
Abstract
Background:
Superior capsular reconstruction (SCR) is an alternative to reverse shoulder arthroplasty for irreparable rotator cuff tears (IRCTs). The reconstructed capsule acts as a static restraint to prevent superior migration of the humeral head. Traditional SCR uses a fascia lata autograft, which has shown failure at the greater tuberosity. An Achilles tendon–bone allograft has been proposed to improve the failure rate.
Purpose:
To evaluate the surgical outcomes of SCR using an Achilles tendon–bone allograft for the treatment of IRCTs.
Study Design:
Case series; Level of evidence, 4.
Methods:
We retrospectively evaluated 6 patients with massive IRCTs who underwent SCR using an Achilles tendon–bone allograft between January 2017 and January 2018. Clinical outcomes were assessed using range of motion, the American Shoulder and Elbow Surgeons score, and the visual analog scale for pain. The acromiohumeral distance and the status of graft integrity were evaluated using serial magnetic resonance imaging. Second-look arthroscopy surgery was performed to evaluate graft integrity at the mean of 7.5 months postoperative.
Results:
The mean ± SD clinical follow-up period was 14.5 months (range, 12-17 months). The American Shoulder and Elbow Surgeons and visual analog scale scores improved from 42.8 ± 11.9 and 4.0 ± 1.2 to 62.1 ± 14.7 and 2.8 ± 1.4, respectively. Forward flexion and external rotation improved from 98° ± 36° and 58° ± 4° to 123° ± 20° and 39° ± 8°, respectively. The acromiohumeral distance improved from 3.9 ± 0.8 mm to 6.4 ± 2.2 mm at final follow-up. However, second-look arthroscopy at a mean of 7.6 months postoperatively confirmed a graft failure rate of 83.3%.
Conclusion:
SCR using an Achilles tendon–bone allograft for the treatment of IRCTs had a high graft failure rate among patients in this case series.
Keywords
Rotator cuff tears represent one of the most common causes of shoulder-related disability. 23 It has been reported that the prevalence of rotator cuff tears is approximately 20% of the general population, 59 which increases to 54% of individuals aged > 60 years. 51 In the Republic of Korea, the age-adjusted rate of rotator cuff repair surgery per 100,000 individuals was 13.15 cases in 2007 and 116.04 cases in 2015. 23 Of irreparable rotator cuff tears (IRCTs), which are mostly associated with massive tear size, 79% are estimated to have recurrent tears after surgical repair. 18 Several nonarthroplasty options have been described for the treatment of IRCTs, including debridement, long-head biceps tenotomy, 57 tuberoplasty, 44 partial repair, 9 tendon transfer, 12 and patch grafts. 1 Reverse shoulder arthroplasty is an alternative option for the treatment of massive IRCTs; however, its longevity is limited in young patients. 49 Mihata et al 39 described reconstruction of the superior capsule of the shoulder using an autograft fascia lata, which provides the passive restraint against the upward migration of the humeral head. Since then, superior capsular reconstruction (SCR) using fascia lata autografts 6,30,32,37,48,60 and human dermal allografts 7,20,45,46 has been used for the treatment of IRCTs.
Graft integrity after SCR is an important independent factor to improve postoperative functional outcomes. 7,35,39 At present, graft failure rates have been variably reported from 0% to 55% and appear to be comparable among various graft types. ∥ The majority of these failures have been observed at the fixation point of the graft on the greater tuberosity. 32 Consequently, an Achilles tendon–bone allograft has been used in SCR to provide stronger fixation at the greater tuberosity site. 27
Results from animal studies have shown that homogeneous tissue healing (bone to bone) is superior to heterogeneous tissue healing (bone to tendon) in terms of healing time and tissue integration with the respect of tensile properties at the healing complex. 31,56 The advantage of an Achilles tendon–bone allograft is an intact native bone–tendon interface that allows homogeneous tissue healing. However, surgical outcomes after SCR using an Achilles tendon–bone allograft have not yet been defined.
