
Abstract
Background:
The comparison of clinical outcomes of arthroscopic footprint-preserving knotless single-row repair with the tear completion repair technique for articular-sided partial-thickness rotator cuff tears (PTRCTs) remains unclear.
Methods:
A total of 68 patients diagnosed with articular-sided PTRCTs who underwent rotator cuff repair between December 2014 and June 2015 were included. Of the 68 patients, 30 received footprint-preserving knotless single-row repair (group 1) and 38 received the tear completion repair technique (group 2). Preoperative and postoperative assessments were compared.
Results:
Both groups had significantly improved American Shoulder and Elbow Surgeons (ASES) scores (group 1: 48.2 preoperatively to 81.9 postoperatively, p < 0.001; group 2: 47.1 preoperatively to 84.9 postoperatively, p < 0.001) and visual analog scale (VAS) pain score (group 1: 6.0 preoperatively to 0.93 postoperatively, p < 0.001; group 2: 6.1 preoperatively to 1.1 postoperatively, p < 0.001), showing that the two procedures significantly improved postoperative shoulder function. No significant differences were shown in ASES score or VAS pain score between the two groups (p > 0.05). The mean operation time was significantly shorter in group 1 with an average of 48.1 min than in group 2 with an average of 60.4 min (p < 0.001).
Conclusions:
Footprint-preserving knotless single-row repair obtains similar clinical results compared to tear completion repair in the treatment of articular-sided PTRCTs. Footprint-preserving knotless single-row repair may be a convenient choice for the treatment of articular-sided PTRCTs. Randomized controlled studies are needed to investigate whether the footprint-preserving knotless single-row repair yields better long-term outcomes through the protection of the bursal cuff and restoration of the healthy footprint.
Keywords
Introduction
Partial-thickness rotator cuff tears (PTRCTs) are common in orthopedic clinics causing shoulder pain and disability in middle-aged patients. 1 PTRCTs can be divided into three subtypes: articular-sided, intratendinous, and bursal-sided tears. 2 Articular-sided tears are two to three times more common than bursal-sided tears. 3 The optimal treatment of PTRCTs, especially articular-sided tears, remains controversial, although surgical repair is suggested for symptomatic articular-sided tears exceeding 50% of thickness of the tendon to prevent tear enlargement. 4
Many surgical techniques can be applied to articular-sided PTRCTs, including repair following full-thickness conversion and various in situ repairs. 4 –6 According to a traditional method, the remnant cuff tissue is repaired to the original footprint after converting the PTRCTs to a full-thickness tear with remnant debridement. This tear completion repair technique is reported to be satisfactory with good visualization, strain characteristics, and healing rates. 7,8 However, the tear completion repair technique reported in some studies causes some complications including a high morbidity rate and delayed recovery, due to damaged integrity of the tendon. 9 Therefore, some surgeons prefer in situ repair of the torn cuff tissue onto the footprint, which can preserve the normal structure of the bursal-sided tendon. 10 –13 In theory, this procedure can improve biological and biomechanical repair properties with a better healing effect.
Trans-tendon repair is a commonly used in situ repair technique. A cadaveric biomechanical study reported that in situ trans-tendon repair was stronger with less gap formation than the tear completion repair technique. 14 However, the results of a recently published meta-analysis showed that both the trans-tendon repair and the tear completion repair technique demonstrated excellent clinical outcomes with no significant differences in functional scores and other evaluations. 15 Furthermore, some authors have raised concerns about the potential damage to the intact tendon during suture anchor insertion and over-tension after the repair. At the same time, this procedure is relatively complex with poor visualization for surgeons. Therefore, we should try other in situ repair techniques to find the optimal procedure for PTRCTs.
In this study, an in situ repair involving a single-row procedure with knotless sutures was applied. To date, few studies have reported the results of this procedure. Therefore, the goal of this study is to compare the clinical outcomes of arthroscopic footprint-preserving knotless single-row repair with the tear completion repair technique for PTRCTs.
Materials and methods
This study was approved by the Institutional Review Board of Shanghai Tenth People’s Hospital, and informed consent for the procedure and the publication of photographs was obtained from all patients. This was a retrospective study with one operating surgeon. The eligible patient population was 117 PTRCT patients diagnosed by magnetic resonance imaging (MRI) before operation between December 2014 and June 2015. The patients we included had grade III articular-sided PTRCTs (exceeding 50% of thickness of the tendon); the diagnosis was based on their symptoms (pain or shoulder dysfunction), physical examination, and MRI and was finally confirmed by arthroscopy. All patients experienced failed conservative treatment for at least 3 months preoperatively, including activity modification, nonsteroidal anti-inflammatory drugs, physiotherapy, and steroid injection. The exclusion criteria were as follows: (1) prior surgery history on the same shoulder; (2) other severe combined pathologies including chondral damage, Bankart lesions, greater tuberosity fractures, and bicep tendon ruptures on the same shoulder; (3) cases with less than a 1-year follow-up after surgery; (4) severe systemic disease; (5) diabetes with an unsatisfactory control; and (6) excluded by arthroscopy.
