
Abstract
Background:
Meniscus root repairs are important for restoring knee function after a complete meniscus root tear. Various suturing patterns have been proposed for the root repair. The 2-simple-stitches (TSS) method is currently the preferred technique, as it is simplest to perform and allows the least displacement of the meniscus root.
Purpose:
To compare the biomechanical properties of a posterior medial meniscus transtibial root repair consisting of an all-inside meniscal repair device (AMRD) construct with the TSS pullout suture pattern.
Study Design:
Controlled laboratory study.
Methods:
Ten pairs of cadaveric medial menisci were prepared with 1 of the 2 constructs. The constructs were randomized between pairs. All constructs were subjected to preloading with 2 N for 10 seconds and then cyclic loading from 5 N to 20 N for 1000 cycles at a frequency of 0.5 Hz. Subsequently, the menisci were loaded to failure at a rate of 0.5 mm/s. All loads were applied in-line with the circumferential meniscal fibers near the posterior medial meniscal horn.
Results:
The mean yield load and stiffness were similar for both constructs. The elongation after cyclic loading was greater for the AMRD. The displacement at both yield load and ultimate failure were also higher for the AMRD. The ultimate failure load of the AMRD was also significantly higher. During load to failure, the mode of failure in the AMRD was heterogeneous. All the TSS constructs failed by suture cutout.
Conclusion:
Posterior medial meniscus root repairs using both the AMRD and TSS constructs have elongation under the biomechanically acceptable threshold of 3 mm. The stiffness and yield loads indicate similar mechanical properties of the constructs. However, the significantly higher elongation for the AMRD leaves the TSS method as the preferred option for transtibial repairs. Despite this, the AMRD construct may still represent a viable alternative to the TSS suture pattern, comparable to alternative suture patterns with similar limitations.
Clinical Relevance:
The AMRD construct may represent a viable alternative to the TSS suture pattern.
Keywords
The primary function of the meniscus is to convert linear joint stresses into hoop stresses, distributing the joint loads to protect articular cartilage. 6,10 Complete medial meniscus root tears render the circumferential fibers of the meniscus nonfunctional. Recent studies identify the importance of root repair, 3,16,27 given its potential to restore meniscal function. 24 The biomechanics of various transtibial pullout suture root repair constructs have been reported. 4,5,7,13,25 The 2-simple-stitches (TSS) pattern is generally regarded as the gold standard, as other suturing methods display higher elongation under cyclic loading. 2,18,22 However, most studies report that the TSS method has lower yield and ultimate failure loads than other techniques. 4,14,19,21
This study compared the biomechanical properties of a novel all-inside meniscal repair device (AMRD) construct with a TSS pullout suture pattern. The AMRD consisted of 2 Ultra FasT-Fix devices (Smith & Nephew), an AMRD system using a pre-tied, self-sliding knot between 2 polyether ether ketone soft tissue lugs on a No. 0 ultra–high molecular weight polyethylene braided suture (Ultra-Braid; Smith & Nephew). 26 While such devices can be technically easier and faster to utilize in peripheral meniscal repair, 1,8 their potential use as regards root repair has not yet been explored. Our null hypothesis was that there would be no difference between the cyclic elongations, failure loads, or stiffness of the AMRD and TSS constructs.
Methods
Specimen Preparation and Mounting
In this matched-pair cadaveric laboratory biomechanical analysis, 10 pairs of fresh-frozen cadaveric knees (4 male knees, 6 female knees; mean age, 54 ± 4 years) were obtained (ScienceCare), and the left and right medial menisci were harvested via sharp dissection from the tibial plateau. 14,21 Each pair received either a TSS with a No. 2 nonabsorbable suture (Ultra-Braid; Smith & Nephew), a suture similar to that used in comparable studies, 3,4,7,14 or an AMRD on the posterior horn. An even number of left and right medial menisci were allocated randomly to each construct. The TSS suturing pattern was chosen as the comparator because it appears in all comparable literature and generally features the lowest elongation. 4,7,14,21
The TSS suture pattern was undertaken as previously described 14 (Figure 1A). The technique proposed for the in vivo insertion of the AMRDs is described by Kodama et al. 18 The AMRDs were inserted to mimic the positioning achieved using this technique 18 (Figure 1B), with entry of the introducer on the superior surface and exit on the posterior surface (Figure 1C). It is noted that 2 devices are used in the current study instead of the single device used in the study by Kodama et al. This makes the AMRD technique more comparable with other doubled suturing techniques appearing in the literature, such as 2 double loop-locking sutures 4,21 or 2 modified loop stitches, 14 which generally provide better strength and stiffness properties than their single technique counterparts.