The current study evaluated the surgical outcomes of our initial experience performing an SCR using an Achilles tendon–bone allograft for the treatment of IRCTs.
Methods
Patient Selection
This was a retrospective case series of patients who underwent SCR at a tertiary referral hospital between January 2017 and January 2018; institutional review board approval was acquired for this study. The inclusion criteria were as follows: (1) diagnosis of IRCT Patte stage 3 medial retraction on preoperative magnetic resonance imaging (MRI) according to patients' medical records between January 2017 and January 2018, (2) minimum evidence of significant bony deformity caused by glenohumeral arthritis on standard shoulder anteroposterior radiograph, 17 (3) irreducible rotator cuff tear after arthroscopic reduction trial, (4) intact deltoid muscle at the time of physical examination, (5) SCR performed by a single surgeon (I.-H.J.), and (6) SCR using an Achilles tendon–bone allograft. Exclusion criteria were as follows: (1) severe bone deformity (Hamada grade 5), (2) severe superior migration of the humeral head that could not be corrected using arm traction, (3) irreparable subscapularis tendon, (4) cervical nerve and axillary nerve palsy, (5) revision SCR, and (6) <2 years of minimum follow-up. A total of 6 patients were included in the current case series.
Surgical Technique
Patients were prepared and draped in the beach-chair position under general anesthesia after an interscalene brachial plexus block. 26 Diagnostic arthroscopy through a lateral portal was performed to confirm the size and configuration of a rotator cuff tear. After the rotator cuff tear was determined to be irreparable without tension, the surgical setting was changed from arthroscopy to an open setting with the following steps.
A 5-cm skin incision was longitudinally made starting from the midpoint of the one-third lateral margin of the acromion to the lateral border of the coracoid process. The deltoid was split longitudinally 3 to 4 cm between the anterior and middle deltoid. A curvilinear incision was made to take down a small portion of the anterior deltoid and the coracoacromial ligament. A routine acromioplasty was performed for all patients. The mediolateral distance from the glenoid to the footprint of the greater tuberosity was measured using a probe for graft sizing. The Achilles tendon–bone graft, which had undergone gamma irradiation (25 kGy), was prepared on a table in the operating room. The Achilles tendon–bone graft was thawed in warm saline for 30 minutes before preparation. The calcaneus bone was trimmed using an oscillating saw to fit the greater tuberosity. The width and length of the Achilles tendon was prepared according to the defect size measured. The Achilles tendon was folded twice to achieve a minimum thickness of 6 mm. A running stitch No. 2-0 polyester suture (Ethibond; Johnson & Johnson) was applied at the graft margin. The bursal side of the graft was marked with a surgical marker pen to ease orientation (Figure 1).

Graft preparation using (A) the Achilles tendon–bone allograft thawed using warm normal saline. The graft was fashioned according to the defect size measured. (B-D) A graft at least 6 mm thick was obtained during the final preparation.
The long head of the biceps tendon was tenotomized, if present. The superior margin of the glenoid was debrided, allowing for 2 all-suture anchors for fixation (Suturefix Ultra Anchor, 1.9 mm; Smith & Nephew). Sutures from the glenoid anchors were passed through the medial end of the graft using horizontal mattress configuration before graft delivery. The graft was introduced into the joint using the Kelly clamp and secured to the glenoid (Figure 2).

The greater tuberosity bone bed was prepared after (A) insertion of the glenoid anchors (left shoulder, beach-chair position). (B) The graft was shuttled to the joint, and (C) the bony portion of the graft was fixed using a cortical screw.