A total of 68 patients diagnosed with PTRCTs who underwent footprint-preserving single-row repair or tear completion repair were included. Of the 68 patients, 30 received footprint-preserving single-row repair (group 1) and 38 the tear completion repair technique (group 2).
All operations were performed by the same surgeon, and the patients were placed in the lateral position under general anesthesia associated with interscalene block. Then, standard diagnostic arthroscopy was carried out. The degree of rotator cuff tear, the quality of the bicep tendon, and the integrity of the glenoid labrum were evaluated under arthroscopy. Tenotomy of the biceps was performed in case of bicipital tendinitis. Subacromial decompression and acromioplasty were conducted when subacromial impingement was observed. If we could not get a satisfactory passive shoulder range of motion (ROM) under anesthesia, then capsular release was carried out.
Knotless single-row repair with footprint preservation
The torn rotator cuff was grasped with a bird’s-beak suture passer with a number 2 suture and was repaired to bone in a single row using an inverted mattress suture at 10 mm medial to the tendon edge. Then, the suture was loaded through the anchor eyelet. An anchor insertion site was created near the lateral margin of the rotator cuff footprint using a punch at a 90° angle to the bone surface. The anchor body was inserted through the prepared hole. The suture tension was adjusted to the optimal state before the anchor body was planted below the bone cortex (Figure 1). Arthroscopy was used to assess the articular-sided rotator cuff side, and we repeated the procedure to put in another anchor if necessary.
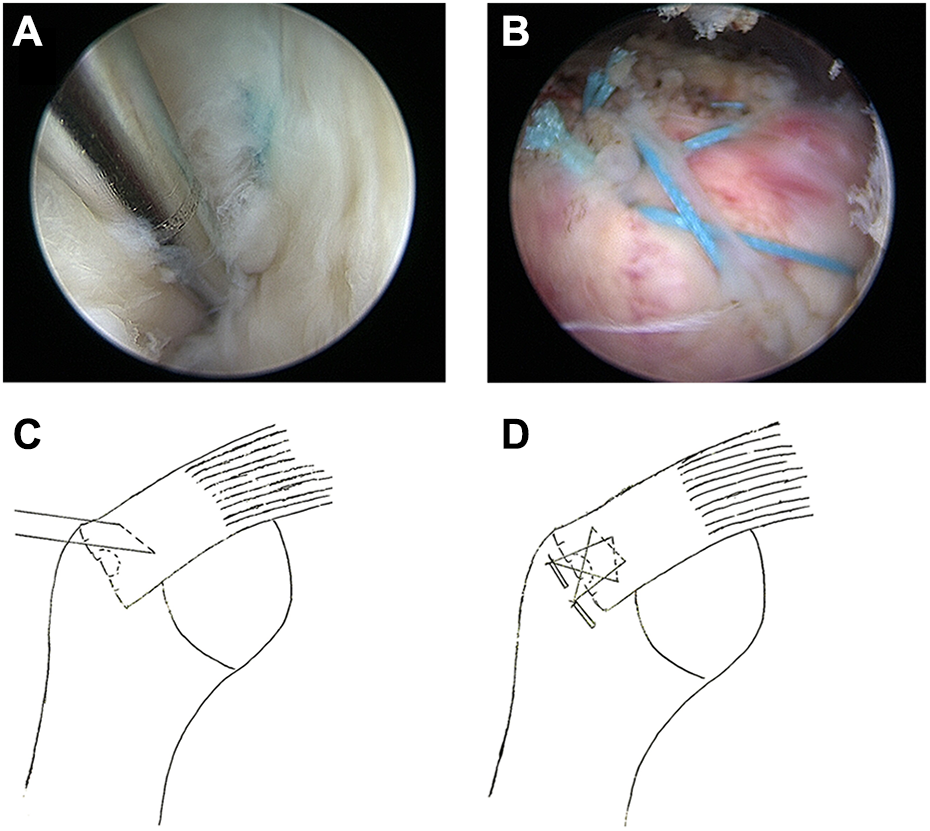
Footprint-preserving knotless single-row repair technique: (a) observed suture pass through supraspinatus under the arthroscope in articular-sided rotator cuff side before locked; (b) completion of the repair using the knotless single-row repair preserving full footprint technique; and (c) and (d) illustration by a diagrammatic sketch.
