in the pediatric knee. Edmonds et al 5 conducted a magnetic resonance imaging (MRI) study of native pediatric knee anatomy and found that the intra-articular length was a mean of 24 to 25 mm in patients aged younger than 7 years but was more than 32 mm for patients older than 7 years of age. Lima et al 16 described a nonlinear growth curve for pediatric ACL length that does not follow the height growth curve. In the adult literature, Miller and Olszewski 21 showed directly measured graft length to be a mean of 23.6 mm, but this has contrasted with other studies that have shown measured distances up to 40 mm. 20,27
A more comprehensive knowledge of pediatric ACL intra-articular length may assist surgeons in adequately addressing the difficulties related to treating this high-risk patient population by carefully selecting graft configuration that support lower rates of graft failure. The purpose of this study was to utilize uninjured pediatric knee MRI data to evaluate ACL length in the context of bone parameters readily available on standard knee preoperative imaging. We hypothesize that dimensions on the knee MRI can estimate the ACL graft length for that patient. This information may be used preoperatively to plan for graft length and optimize graft configuration.
Methods
Patient Selection and MRI Examinations
Ethics approval for this study was provided by our institution. The patient cohort was aggregated using an integrated database (STARR). Patients who had an existing MRI scan of the knee on file from January 2005 to August 2018 were included in our study. Patients were excluded if there was a reported prior injury or surgery to the knee, or deformity to the tibia or femur, or other syndromes. Additionally, we excluded patients with a closed physis. A total of 110 patients, 64 girls and 46 boys aged 1 to 13 years (median age, 10 years) were selected. All MRIs were T1-weighted, 1.5-T with a 2.5-mm section thickness as clinically appropriate, performed within the home institution.
MRI Measurements
The ACL length, sagittal inclination, coronal inclination, and intercondylar roof inclination were measured as described previously by Lima et al. 16 Using the eUnity PACS Viewer (Client Outlook), 2 3 evaluators (E.P.T., A.B.D., B.V.) independently measured each parameter to provide interrater reliability. The evaluators were medical students and orthopaedic residents experienced with pediatric knee cadaveric dissections and MRI measurements of pediatric knees. Oversight and training, including review of the measurements, was supervised by a senior orthopaedic surgeon (K.G.S.).