The greater tuberosity was cleared from degenerated fibrocartilage using a bone curette and rongeur. The greater tuberosity was prepared using the combination of a burr and bone rasp to allow maximum bone-to-bone contact with the bone part of the graft. The bone portion of the graft was fixed to the greater tuberosity using a 3.5-mm self-tapping cortical screw and washer (Depuy Synthes). The graft was repaired side to side using polyester sutures (No. 1 Ethibond; Johnson & Johnson) to the remaining anterior and posterior rotator cuff tissue. When possible, the remaining bursa tissue was repaired to the reconstructed capsule as adapted from previous studies. 4 The deltoid was repaired to the acromion using heavy absorbable suture (No. 1 Vicryl; Ethicon).
After the surgery, all patients used a shoulder abduction brace (in 30° to 45° abduction) for 6 weeks and began pendulum exercises at 3 weeks. After gaining range of motion (ROM) after surgery, patients were taught strengthening exercises for the periscapular muscles and rotator cuff by a dedicated physical therapist at 3 months postoperatively.
Clinical Outcomes Assessment
Pain was measured using a visual analog scale (VAS). Functional outcome was evaluated using the American Shoulder and Elbow Surgeons (ASES) score with minimal clinically important difference as a reference value. 25 For active shoulder ROM, forward flexion (FF) and external rotation (ER) were measured using a handheld goniometer. The internal rotation was measured as the spinous process level that could be reached by the thumb of the patient in a sitting position. Medical records were reviewed for any surgical complications such as reoperation, wound complications, deep infections, and nerve injury. A fellowship-trained orthopaedic surgeon acting as the independent examiner (Y.S.) who was not involved in the surgery performed all clinical assessments at 3, 6, and 12 months postoperatively.
Radiological Outcomes Assessment
The preoperative MRI scans were reviewed to evaluate the involved tendons, tear size, and fatty infiltration according to the Goutallier index. 10,14 The graft integrity was evaluated after the index surgery using a 3.0-T MRI (Achieva; Philips Medical System) at postoperative months 3, 6, and 12 and then annually thereafter (Figure 3). 32

Magnetic resonance imaging scan of the right shoulder for the evaluation of graft integrity at 6 months after index surgery (yellow arrows indicate intact graft).
Graft failure was defined as any sign of graft discontinuity observed in every coronal section. 3 The timing of graft tear was categorized as early (within 3 months postoperatively), midterm (at 3-6 months postoperatively), and late (after 6 months postoperatively). 24 The acromiohumeral distance (AHD) was measured using plain standard shoulder radiographs, which were taken with the radiographic beam tilted 20° caudally in anteroposterior projection. 58 The stage of rotator cuff arthropathy was evaluated using the Hamada classification system. 17 Fatty infiltration of the rotator cuff muscles was rated using the global fatty degeneration index (GFDI). 15 A fellowship-trained shoulder specialist (E.K.) who was blinded to patient-identifying information and clinical outcomes analyzed all imaging studies.
Second-Look Arthroscopy and Histology Assessment
Arthroscopically assisted implant removal was performed when evidence of greater tuberosity union existed and was confirmed using MRI assessment. The implant removal procedure typically occurred in the 6-month postoperative period. A second-look evaluation of graft integrity was performed during the implant removal procedure (Figures 4 and 5). We considered any sign of graft discontinuity as graft failure and recorded the position of this failure. A biopsy was performed when graft failure was confirmed. Tissue retrieved during biopsies was evaluated using hematoxylin and eosin staining.

