
Abstract
Background:
Patients with ruptures of the distal biceps brachii tendon (DBBT) have traditionally been treated via surgical repair, despite limited patient data on nonoperative management.
Purpose/Hypothesis:
To determine the clinical and functional outcomes for patients with partial and complete DBBT injuries treated nonoperatively or surgically through an anatomic single-incision technique. We hypothesized that there would be no difference in outcomes in patients treated with nonoperative or operative management.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective chart review identified all patients with a partial or complete DBBT injury sustained between 2003 and 2017. Surgically treated patients underwent DBBT repair using an anatomic single-incision technique. Nonoperative management consisted of formal physical therapy. The following clinical outcome measures were included for analysis: American Shoulder and Elbow Surgeons (ASES) score; the Disabilities of the Arm, Shoulder and Hand (DASH) upper extremity patient questionnaire; the Single Assessment Numeric Evaluation (SANE) score; and the 36-Item Short Form Health Survey.
Results:
A total of 60 patients (mean ± SD age, 47.8 ± 11.5 years; range, 18-70 years) sustained DBBT ruptures (38 complete and 22 partial) during the study period. Of patients with complete DBBT, 34 were treated operatively and 4 nonoperatively; of those with partial DBBT, 11 were treated operatively and 11 nonoperatively. At a mean follow-up of 5.4 ± 4.0 years (range, 0.5-16.6 years), patients with complete DBBT ruptures achieved overall similar improvements with respect to mean ASES pain, ASES function, SANE, and DASH scores, regardless of whether they were treated operatively or nonoperatively. Subjective satisfaction and functional scores were comparable between the groups. Similarly, at a mean follow-up of 4.1 ± 3.8 years (range, 0.5-11.3 years), patients with partial DBBT injuries had improved mean ASES pain, ASES function, SANE, and DASH scores, regardless of operative or nonoperative treatment. Subjective satisfaction and functional scores were comparable between these groups. For those treated surgically, 5 patients (11.1%) sustained a surgical postoperative complication.
Conclusion:
In our case series, patients were able to achieve satisfactory outcomes regardless of whether they were treated nonoperatively or with an anatomic single-incision approach for complete or partial DBBT ruptures.
Complete ruptures of the distal biceps brachii tendon (DBBT) are relatively infrequent injuries, with a reported incidence as low as 1.2 per 100,000 per year. 22 Although accounting for only 2% to 3% of all biceps tendon tears, these injuries contribute to a significant decrease in supination and flexion strength as well as overall endurance. 19,22 In addition, patients may experience chronic antecubital fossa pain with nonoperative care. 30,31,32 Nonruptured pathologies span a wide spectrum and include chronic tendon degeneration, bicipitoradial bursitis, and partial tear conditions associated with repetitive activity or microtrauma or without a traumatic event.
Complete ruptures of the DBBT typically occur in young active men, particularly those with a history of tobacco smoking and steroid use. 27 While patients who have sustained complete tears may benefit from surgical intervention, low-demand or unhealthy patients may be better suited for nonoperative treatment. 4,8 Thus, when approaching patients with complete tears of the DBBT, particularly in the acute setting, current orthopaedic literature overwhelmingly recommends surgical treatment, despite only limited data being available for a nonoperative approach. 1,3,4,7,9,15,26 Various repair techniques have been developed to match the structural properties of an intact tendon, shedding light on the complexity of managing this unique patient cohort. 6,7,12,17,23,24,32 This places even more importance on patient selection and surgeons’ choice of optimal treatment. 1,4,9 Additionally, the associated risks of surgery, coupled with the published satisfactory outcomes in patients treated nonoperatively, have opened the door for nonoperative treatment in the setting of complete and partial tears. §
In the current study, we sought to report on clinical and functional outcomes in patients with partial and complete DBBT injuries treated nonoperatively or surgically using an anatomic single-incision approach. We hypothesized that there would be no difference in outcomes in patients treated with nonoperative or operative management.