Images of (A) the TSS construct and (B-D) the AMRD construct. (C) The position of the introducer for the first device is shown. (D) More detail for the application of the AMRD is shown schematically. AMRD, all-inside meniscal repair device; TSS, 2-simple-stitches.
The mounting protocol was similar to previously described methods 7,12,14,19,21 with the body of the menisci clamped 10 mm from the insertion of the sutures in the meniscus 7,12,21 (Figure 2B). The tissue clamp was fixed to the mechanical testing machine base (ElectroPuls E10000; Instron). The suture tails of the TSS and AMRD were tied around an 8 mm–diameter horizontal pin, which was attached to the linear actuator of the mechanical testing machine via a 1-kN load cell (Instron) using multiple square knots 13,14,19,25 (Figure 2). The free length of suture from the pin to the insertion in the meniscus was set to 40 mm before each test (Figure 2B). The menisci were mounted so that the load was applied parallel to the fibers of the posterior meniscotibial ligament. 14 The mounting and testing were performed at room temperature, and the specimens were kept moist with saline solution.

Photographs of test fixture showing (A) the meniscus fixed in the test clamp and the sutures tied over the 8-mm pin, which is fastened to the 1-kN load cell, and (B) the distances between the insertion point of sutures in the meniscus and the pin at the start of each cyclic test.
Biomechanical Testing
Cyclic Loading. Each specimen was subjected to cyclic loading as follows: preload of 2 N for 10 seconds followed by cyclic loading from 5 N to 20 N for 1000 cycles at a frequency of 0.5 Hz. Elongation after cyclic loading was considered the only clinically relevant parameter during this loading regime. The elongation after cyclic loading measures the change in length of the total construct (ie, between the clamp and the pin) (Figure 3). This methodology was adopted from previous biomechanical root repair evaluations and is designed to mimic in vivo postoperative loads after repair. 14 Note that elongation after cyclic loading replaces cyclic displacement 7,14,21 used in previous papers to clearly distinguish this measurement from displacements analyzed in load-to-failure testing.

Representative cyclic loading curve using WaveMatrix. The inset details the cyclic nature of loading. The elongation after cyclic loading is annotated in red.
Load-to-Failure Testing. After cyclic loading, the menisci were loaded to failure at a rate of 0.5 mm/s until failure. 4,14,21 The following results were analyzed: yield load; displacement at yield load; ultimate failure load; displacement at ultimate failure; and the stiffness of construct. The yield load was defined as the first substantial deviation from linearity of the load-displacement curve (Figure 4). The ultimate failure load was defined as the highest peak in the load-displacement curve before total failure of the construct (Figure 4). Finally, the linear stiffness of the constructs is defined as the slope of the load-displacement curve in the linear elastic region (Figure 4). The mode of failure was also determined by visual inspection for each test.