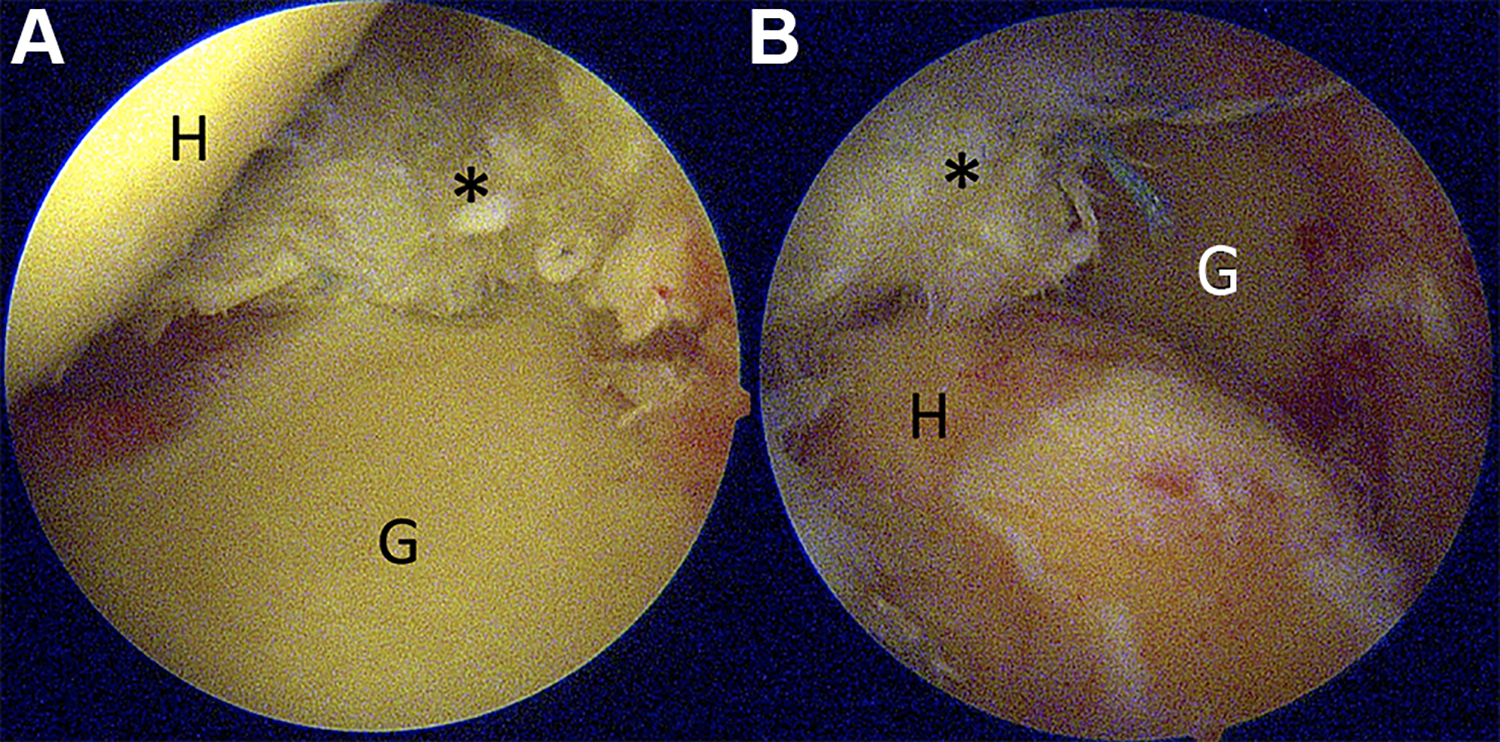
Second-look arthroscopy (right shoulder, patient 4) at the glenohumeral joint during implant removal procedure revealed an intact graft (asterisks) at 7 months after superior capsular reconstruction. (A and B) Glenohumeral joint, posterior viewing portal. G, glenoid; H, humerus.
Second-look arthroscopy (left shoulder, patient 5) during implant removal showing failure of the graft (asterisks) at the anterior aspect at 7 months after superior capsular reconstruction. (A) Glenohumeral joint, posterior viewing portal, and (B) subacromial joint, lateral viewing portal. G, glenoid; H, humerus.
As this was a case series with a limited number of patients, we did not perform statistical comparisons.
Results
Clinical Outcomes
A total of 6 patients (4 men, 2 women) were reported at a mean follow-up of 14.5 months (range, 12-17 months). The dominant extremity was affected in 50% of the patients. Five patients were manual workers. The patients’ mean age at the time of surgery was 62.3 years (range, 60-65 years) (Table 1).