Methods
Patient Selection
A retrospective chart review was performed to identify all patients with complete or partial DBBT injuries. All cases were obtained from the practice of a shoulder and elbow fellowship–trained surgeon (A.D.M.) between November 2003 and December 2017. Institutional review board approval was obtained before initiation of the study. Inclusion criteria consisted of patients aged ≥18 years with a complete or partial DBBT rupture that was managed nonoperatively or via operative fixation. Patients were excluded if they had undergone revision surgery or sustained concomitant fractures other than avulsion fractures of the tendon, as this could confound postoperative pain and outcomes. Likewise, they were excluded if they were representative of a vulnerable population (eg, incarcerated, a patient in a substance abuse facility) potentially subjected to different constraints that could affect their outcomes, follow-up, or ability to make voluntary decisions with respect to research participation.
The decision to pursue operative or nonoperative management is a highly individualized and multifactorial decision, influenced in part by patient factors including activity level, symptom severity, medical history, ability to comply with nonoperative or operative protocols, and patient desires.
Nonoperative Treatment
Nonoperative management included a shoulder sling for comfort (for 2-4 weeks) and formal physical therapy to encourage wrist and elbow strength, specifically elbow supination and flexion. All patients attended a minimum of 1 physical therapy session before completing an individual home exercise program. Patients were encouraged to take nonsteroidal anti-inflammatory medications to assist with pain control and swelling and to return to activity as tolerated when the pain and symptoms subsided. Particular exercises and progression and duration of therapy are at the discretion of the physical therapist and based on patient symptoms. As such, the variability in terms of physical therapists and locations, combined with the limited available data that exist as a result of the retrospective nature of the current study, makes conclusions about interval follow-up and types of strengthening exercises difficult.
Surgical Technique
All patients receiving surgery underwent an anatomic single-incision DBBT repair using a combined soft tissue button and biotenodesis interference screw fixation, as previously described. 18,28 Briefly, the patient was placed in a supine position on the operating table. The operative extremity was set on a hand table in a maximally abducted position to allow for easy fluoroscopic access during the procedure. A single anterior transverse incision was marked approximately 3 finger widths (3-4 cm) distal to the antecubital fossa. Typically, this incision is roughly two-thirds the width of the forearm and can be extended medially or laterally if increased exposure to the radial tuberosity is desired. Blunt dissection was carried out to the level of the avulsed end of the biceps tendon, with caution taken to preserve the lateral antebrachial cutaneous nerve. Once the tendon stump was identified, it was traced proximally to its muscle belly and released circumferentially to allow for increased tendon mobilization. If a partial tear of the distal biceps was visualized, the tear was completed and pulled through the incision at this time (Figure 1A). To do so, a traction suture is placed into the myotendinous junction of the distal biceps (Figures 1B and 2A), and the damaged portion of the tendon is resected.
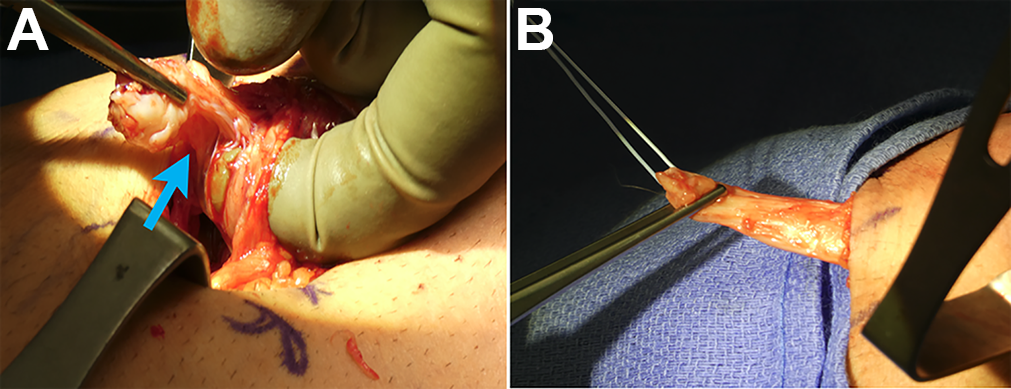
(A) A single anterior incision was made over the elbow joint, and blunt dissection was carried out down to the level of the avulsed end of the biceps tendon (blue arrow, partial tear). (B) If a partial tear was encountered, the tear was completed.