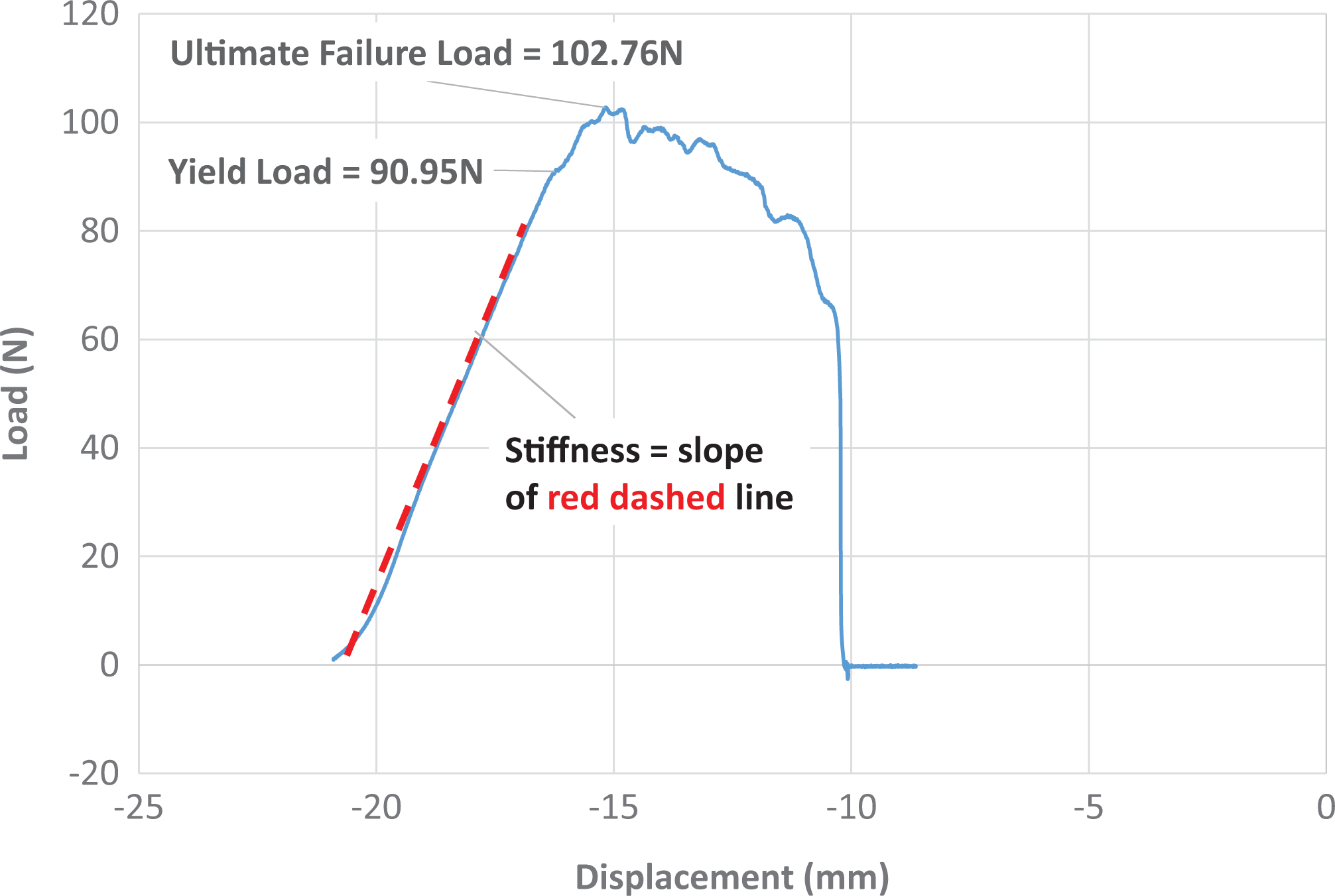
Representative load-to-failure curve collected using WaveMatrix. Shown are distinct yield and ultimate failure loads. The stiffness was calculated as the slope of the red dashed line.
WaveMatrix software (Instron) was used to control the mechanical testing machine and record the test data. It is noted that all elongations and displacements were determined from the WaveMatrix raw data, consistent with all existing literature on meniscus root repairs, which considers any machine compliance negligible. 4,7,14,21
Statistical Analysis
In the cyclic testing, 1 specimen from the TSS group was confirmed as an outlier via several test methods 9,11,15,28 and removed from the analysis for only the cyclic testing. A Student t test was used to analyze these results. The load-to-failure testing was run as a separate test, allowing for all data to be analyzed with a paired t test. The difference in results was considered statistically significant if P < .05.
Results
The results for all cyclic and load-to-failure testing are summarized in Table 1.
Comparison of Biomechanical Properties a

a Data are reported as mean ± SD. Bolded P values indicate statistically significant difference between groups (P < .05). AMRD, all-inside meniscal repair device; TSS, 2-simple-stitches.
Cyclic Loading
During cyclic loading, there were no failures in either construct. The elongation after cyclic loading of the AMRD construct was significantly higher than the TSS construct (P = .004) (Table 1 and Figure 5).

Boxplot showing the elongation after cyclic loading of the constructs. The box represents the interquartile range (IQR) (quartile 1 [Q1] to Q3), the black diamond represents the mean, the horizontal line the median values, and the error bars represent the minimum and maximum (calculated as Q1 – 1.5 × IQR and Q3 + 1.5 × IQR). The circle indicates an outlier. AMRD, all-inside meniscal repair device; TSS, 2-simple-stitches.