ACL Length (anterior and midsubstance). Using the best sagittal image of the ligament, the ACL length was determined by 2 separate measurements. The anterior ACL length was measured as the distance from the most posterosuperior point of the femoral origin to the most anterior point of the tibial insertion of the ligament (Figure 1A). The midsubstance ACL length was measured from the most posterosuperior point of the femoral origin to the midsubstance of the tibial insertion (Figure 1B).
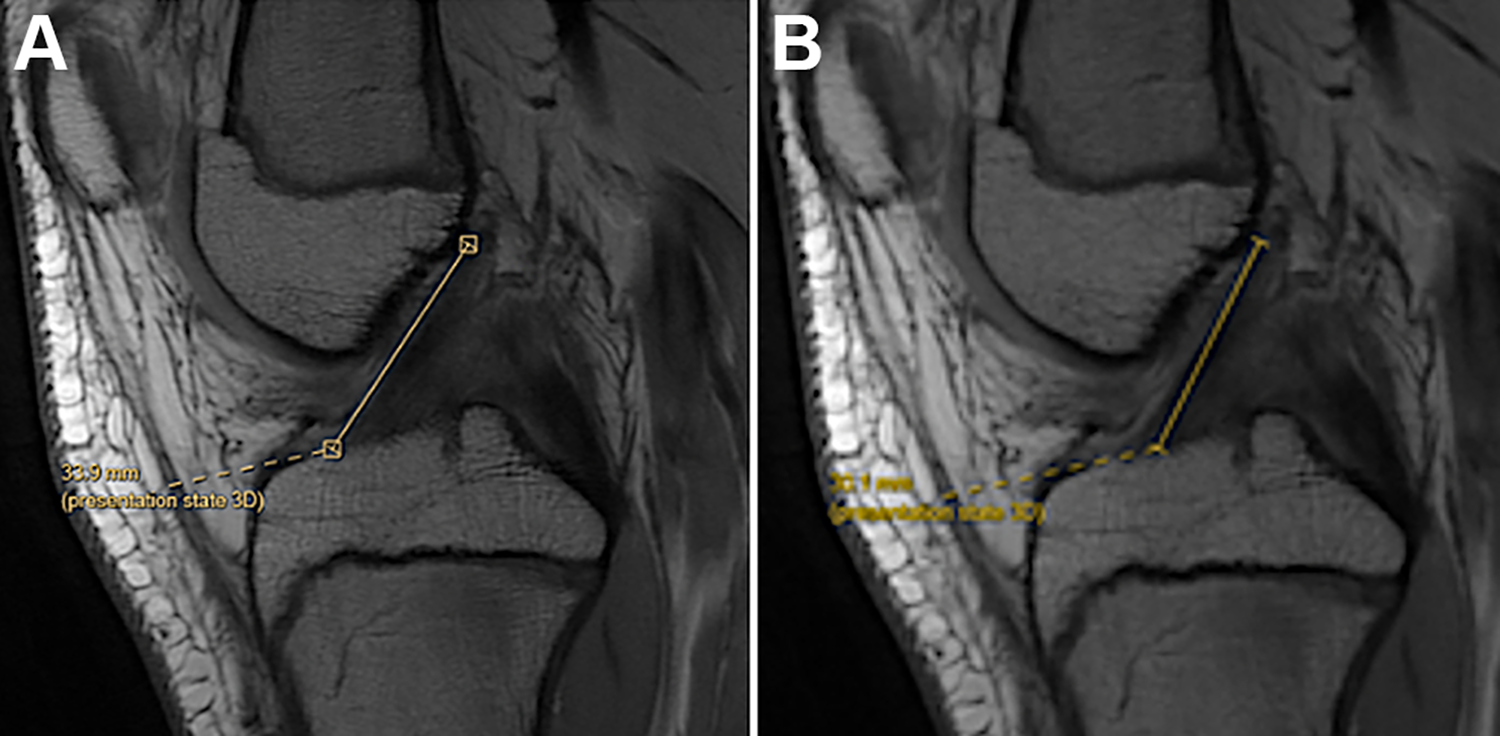
(A) The anterior ACL length was measured as the distance from the most posterosuperior point of the femoral origin to the most anterior point of the tibial insertion of the ligament. (B) The midsubstance ACL length was measured from the most posterosuperior point of the femoral origin to the midsubstance of the tibial insertion. ACL, anterior cruciate ligament.
Intercondylar Roof Inclination. Using a midline sagittal image, the angle of the intercondylar roof incline was measured between the Blumensaat line and the central line parallel to the diaphysis (Figure 2).

Using a midline sagittal image, the angle of the intercondylar roof incline was measured between the Blumensaat line (lower line in image) and the central line parallel to the diaphysis. In this patient, the inclination was 35.9°.
Lateral Femoral Condyle Depth. The depth of the lateral femoral condyle was recorded on the sagittal image with the widest portion of the lateral femoral condyle. The measurement was conducted from the most anterior margin on the condyle to the most posterior ossified margin along a line drawn perpendicularly to the posterior cortical reference line parallel to the diaphysis (Figure 3).

The depth of the lateral femoral condyle was recorded on the sagittal image with the widest portion of the lateral femoral condyle. The measurement was made from the most anterior margin on the condyle to the most posterior ossified margin along a line drawn perpendicularly to the posterior cortical reference line parallel to the diaphysis. In this patient, the depth was 59.78 mm.
Distal Femoral Epiphysis Width. On the coronal view with the widest portion of the distal femur, the width of the distal femoral epiphysis was measured along a line that was parallel to a reference line connecting the most distal aspect of both the medial and lateral condyles (Figure 4).

On the coronal view with the widest portion of the distal femur, the width of the distal femoral epiphysis was measured along a line that was parallel to a reference line connecting the most distal aspect of both the medial and lateral condyles. In this patient, the width was 68.00 mm.