(A) A traction suture was placed into the myotendinous junction of the distal biceps. (B) Preparing of the drill hole (blue arrow). (C) A 4 × 12–mm soft tissue button, either an EndoButton (Smith & Nephew) or a Suture Button (Arthrex) was secured to the tendon. The button was passed through both cortices and the sutures alternatively tensioned to flip the button. Once appropriately positioned under fluoroscopy, the sutures were tied down. (D) Last, a unicortical biotenodesis screw was placed into the radial side of the bone tunnel to push the tendon ulnarly.
The remaining tendon sheath was followed to the level of the radial tuberosity. Forearm hypersupination allowed for protection of the posterior interosseous nerve by positioning it under the supinator muscle and rotating the tuberosity to expose more of the footprint. To better visualize the radial tuberosity, a wide blunt Hohmann retractor could be placed ulnarly and an Army-Navy retractor radially. With adequate exposure now achieved, the tendon stump was prepared for reinsertion. With the tendon tensioned using an Alice clamp, any degenerative tissue emanating from the torn tendon end was removed with Mayo scissors or a skin knife. Tendon length was evaluated to ensure that reduction of the interval was possible. The tendon was stitched on both sides approximately 2.5 cm proximally using locking Krakow stitches. A second nonabsorbable suture was placed centrally in a locking Krakow fashion to facilitate insertion of the cortical button.
Next, an 8 × 12–mm soft tissue button, either an EndoButton (Smith & Nephew) or a Suture Button (Arthrex) (Figure 2, B and C), was secured to the tendon. A 3.2-mm guide pin was then drilled unicortically through the radial tuberosity with the forearm hypersupinated to facilitate placement of the biotenodesis screw (Arthrex). Positioning was confirmed under fluoroscopy. A cannulated reamer was drilled unicortically over the guide wire. The guide wire was removed and drilled through the second cortex at an ulnar angle to protect the posterior interosseous nerve and more anatomically fix the tendon to its insertion site. The button was passed through both cortices and the sutures alternatively tensioned to flip the button. Once appropriately positioned under fluoroscopy, the sutures were tied down.
Last, an interference screw was inserted (8 × 12 mm; PEEK; Arthrex) into the radial side of the bone tunnel to push the tendon ulnarly. The suture limbs were tied down over the top of the screw, and the ends were trimmed to an appropriate length. The deep and superficial components to the wound were closed (Figures 2D and 3), and the elbow was splinted at 90° of flexion and full supination.

Radiographs taken immediately postoperatively to ensure the correct anatomic placement of the tendon. (A) Anteroposterior external oblique view (in external rotation). (B) Anteroposterior medial oblique view (in internal rotation). (C) Lateral view.
Postoperative Rehabilitation
The postoperative splint was replaced with a compression sleeve 3 to 5 days after surgery. Rehabilitation therapy started 1 week after surgery with gentle active motion, including pronation, supination, flexion, and extension. After 2 to 3 weeks, the patient was allowed to resume activities of daily living as tolerated. After 4 weeks, patients were allowed to resume normal activity and were advised to avoid excessive elbow flexion against resistance for 2 to 3 months after surgery. In addition, any strengthening exercises were prohibited for 12 weeks after surgery.
Clinical Outcome Measures
Clinical outcome measures included the American Shoulder and Elbow Surgeons (ASES) and the Disabilities of the Arm, Shoulder and Hand (DASH) upper extremity patient questionnaire. 33 Patient satisfaction assessment included the 36-Item Short Form Health Survey (Physical and Mental Component Summary scores). 31 As preoperative outcome scores were not available for patients who underwent nonoperative treatment, they were collected at only the final visit. A Single Assessment Numeric Evaluation (SANE) score and the DASH upper extremity patient questionnaire were also obtained at terminal follow-up. 20,33 The SANE score was available only for patients treated surgically.