Load-to-Failure Testing
The yield load and stiffness of the AMRD construct were similar to the TSS construct (P = .19 and P = .89, respectively) (Table 1 and Figure 6). The AMRD had significantly higher values than the TSS for all other parameters (Table 1 and Figures 6 and 7).

Boxplot showing the (A) ultimate failure load and (B) displacement at ultimate failure load. The box represents the interquartile range (IQR) (quartile 1 [Q1] to Q3), the black diamond represents the mean, the horizontal line the median values, and the error bars represent the minimum and maximum (calculated as Q1 – 1.5 × IQR and Q3 + 1.5 × IQR). AMRD, all-inside meniscal repair device; TSS, 2-simple-stitches.

Boxplot showing the (A) yield load and (B) displacement at yield load for the all-in meniscal repair device and 2-simple-stiches constructs. The box represents the interquartile range (IQR) (quartile 1 [Q1] to Q3), the black diamond represents the mean and horizontal line the median values, and the error bars represent the minimum and maximum (calculated as Q1 – 1.5 × IQR and Q3 + 1.5 × IQR). AMRD, all-inside meniscal repair device; TSS, 2-simple-stitches.
All of the TSS constructs failed by the sutures pulling through the meniscal tissue. The mode of failure for the AMRD constructs was heterogeneous with the sutures snapping at the square knot tied near the 8-mm pin in 5 cases, the sutures snapping at 1 of the lugs in 2 cases, and the remaining 3 failing when the sutures and lugs from 1 of the AMRDs pulled through the meniscal tissue.
Discussion
In this investigation, the TSS constructs had less elongation, higher ultimate failure load, less displacement at ultimate failure with similar yield load, and linear stiffness compared with the AMRD construct.
Use of the AMRD construct for transtibial meniscus root repair is a novel application for an AMRD, and as such, the AMRD and TSS represent 2 very different root repair methodologies. The Ultra FasT-Fix devices used in this study rely on the resistance to pullout of the lugs, which are passed through the meniscus during insertion. The sliding knot connecting the 2 lugs is tightened and secured, gripping the meniscal tissue between the 2 lugs and providing additional resistance to failure by pullout through the meniscus (Figure 1D).
However, in this study, this complex mechanism is prone to increased elongation. This might be due to the continued tightening of the slip knot under load combined with the complex interaction of the lugs with the meniscal tissue. This combination of increased construct complexity and higher elongation has been observed in studies looking at alternative suture patterns. 4,14,21 It is for this reason that the TSS has been recommended as a technically simpler suture pattern benefiting from a combination of lower elongation and reasonable ultimate failure load compared with other suture patterns such as horizontal mattress suture or modified Mason-Allen suture. 7,14
The differences between the constructs are reflected in the mode of failure observations, with the TSS constructs all cutting through the meniscal tissue, while the suture failed in most of the AMRD constructs. Yet, despite these differences, both constructs performed adequately compared with established biomechanical benchmarks. There was elongation after cyclic loading for both constructs of less than 3 mm, the threshold for maintaining biomechanical function of the meniscus. 7,14,21 Although the elongation was acceptable for both constructs, it was significantly higher for the AMRD construct (P = .004).
The linear stiffness of the constructs was similar (P = .89). The linear stiffness of the TSS has been reported as higher than other common suture patterns. 18 A higher linear stiffness of meniscal repair constructs during load-to-failure testing is considered desirable from a clinical perspective. 4,14
The yield and ultimate failure load parameters are less clinically relevant than the elongation and stiffness properties, as they are typically well in excess of the loads generated during early rehabilitation protocols. 13,20 However, they still provide some indication of the relative strength of the constructs and a point of comparison with previous literature. 4,7,21 The yield loads were similar for the 2 constructs (P = .188), indicating similar fixation strength under extreme loading conditions. However, the displacements at yield load were significantly higher for the AMRD (P = .018) and were all well in excess of the 3-mm threshold for both constructs, underlining the importance of low loading during early rehabilitation. 22,23
The TSS pattern was chosen as the comparator as it has consistently demonstrated the least elongation after cyclic loading when compared with more complex suture constructs. 7,14,21 The elongation after cyclic loading for the TSS construct in the current study is consistent with the cyclic displacement after 1000 cycles recorded in LaPrade et al, 21 which also used human cadaveric tissue but with increased cyclic loads (5-20 N vs 10-30 N 21 ).