Preoperative Patient Characteristics

The mean preoperative ASES and VAS scores were 42.8 ± 11.9 and 4.0 ± 1.2, respectively. The mean postoperative ASES and VAS scores at the final follow-up were 62.1 ± 14.7 and 2.8 ± 1.4, respectively. The mean preoperative ROM of FF and ER were 98° ± 36° and 58° ± 4°, respectively. The mean postoperative ROM of FF and ER at the final follow-up were 123° ± 20° and 39° ± 8°, respectively (Table 2). As this was a case series with a limited number of patients, we did not perform statistical comparisons.
Comparison of Pre- and Postoperative Clinical Outcomes a

a ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FF, forward flexion; IR, internal rotation; L, lumbar; Postop, postoperative; Preop, preoperative; T, thoracic; VAS, visual analog score.
Radiological Outcomes
The AHD improved from 3.9 ± 0.8 mm to 6.4 ± 2.2 mm at the final follow-up. GFDI and stage of rotator cuff arthropathy (Hamada stage) did not change from pre- to postoperatively. Graft failure was confirmed in 1 patient (patient 2) on MRI examination at 3 months postoperatively.
Second-Look Arthroscopy and Histology Assessment
Graft failure at the anterior site was confirmed using second-look arthroscopy for 3 patients and at the posterior site for 2 patients (Table 3). The histology examination of the failed graft tissue revealed an arrangement of dense collagen fibers with poor cellularity and blood vessels. We found no significant evidence of inflammation or viable blood vessel formation. There was no living fibroblast observed (Figure 6).
Comparison of Pre- and Postoperative Radiological Outcomes a

a Dash indicates no failure. AHD, acromiohumeral distance; GFDI, global fatty degeneration index; MRI, magnetic resonance imaging; Postop, postoperative; Preop, preoperative.

Microscopic evaluation of failed graft with hematoxylin and eosin staining: (A) 20× magnification and (B) 40× magnification insert showing poor cellularity and no viable blood vessels.
Discussion
This case series describes the limitations of the Achilles tendon–bone allograft used in SCR for the treatment of IRCTs. The literature has shown that graft integrity can positively affect functional outcomes. 7,35 –39 To decrease the graft failure rate, a thick graft can enhance stiffness. 36 However, despite the robust Achilles tendon–bone allograft used, the current study shows a high graft failure rate, which perhaps corresponds to unsatisfactory clinical outcomes. Only 50% of our patients had improvements in their ASES scores that reached the minimal clinically important difference of 21.0 points. 25 The greatest improvement was seen in the patient with an intact graft on second look.
The use of an Achilles tendon--bone allograft for SCR has been previously reported. 27,34 However, these previous reports were technique articles that did not provide clinical or radiographic outcomes. The current study assessed graft integrity serially using MRI scans. Postoperative MRI evaluation at the 3-month follow-up revealed 1 failed graft (16.7%), which was considered a relatively favorable outcome. However, second-look arthroscopy at an average of 7.6 months revealed a greater graft failure rate (5 of 6 grafts; 83.3%), perhaps implying that MRI evaluation overestimates graft integrity.