Tear completion repair technique
The partial articular-sided rotator cuff tear was first converted into a full-thickness tear. Then, the soft tissue of the footprint was cleared up with decortication of the greater tuberosity using a round bur. A single-row repair technique was used by inserting a double-loaded suture anchor in the footprint of the greater tuberosity.
Postoperative rehabilitation
All patients received the same postoperative rehabilitation protocol. A shoulder brace was used to maintain the shoulder at 0° of external rotation and 15° of abduction for 6 weeks. If the patients could tolerate it, they were encouraged to do pendulum exercises and passive gentle ROM exercises to prevent shoulder stiffness. After 6 weeks of shoulder immobilization, the shoulder brace could be removed, and active-assisted ROM exercise was started until 3 months after operation, when active-resisted ROM exercise was allowed. All included patients were asked to maintain a follow-up period of at least 1 year.
Preoperative and postoperative assessment
All patients were evaluated preoperatively and postoperatively within 1 year. All assessments in this study, including the American Shoulder and Elbow Surgeons (ASES) score and the Visual Analog Scale (VAS) pain score, were documented preoperatively and 1 month, 3 months, and 1 year postoperatively. Furthermore, parameters were also collected.
Statistical analysis
All statistical analyses were performed using SPSS version 22 software. Continuous variables were analyzed by paired Student’s t-tests. Dichotomous variables were determined using the χ 2 test. A p value <0.05 was considered significant.
Results
All demographic characteristics of patients are listed in Table 1. No significant differences between the two groups with respect to age, gender, or body mass index (BMI) were reported. There were 8 cases with a mean age of 63.1 ± 6.9 years caused by trauma in group 1 and 11 cases with a mean age of 60.3 ± 6.3 years in group 2. There were six diabetes with a mean BMI of 24.45 ± 3.25 in group 1 and five diabetes with a mean BMI of 23.54 ± 2.72 in group 2. The follow-up time ranged from 12 months to 15 months with a mean of 13 months. No intraoperative or postoperative complications were observed.
Patient information before operation.

BMI: body mass index.
We used two rivets to fix the rotator cuff in 19 patients of group 1 and 20 patients of group 2. None of the patients used three rivets. Under anesthesia, we found five patients with shoulder stiffness in group 1 and six patients with shoulder stiffness in group 2. Tenotomy was carried out in five patients of group1 and four patients of group 2. Group 1 had seven patients and group 2 had nine patients who underwent subacromial decompression and acromioplasty (Table 2).
Number of rivets and intraoperative treatment of two groups.

Some patients showed a favorable repair under MRI 1 month after the operation (Figure 2). At 1 year, both groups had significantly improved functional scores (Table 3). In group 1, the VAS pain score decreased from 6.0 preoperatively to 0.93 postoperatively, and in group 2, it decreased from 6.1 to 1.1. The VAS pain score was not significantly different between the two groups at either time. The mean ASES score improved from a mean of 48.2 preoperatively to 81.9 postoperatively in group 1 and from a mean of 47.1 preoperatively to 84.9 postoperatively in group 2. No significant difference was shown in the ASES score between the two groups, showing that the two procedures significantly improved postoperative shoulder function.

(a) and (b) Partial articular-sided rotator cuff tear marked by blue arrow and black arrow shows the integrity of the bursal side; (c) one month after the footprint-preserving single-row repair, black arrow shows the rotator cuff and red arrow shows the rivet; and (d) one month after the tear completion and repair, black arrow shows the highly edematous rotator cuff, while red arrow shows the rivet.
The function score results of the two groups.

ASES: American Shoulder and Elbow Surgeons; VAS: Visual Analog Scale.
In both groups, patients with acromioplasty postoperative data showed no difference in the ASES score (group 1: 77.4 ± 13.8 vs. 83.3 ± 9.9, p = 0.219; group 2: 84.4 ± 5.3 vs. 85.1 ± 5.9, p = 0.767) and VAS pain score (group 1: 0.6 ± 0.5 vs. 1.0 ± 1.0, p = 0.254; group 2: 1.2 ± 0.7 vs. 1.0 ± 0.9, p = 0.494) compared with patients without acromioplasty.
Furthermore, the mean operation time was significantly shorter in group 1 with an average of 48.1 min than that in group 2 with an average of 60.4 min (p < 0.05).
Discussion
This study investigated the clinical outcomes of two cohorts of patients who underwent either footprint-preserving single-row repair or tear completion repair in the treatment of PTRCTs. No significant difference was observed in the level of pain or functional score between the two groups 1 year after surgery.