Coronal Notch Width. The coronal notch width was defined as the maximum width of the intercondylar notch, viewed coronally, along a line parallel to a reference line connecting the most distal aspect of both the medial and lateral femoral condyles (Figure 5).

The coronal notch width was defined as the maximum width of the intercondylar notch, viewed coronally, along a line that was parallel to a reference line connecting the most distal aspect of both the medial and lateral femoral condyles. In this patient, the width was 20.79 mm.
Statistical Analysis
Descriptive statistics are presented as counts and percentages for categorical variables and as means and standard deviations for continuous variables. Differences in radiographic measures and ages between male and female patients were analyzed using independent 2-sample t tests; differences in ethnicity between male and female patients were analyzed with the chi-square test.
For each bone morphology measure, a univariate linear regression model was created individually using age- or patient-size variables, testing both linear and quadratic terms. Femoral width, femoral depth, and coronal notch width were used as proxies for patient size. Models were compared using adjusted R 2 values, which adjusts for the number of variables in the model and is the best for model comparison. Multivariable regression models were then created for each radiographic ACL measure, using backward stepwise regression to find the best-fitting models using R 2 values. The intraclass correlation coefficients (ICCs) were reported for each radiographic measure among the 3 evaluators. All statistical analyses were completed using RStudio Version 1.1.456 (RStudio) 11 using a 2-sided level of significance of .05.
Results
Neither the age nor ethnicity of our study population were significantly different between male and female patients.
On average, girls had a narrower coronal notch than boys as a group by 1.3 mm (P < .001) (Table 1 and Figure 6). No significant differences between sexes were observed for ACL length (both anterior and midsubstance) (P = .684 and P = .365, respectively), intercondylar roof inclination (P = .794), depth of lateral femoral condyle (P = .082), and width of distal femoral epiphysis (P = .431).
Differences in ACL Measurements Between Sexes a

a Data are reported as mean ± SD. ACL, anterior cruciate ligament.
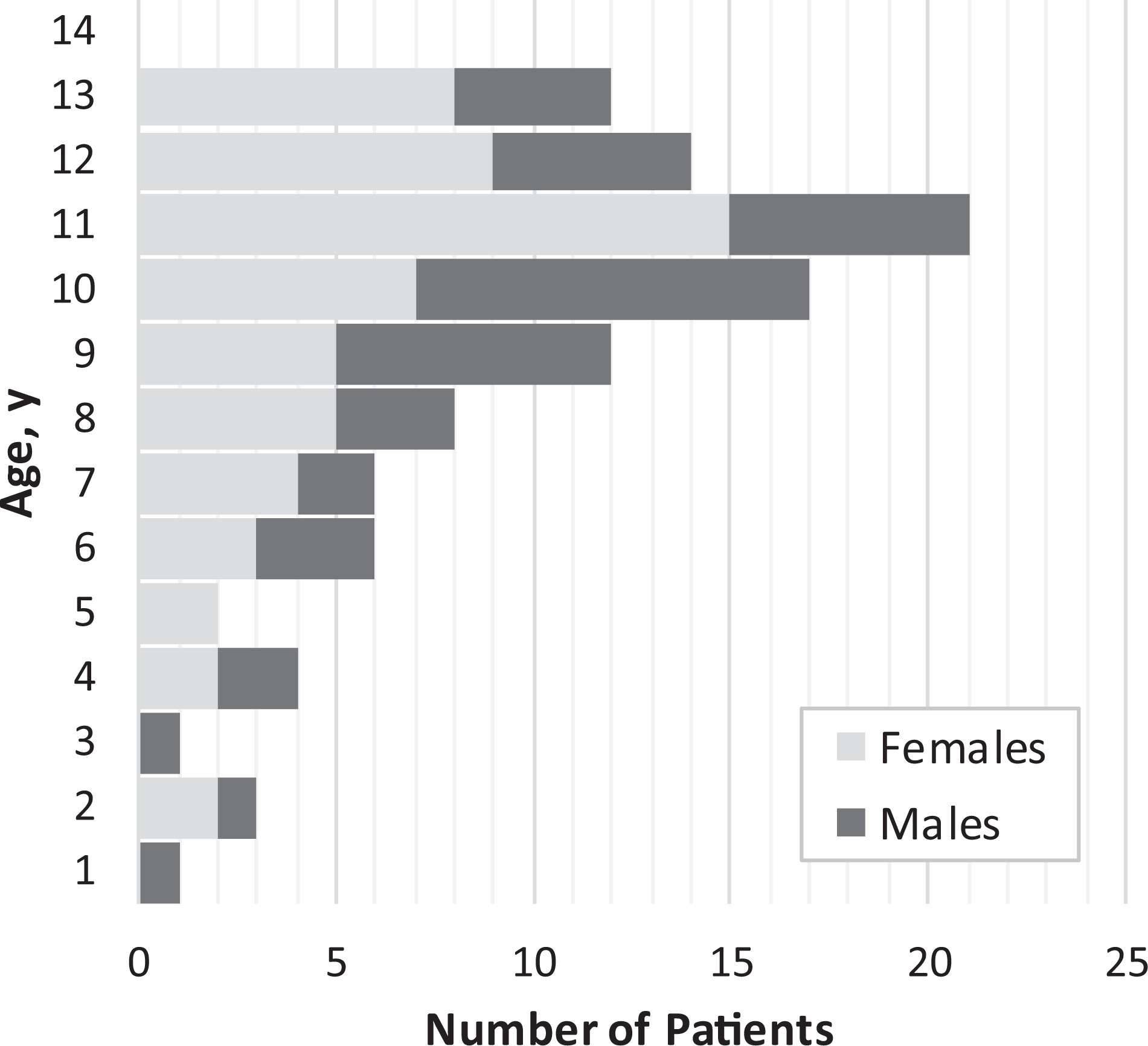
Age distribution of the patients by sex.
When examining the covariates for anterior ACL length for each sex, female ACL length was most strongly associated with the depth of the lateral femoral condyle under linear regression (adjusted R 2 = 0.65; P < .001) (Table 2 and Figure 7). For boys, ACL length was most strongly associated with the distal femoral condyle width taken in the coronal view (adjusted R 2 = 0.70; P < .001) (Figure 8). The strongest association for midsubstance ACL length for both sexes was in the same order as the covariates for anterior ACL length (Table 3). The overall ICC value was 0.81, with most ICC values for individual measurements being above 0.75 (Table 4).