There were some differences between TSS results in this study and those in the existing literature. For instance, the stiffness values of the TSS constructs recorded in this study (24.5 N/mm) lie midway between the pre- and post-conditioning stiffnesses of 20.6 N/mm and 31.5 N/mm recorded in Anz et al, 4 where the first reading is before any loading of the tissue and the second has been subjected to cyclic loading immediately before pullout testing. In contrast, the current study used 2 separate programs for the cyclic loading and load-to-failure protocols, resulting in a delay between the 2 tests, which would allow some relaxation of the construct.
The yield and ultimate failure loads for the TSS recorded in this study were also lower than those found in similar studies. This may be due to the greater age of the donors (53 vs 24 years 21 ) and the different suture type, both of which potentially have a negative impact on the failure results. The TSS sutures used in this study were No. 2 UltraBraid compared with No. 2 FiberWire (Arthrex), 4,7,14,21 while the AMRD used No. 0 UltraBraid. The UltraBraid has no central core and a different braiding pattern compared with the FiberWire, 17 which results in lower initial stiffness and higher deformation as the braiding aligns itself with the applied load.
Limitations
There are several limitations associated with the current study. Most notably, the meniscus was removed from the tibia before applying the root repair constructs. This means that the techniques were not applied arthroscopically, to replicate in vivo surgery. 4 Instead, the menisci were fully excised before the techniques were applied. This has three implications:
The loading vector during testing is not representative of physiological loading on the construct (however, there are several other papers 7, 12, 14, 19, 21 that use a similar loading protocol).
The comparison of parameters such as time for repair and ease of use were not able to be assessed. In particular, removal of the meniscus from the tibia made it impossible to assess how easily the technique can be applied in vivo.
There was difficulty securing the AMRD construct in the testing jig without loosening of the sliding knot at the meniscal tissue interface. The degree of loosening was not measured during testing. It is noted that the manual for the AMRD devices 26 details several methods for securing this sliding knot in vivo for meniscal repairs. Removing the meniscus from the tibia before applying the constructs made it impossible to determine whether these same techniques would secure the sliding knot for the proposed root repair technique.
Another limitation was that the testing was conducted on cadaveric tissue, which cannot take into account the change in performance due to biological repair mechanisms. As with similar studies, this time-zero study can model only the performance of the construct during immediate postoperative rehabilitation. 4,7,14,21 While cadaveric tissue similar in age to patients undergoing root repair was used, it is likely that cadaveric tissue may hold a suture to a lower load than in noncadaveric meniscal tissue. However, the matched pair design of this comparison study still highlights the differences between the 2 different fixation techniques.
The failure to assess the slippage in the square knot tied near the 8-mm pin is also a limitation of this study. However, the study aimed to assess the elongation and displacement of the constructs as a whole, rather than identify local points of failure.
As noted earlier, the suture sizes were not the same for the 2 constructs, with No. 2 sutures used for the TSS construct and No. 0 sutures used for the AMRD construct. This limitation arguably may lead to some biasing of the results. However, it was thought important to use sutures in the TSS of comparable size with those used in similar studies. 4,7,14,21 The size of the sutures in the AMRD construct is fixed.
Finally, only the TSS construct was used for comparison in the current study. However, the TSS has been recommended as the optimum pullout suture pattern as it is both less technically difficult and has less cyclic elongation than other techniques. 14,18,22
Conclusion
This time-zero study showed that the TSS provides significantly lower elongation than the AMRD. The displacement at yield and ultimate load was also lower for the TSS. The 2 techniques had similar stiffness and strength and both recorded elongations below 3 mm, which has been adopted as a threshold for biomechanical performance. 7,14,21 These results indicate that the TSS should remain the preferred method for medial meniscus root repair, but the AMRD construct may be an acceptable alternative. However, further in vivo studies are required to confirm the appropriateness of the AMRD method.
Footnotes
Final revision submitted October 29, 2020; accepted November 29, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: Smith & Nephew provided the funding for this study as well as donating the devices and sutures. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Macquarie University (ref: 5201300835).