Functional Outcome Measures
Secondary outcome measures included range of motion, specifically active extension, flexion, supination, and pronation. All range of motion measurements were recorded by the same evaluator (A.D.M.) using a goniometer.
Statistical Analysis
Descriptive statistics, including mean and standard deviation as well as median, were calculated to characterize the patient groups. Patients were grouped according to injury severity (complete vs partial) and treatment (operative vs nonoperative). Given the small group sizes for some comparisons, the Wilcoxon rank-sum test was used to examine differences in clinical outcome scores. P <.05 was set to be statistically significant. All analyses were performed with Stata statistical software (Version 15; StataCorp).
Results
Patients
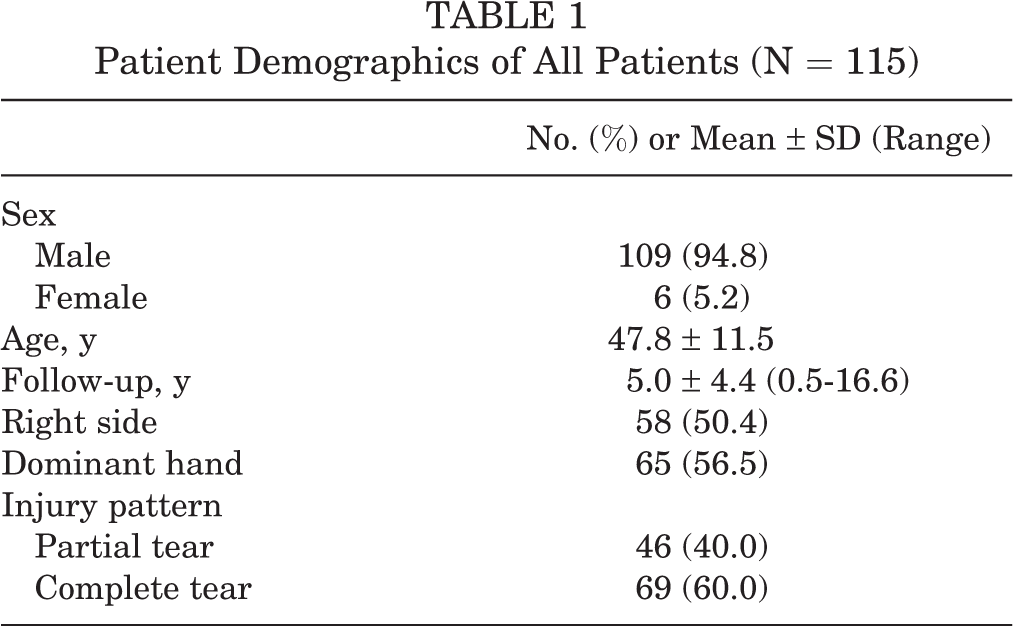
A total of 115 patients undergoing treatment for complete or partial DBBT rupture between November 2003 and December 2017 were identified. Of these patients, 69 (1 woman) sustained a complete tear of the DBBT and 46 patients (4 women), a partial tear (Figure 4). Patients were 47.8 ± 11.5 years old (mean ± SD) at the time of injury and had a mean follow-up of 5.0 ± 4.4 years (range, 0.5-16.6 years). Patient demographics are demonstrated in Table 1. There was no statistically significant difference in age, sex, or follow-up between patients with complete and partial tears.