Predictors for Anterior ACL Length a
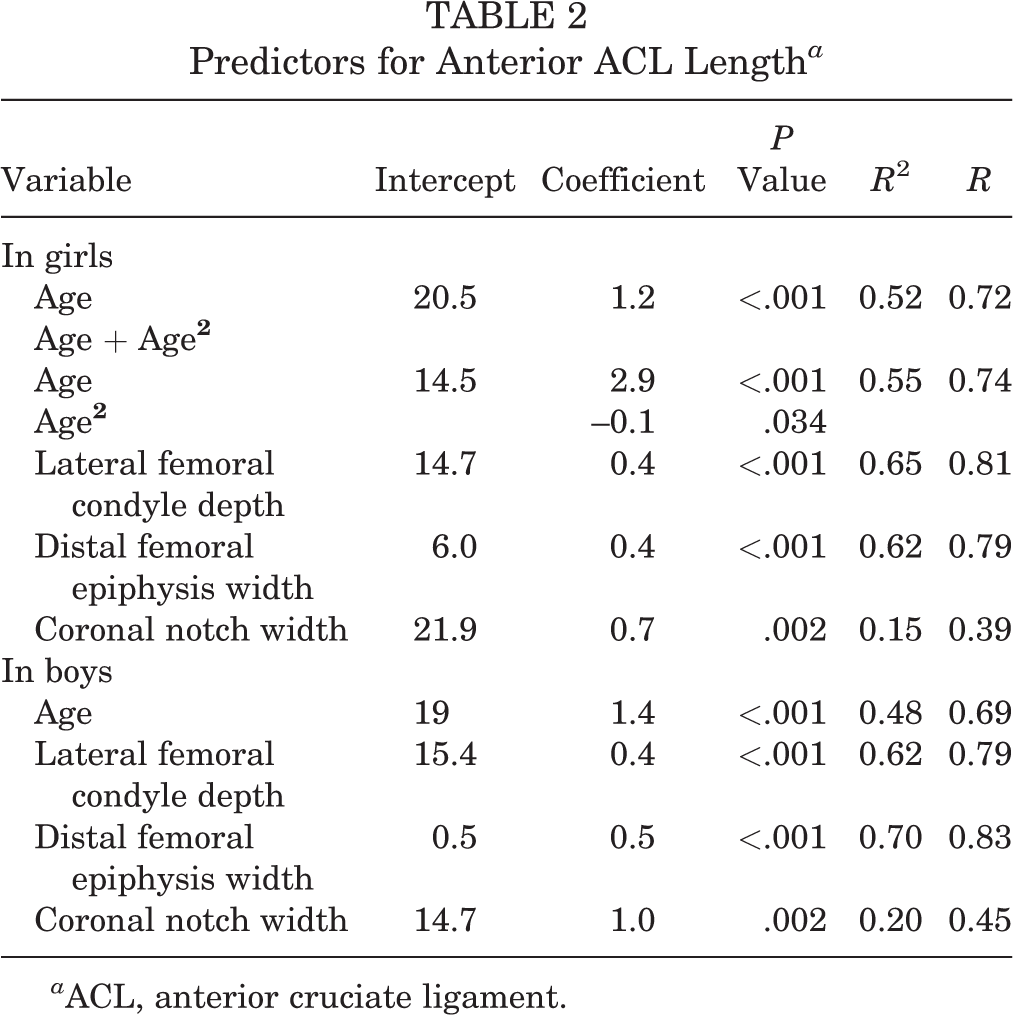
a ACL, anterior cruciate ligament.

The line/curve of best fit (blue line) for girls of anterior (ANT) ACL length by predictor: (A) age; (B) distal femoral epiphysis width; (C) lateral femoral condyle depth; and (D) coronal notch width. Gray shading indicates the 95% CI for the model. ACL, anterior cruciate ligament.

The line/curve of best fit (blue line) for boys of anterior (ANT) ACL length by predictor: (A) age; (B) distal femoral epiphysis width; (C) lateral femoral condyle depth; and (D) coronal notch width. Gray shading indicates the 95% CI for the model. ACL, anterior cruciate ligament.
Predictors for Midsubstance ACL Length a
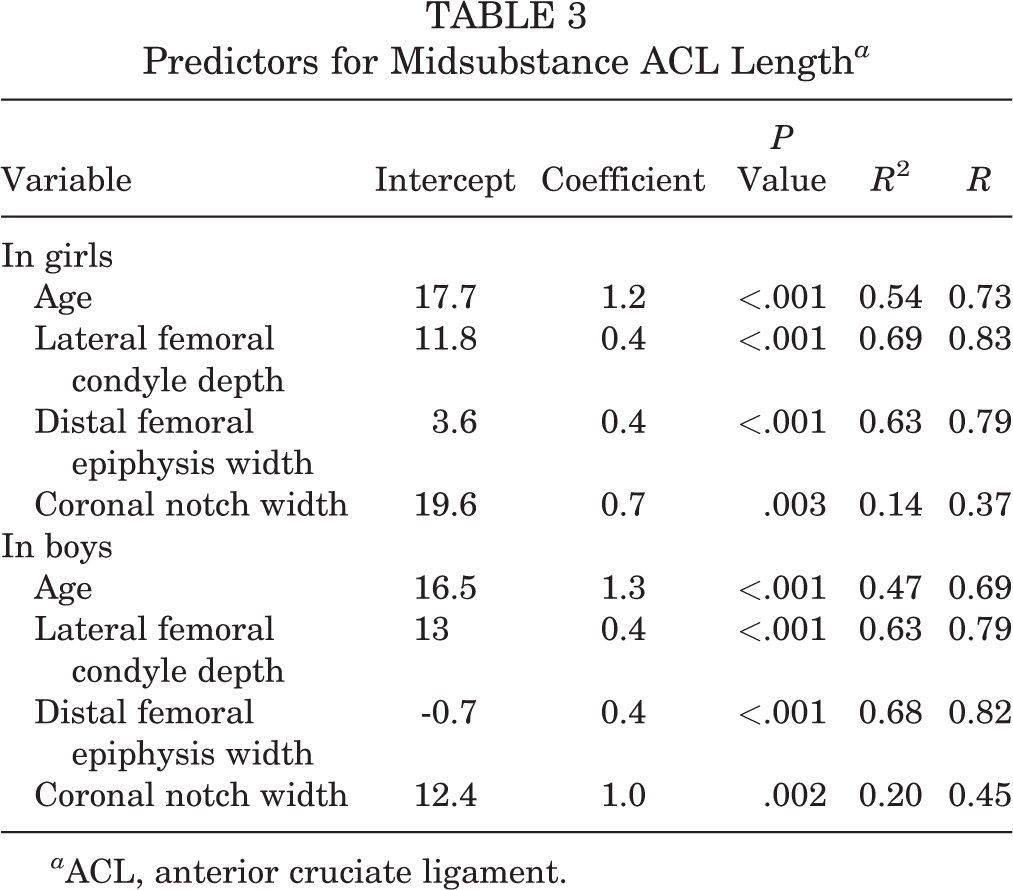
a ACL, anterior cruciate ligament.
ICC Values for ACL Measurements Between the 3 Evaluators a

a Analysis is based on the measurements of 14 patients randomly selected to compare between evaluators. ACL, anterior cruciate ligament; ICC, intraclass correlation coefficient.
Regression analysis was used to construct equations that best estimated ACL length:
Female anterior ACL length (mm) = 0.4 × (Lateral femoral condyle depth) + 14.7
Male anterior ACL length (mm) = 0.5 × (Distal femoral epiphysis width) + 0.5
Female midsubstance ACL length (mm) = 0.4 × (Lateral femoral condyle depth) + 11.8
Male midsubstance ACL length (mm) = 0.4 × (Distal femoral epiphysis width) – 0.7
Discussion
The most significant finding of the current study was that MRIs of osseous parameters effectively estimated ACL intra-articular distance and that correlations were sex-dependent. The width of the distal femoral epiphysis was most strongly associated in boys, and the lateral femoral condyle depth was most strongly associated in girls, for ACL dimension.
In this study, the female ACL length increased with age and began to plateau at around 12 years of age. As our study was limited to preteen patients, we were not able to draw conclusions on growth deceleration in male patients, nor were we able to determine peaks of growth. However, these findings are consistent with prior literature, as Lima et al 16 showed stabilization in growth acceleration between ages 11 and 14 years in girls and 12 to 15 years in boys. Similar to Lima et al, our growth deceleration preempted the expected peak height velocity of height growth, as documented by McCormack et al 19 and Kelly et al, 14 wherein growth velocity peak corresponds to the age of 11.6 years for girls and 13.4 years in boys. 14,19 Similarly, Tuca et al 32 demonstrated that ACL growth plateaued before most rapid height growth. In their series, which reviewed MRI scans of pediatric patients aged 3 to 13 years, both ACL volume and intercondylar notch size plateaued at age 10, notably without significant differences between boys and girls.