Basic science studies have emphasized the importance of bone-tendon interface regeneration at the greater tuberosity to reduce failure of rotator cuff repair. 29,33,54,55 These studies have shown that homogeneous tissue healing is superior to heterogeneous tissue healing by comparing bone-to-bone healing and tendon-to-tendon healing with tendon-to-bone healing using different animal models. 31,56 The Achilles tendon--bone allograft with a native bone-tendon interface, which allows homogeneous tissue healing at the greater tuberosity, was used in the current study. The graft failure occurs at the tendinous portion (midsubstance of the Achilles tendon–bone allograft) at which a side-to-side repair with the remaining rotator cuff was performed. Furthermore, the graft failures were not observed at the medial (glenoid) or lateral (greater tuberosity) fixation sites. Perhaps medial and lateral healing of the graft was associated with the improvement in ROM and outcome scores in some of our patients, as the shoulder joints were able to force couple and remain functional. It is universally accepted that structural integrity does not always reflect the clinical outcome after rotator cuff repair surgery. Smaller retear compared with the initial tear was reported to be well tolerated by most of the patients after rotator cuff repair surgery. 11 We postulated that a midsubstance tear such as that observed in the present case series of IRCTs can be analogous to those smaller retear cases after rotator cuff repair surgery. Furthermore, it is also possible that the improvements observed in some of our patients were associated with the acromioplasty or resulted from a tuberoplasty effect. The improvement in pain was observed in patients with massive rotator cuff repair after a failed dermal allograft procedure because the tuberosity is covered by the graft to prevent bone-to-bone contact with the acromion. 41
SCR is still evolving from a surgical technique standpoint, with a wide variety of procedures being reported. 2,5,16,19,28,42,53 To date, debate exists about whether a side-to-side graft repair to the adjacent remaining rotator cuff is necessary. 20,30,40 The side-to-side graft repair was performed with the premise of having complete restoration of shoulder stability, which was supported by a previous biomechanical study. 40 Our study revealed that the side-to-side repair of the graft to the remnant native tissue had a high failure rate. Lee and Min 30 described the side-to-side repair of the graft to the posterior remnant tissue in their retrospective series and showed that remnant tissue is mostly poor quality. Perhaps the cause of side-to-side repair failure of the SCR is associated with the poor quality of the native tissue.
The decision to use an autograft or allograft in SCR is commonly decided by the advantages and disadvantages in individual cases as well as the surgeon’s preference, and it depends on the political and regulatory issues that vary among countries. Allograft use has had its own innate limitations in lower biological properties compared with autograft when certain types of sterilization were used. 8,47 However, allografts have historically been used during orthopaedic procedures because of lower donor-site morbidity and shortened surgical times. 47 These advantages have resulted in an increased utilization of allografts over the past decade. 13
All tendon grafts, whether autogenous or allogenous, undergo the same process of tissue integration, with graft necrosis, revascularization, cell repopulation, and remodeling. 21 The literature has shown that the incorporation of an allograft in the knee occurred more slowly and less completely in an animal study. 22 A clinical comparative study assessed the early versus late surgical outcome of patients with anterior cruciate ligament reconstruction using an allograft. 43 The study showed that the functional outcome was favorable and remained consistent at long-term follow-up. The present case series demonstrated limited incorporation of the Achilles tendon--bone allograft, which was reflected in the high failure rate. The histologic analysis of the failed graft demonstrated poor vascular ingrowth, which perhaps led to poor healing potential. 50,52 It is possible that the specific type and dose of sterilization, particularly gamma irradiation, may have contributed to the graft failure. Another consideration is the poor vascularity of the native tissue used for the anterior and posterior repair.
Study Limitations
The limitations of the current study follow. First, the study was a retrospective case series with a small sample number; patients were few because the Achilles tendon–bone allograft was not used after the negative results of 6 consecutive patients. Statistical analysis was not performed because of the small sample size. Second, surgical outcomes were based on an early result. Surgical outcomes are reported at a short-term follow-up because of the end point of the study (ie, failed graft). Third, performance bias was possible, as the outcomes represented the experience of a single surgeon who specializes in shoulder surgery. Despite the limitations, surgeons may benefit from the current study in terms of weighting their decision to choose a particular SCR graft type.
Conclusion
SCR using an Achilles tendon–bone allograft for the treatment of IRCTs has limitations that show a considerable graft failure rate.
Footnotes
Acknowledgment
The authors thank Jong-Hwee Park, CNS, for her assistance in medical data collection.
Final revision submitted November 13, 2020; accepted December 14, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Basic Science Research Program through the Asan Institute for Life Sciences funded by Asan Medical Center (2020IL0044). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Asan Medical Center (ref: S2020-0342-0001).