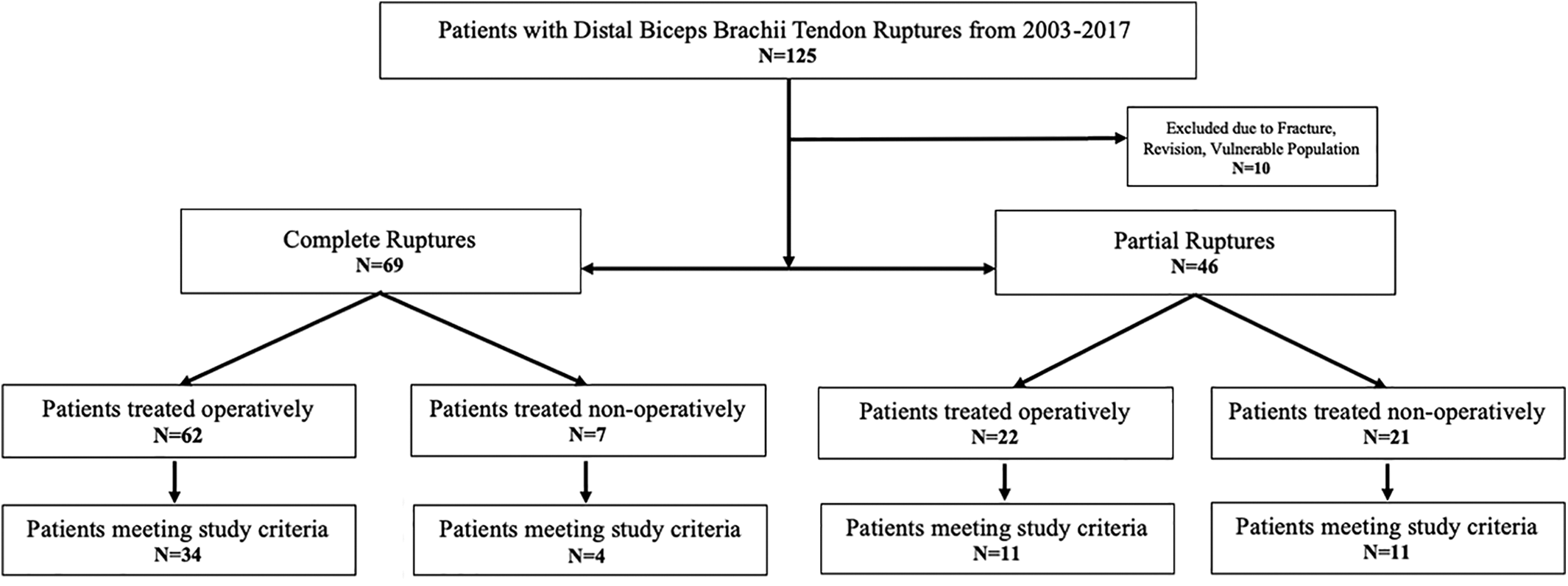
Flowchart displaying patient selection for study inclusion.
Patient Demographics of All Patients (N = 115)
Clinical Outcome Scores
Clinical outcome scores were available for 60 patients (52.2%). Thus, 38 patients (33.0%) and 22 patients (19.1%) who required treatment for complete and partial DBBT tears were included, respectively. Patient descriptions are displayed in Table 2.
Descriptive Data of Patients Included in Final Data Analysis a

a Data are reported as No. or mean ± SD (range). DBBT, distal biceps brachii tendon; NA, not available.
Complete DBBT Tears
At a mean follow-up of 5.4 ± 4.0 years, patients who underwent operative treatment for complete DBBT injuries achieved an ASES pain score of 40.4 ± 12.1, an ASES function score of 45.6 ± 8.3, a SANE score of 93.6 ± 6.8, and a DASH score of 3.4 ± 5.5, all of which were statistically significant improvements as compared with preoperatively (P < .01). Similarly, patients who opted for nonoperative treatment (follow-up, 13.2 ± 2.4 years) achieved similar scores for ASES pain (48.0 ± 4.0), ASES function (44.1 ± 11.8), and DASH (2.1 ± 1.8) (Table 3, Figures 5 and 6). Mean subjective satisfaction, including Physical and Mental Component Summary scores, was comparable between the groups (Table 4).