As smaller graft size has been associated with higher rates of ACL failure, surgical techniques and planning that allow for optimal graft length and diameter should be considered. At the other end of the spectrum, a graft that is too large may present alternative risk. To date, no studies have demonstrated a clear clinical benefit of a graft beyond 10 mm in diameter. In fact, enlarged graft size has been identified as a risk factor for arthrofibrosis, a condition of particular risk in pediatric ACLR. 17 Su et al 30 conducted a retrospective case-control study of 20 patients with arthrofibrosis after ACLR and found that an increase of 1 mm in graft diameter was associated with a 3.2-times increased odds of this complication. Large grafts are concerning for both overt mechanical impingement that results from overstuffing a knee with a smaller intercondylar notch, as has been documented in pediatric studies, 31 as well as from an overactive biologic inflammatory response. However, the true mechanism in which arthrofibrosis develops has not been fully explained, and the literature provides conflicting results in identifying consistent risk factors. Moreover, arthrofibrosis can typically be expected to resolve with treatment. Regardless, a diagnosis of arthrofibrosis may delay postoperative rehabilitation and may require additional operative procedures. In the end, a surgeon must balance surgical decision-making between expected risk of retear with a small graft versus the risk of possible impingement with a larger graft.
The graft length dimension in terms of the ideal or optimal graft length for the femoral and tibial tunnels is not made clear in the literature. This is due to significant variation in graft choice (quadriceps, tendon, patellar bone/patellar tendon/tibial bone, hamstring, allografts, etc) and variation in fixation techniques with interference screws, suspensory devices, anchors, variation in postoperative rehabilitation, and so on. 9,26 It is the senior author’s (K.G.S.) perspective that interference screw fixation requires longer grafts to obtain adequate fixation strength, but other fixation constructs such as suspensory devices or suture anchors require shorter grafts at the healing interface in these tunnels. Minimal tunnel graft length recommendations are not clear in the literature, with studies suggesting varying lengths 25, 34 to obtain adequate fixation. In most cases, it is prudent to aim for at least 15 mm of graft to reside within the femoral and tibial tunnels and rely predominantly on suspensory and/or anchor fixation devices in cases in which the tunnel/graft interface is shorter. 10,12 The minimal length of graft placement in the tunnel is not clear in the literature, with some animal studies suggesting 15 mm is the length to be considered for some graft types. 25
Study limitations should be noted. Due to the technique of measuring the ACL on the sagittal plane MRI, the measurements may be interpreted as maximum-length measurements and could overestimate the length to the midpoint of the ACL attachment on the femur. During reconstruction, the femoral tunnel is often placed centrally in the femoral footprint, slightly lower than the location of the measurement data, which would result in a shorter overall graft length when performing ACLRs. The current measurements could overestimate the intra-articular graft length necessary for reconstruction and may be considered maximum possible distances.
Additional limitations are noted with the inherent technology limitations of MRI. A slice thickness of 2.5 mm may alter the findings for smaller structures and anatomy variation, particularly in complex 3-dimensional ligamentous anatomy that does not follow precise coronal or sagittal planes. Future studies may consider utilizing ligament-specific sequence imaging to enhance data interpretation or newer MRI protocols that employ the generation of a narrower slice thickness.
Conclusion
The present study analyzed native pediatric ACL parameters and provided a framework in which to estimate intra-articular ACL graft length for ligament reconstructive procedures. Amid the combined challenges of autograft length and size, these data provide information to optimize surgical planning and graft size/configuration for skeletally immature athletes, who have high rates of both ACL injury and reinjury. Due to alterations in ACL anatomy with tearing, bone dimension that correlates with the ACL length may be more valuable than measuring the distance between the ACL footprints in a torn ACL. This information may help surgeons plan for graft configurations that allow for larger overall graft diameter and lower rates of reinjury.
Footnotes
Final revision submitted October 23, 2020; accepted December 14, 2020.
One or more of the authors has declared the following potential conflicts of interest or source of funding: The cadaveric specimens were donated by Allosource. T.J.G. has received educational support from Arthrex and Liberty Surgical. P.D.F. has received educational support from Smith & Nephew and hospitality payments from Medical Device Business Services. D.W.G has received educational support, consulting fees, nonconsulting fees, and royalties from Arthrex and faculty speaker fees from Synthes. T.J.S. has received educational support from Midsouth Orthopedics. K.G.S. has received educational support from Evolution Surgical and hospitality payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Stanford University (protocol No. 49137).
Acknowledgment
The authors thank the Stanford University Department of Orthopedics for its continuous support.