PTRCT is the most common type of rotator cuff tear. 16 The optimal surgery method in the treatment of PTRCTs remains controversial. Currently, tear completion repair and the in situ trans-tendon procedure are the two commonly adopted methods. Accumulating studies 4,16 –20 have compared these two procedures. The tear completion repair technique is a traditional method with satisfactory clinical outcomes. 21,22 A partial tear converted to a full-thickness tear could obtain an advantageous healing microenvironment that is similar to an acute full-thickness tear. 5 This technique also had good outcomes in our study, with significantly improved ASES score from 47.1 ± 12.6 to 85.0 ± 5.7 (p < 0.001) and pain relief from 6.1 ± 1.1 to 1.1 ± 0.83 (p < 0.001). Nevertheless, the tear completion repair technique could potentially damage normal tissue, change the normal footprint, and potentially lead to a length–tension mismatch after rotator cuff repair surgery. 23 Therefore, some authors recommend the in situ trans-tendon repair technique, as the bursal-side rotator cuff tendon could be better restored to maintain the tendon integrity, normal footprint, and biomechanical characteristics. 5,23 However, some concerns have been raised about the potential damage to the intact tendon during suture anchor insertion and over-tension after the repair. Moreover, a recently published meta-analysis that included three randomized comparative studies has suggested that in situ trans-tendon repair is an effective treatment for articular PTRCTs, although there were no significant differences between tear completion and repair. 15 Therefore, we applied footprint-preserving single-row repair, which can also restore native footprint and provide good fixation for the rotator cuff.
Usually, rotator cuff tear is accompanied by other pathologies. Seo et al. 24,25 found that articular PTRCTs were correlated with shoulder stiffness, and capsule release at the same time bring a rapid recovery but a similar overall satisfactory results. Another study showed that chronic rotator cuff tears may be a cause of biceps tendinitis. 26 When we found the existence of tendinitis under arthroscope, treatment was necessary. Although we had treated several patients as mentioned above in our study, the sample size was so small that these patients did not have a significant effect on any results.
This study suggests that both surgical techniques could create satisfactory clinical outcomes, with significantly improved functional scores and pain relief. Furthermore, the footprint-preserving single-row repair tended to be more convenient than the tear completion repair technique because the former had a shorter operative time. To date, few studies about the clinical outcomes of footprint-preserving single-row repair have been reported. This procedure can also protect the articular layer to the medial footprint in a way that is akin to the trans-tendon technique; however, it can cause less tension than the trans-tendon technique. In this study, a number 2 suture with a mattress suture was applied, letting us obtain higher footprint contact pressure. Previous studies have reported that repair configurations with a higher footprint contact pressure could significantly decrease the retear rate postoperatively. 27,28 Furthermore, the single-row repair preserving the full footprint can create superior contact pressure of the rotator cuff on the surface of the humeral head than can the conventional single-row repair. 29
Some limitations of this study should be considered. First, this is a retrospective study in which data accuracy and quality are lower than in a prospective, randomized controlled database; therefore, a prospective randomized controlled study is needed. Second, the option of operative techniques produces selection bias, although there was no difference in preoperative statistics. Third, the statistics only included the first year after operation; the long-term clinical outcome and the complications were not assessed. Finally, this study had a relatively small sample size.
Conclusions
In summary, our study demonstrated that there were no significant differences in postoperative VAS pain score or ASES score between the footprint-preserving single-row repair and the tear completion repair in the treatment of articular-sided PTRCTs. Footprint-preserving single-row repair can be curative and convenient. However, due to the small sample size and relatively short follow-up period, whether the footprint-preserving single-row repair can keep the bursal cuff intact and restore the healthy footprint better in the long term than the tear completion repair remains unknown. Therefore, a longer term study with larger sample sizes involving a randomized controlled design is urgently needed.
Footnotes
Authors’ note
Please contact the authors for data requests.
Authors’ contributions
Cen Tao Liu and Heng an Ge contributed equally to this work and should be considered co-first authors. Cen Tao Liu, Heng an Ge, and Biao Cheng conceived the study and participated in its design; Cen Tao Liu, Jing Biao Huang, Rui Hu, Yi Chao Cheng, Peng Wu and Min Wang collected the clinical data; and Cen Tao Liu and Heng an Ge performed the statistical analysis and drafted the manuscript. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Natural Science Foundation of China (grant nos 81372005 and 81401851) and Scientific Research Project supported by the Shanghai Committee of Science and Technology (grant no. 13DZ194808 and 15441904403), Scientific Research Project supported by Shanghai Municipal Commission of Health and Family Planning (No. 20134244), and horizontal research funds from Shanghai Ruiji Trading Company and Shanghai Bojin Kinetic Medical Technology Co. Ltd (No. shrj20170501sy and No. 201705-QP-C1085-011).