Clinical Outcome Measures at Last Follow-up a

a Data are reported as mean ± SD. DASH, Disabilities of the Arm, Shoulder and Hand; DBBT, distal biceps brachii tendon; NA, not available; SANE, Single Assessment Numeric Evaluation.
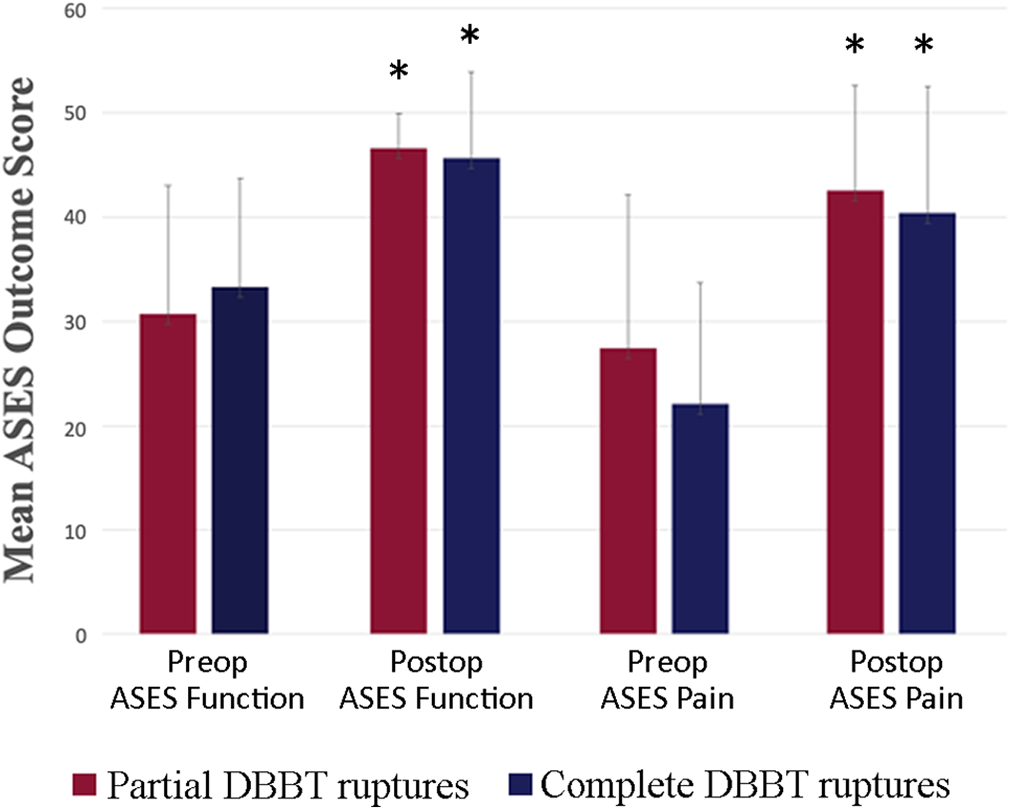
Mean ASES scores for DBBT ruptures treated operatively. Error bars indicate SDs. *Statistically significant improvement (P < .05) when compared with preoperative score. ASES, American Shoulder and Elbow Surgeons; DBBT, distal biceps brachii tendon; Postop, postoperative; Preop, preoperative.
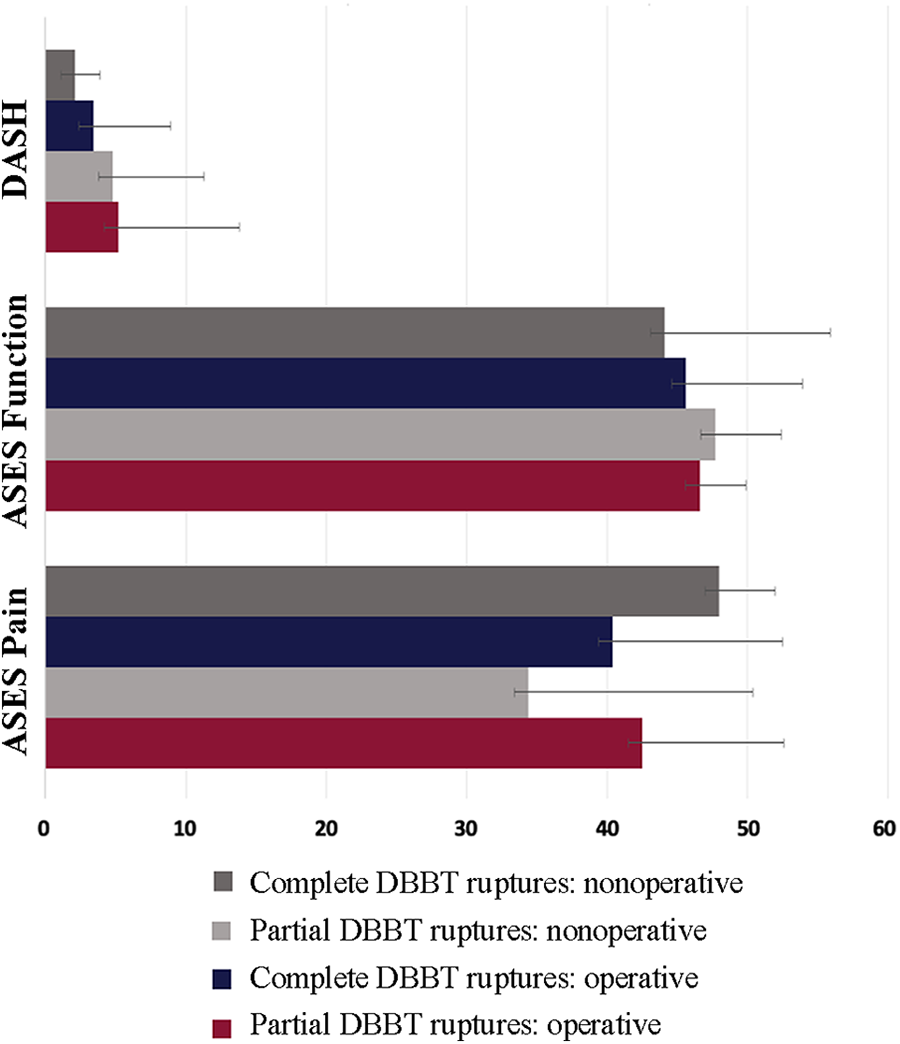
Mean clinical outcomes scores at latest follow-up. Error bars indicate SDs. ASES, American Shoulder and Elbow Surgeons; DASH, Disabilities of the Arm, Shoulder and Hand; DBBT, distal biceps brachii tendon.
Patient Satisfaction for Complete and Partial DBBT Tears a

a Data are reported as mean ± SD. DBBT, distal biceps brachii tendon; NA, not available; SF-36, 36-Item Short Form Health Survey.
Partial DBBT Tears
At a mean follow-up of 4.1 ± 3.8 years, patients who underwent operative treatment for partial DBBT injuries achieved an ASES pain score of 42.5 ± 10.1, an ASES function score of 46.6 ± 3.3, a SANE score of 94.2 ± 5.9, and a DASH score of 5.2 ± 8.6, which were found to be statistically significant improvements as compared with preoperatively (P < .01). Similarly, patients who opted for nonoperative treatment (follow-up, 2.2 ± 2.9 years) achieved similar scores in ASES pain (34.4 ± 16.0), ASES function (47.7 ± 4.7), and DASH (4.8 ± 6.5) (Table 3, Figures 5 and 6). Mean subjective satisfaction, including Physical and Mental Component Summary scores, was comparable between the groups (Table 4).
Patients who underwent successful nonoperative treatment for complete DBBT injuries achieved similar active flexion (126.5 ± 5.9 vs 127.9 ± 8.0), extension (0.5 ± 1.5 vs 0.0 ± 0.0), supination (88.9 ± 2.6 vs 90.0 ± 1.4), and pronation (87.8 ± 6.6 vs 75.8 ± 11.6) as compared with those who underwent operative treatment, respectively.
Surgical Complications
Five patients (11.1%) had complications after surgical treatment of complete or partial DBBT ruptures. By injury type, 2 patients with partial tears had neurologic symptoms of the lateral antebrachial cutaneous nerve, which did not require further treatment and resolved with time. One patient required revision surgery (for rerupture) via the use of an Achilles allograft to repair the ruptured biceps.
Of the patients with complete DBBT tears, 2 had postoperative neurologic symptoms of the lateral antebrachial cutaneous nerve, which also resolved with time.
Discussion
The most important finding of this study was that patients with complete and partial DBBT ruptures treated operatively and nonoperatively maintained satisfactory functional outcomes at final follow-up. In addition, when using the presented anatomic single-incision approach, major postoperative complication rates were low, which is consistent with current literature. 2
Complete DBBT tears typically occur in young, active laborers who undergo large eccentric loading to a fixed elbow, whereas partial DBBT tears may present more discreetly and without a well-defined injury. 16,30,32 When DBBT ruptures are approached nonoperatively, a loss of 21% to 55% in supination strength, 79% of supination endurance, 10% to 40% of flexion strength, and 30% of flexion endurance might be expected. 12,19,29 However, the magnitude of this may not be fully appreciated by a young, sedentary individual or an elderly patient with significant comorbidities. 12 The clinical relevance of losing flexion and supination strength and endurance might be overestimated, as patients (except for high-demand manual workers) may not require surgical repair to restore strength and endurance. Furthermore, the high complication rate reported in the current literature associated with operative treatment calls into question the superiority of operative versus nonoperative approaches. 1,6,7,12,14 As such, the optimal treatment for complete and partial DBBT ruptures remains controversial, 1,3 –5,7 –9,12,15,16 with some evidence suggesting favorable outcomes in low-demand or unhealthy patients treated nonoperatively. 4,8 This is supported by the current study wherein patients with complete and partial DBBT ruptures treated operatively and nonoperatively maintained satisfactory clinical and functional outcomes at final follow-up. However, the majority of patients presenting with complete or partial DBBT tears still opt for operative treatment, which may be inherent to a subsequent Popeye deformity and cosmetic reasons, rather than true functional deficit.
For partial tears, initial intervention includes a period of bracing, rest, and physical therapy, 4,5 particularly when the lacertus fibrosus is intact (Figure 7), for example, which may lend itself to decreased functional deficits. 1,25 Still, in cases of tears refractory to nonoperative management, operative intervention remains a viable option. 3 –5 To that end, a spectrum of repair techniques has been described for DBBT ruptures, reflecting the incertitude of how to best address this injury 6,7,12,17,23,24,32 and that nonoperative management may be reasonable for partial and complete tears. 5,9,10,12,14 –16,19,21,23 However, for partial or complete DBBT tears that are approached operatively, Mazzocca et al 24,28 demonstrated that surgical treatment should attempt to anatomically repair the DBBT to the ulnar aspect of the radial tuberosity to increase biomechanical strength for supination. Additionally, by using the proposed technique, posterior interosseous nerve or lateral antebrachial cutaneous nerve injuries may be reduced. All of the patients having neural affection experienced full recovery; thus, none of them required further intervention. Another advantage of this technique is that patients can initiate postoperative rehabilitation exercises 1 week postsurgically and ultimately transition to the normal activities of daily living at just 2 weeks. As such, range of motion is not compromised postoperatively or at the expense of the repair integrity itself. Subsequently, just 1 patient had reported a postoperative rupture requiring revision surgery. Furthermore, the current study uniquely showcases the clinical outcomes and natural history of partial and complete distal biceps tendon tears as they pertain to nonoperative and operative management.
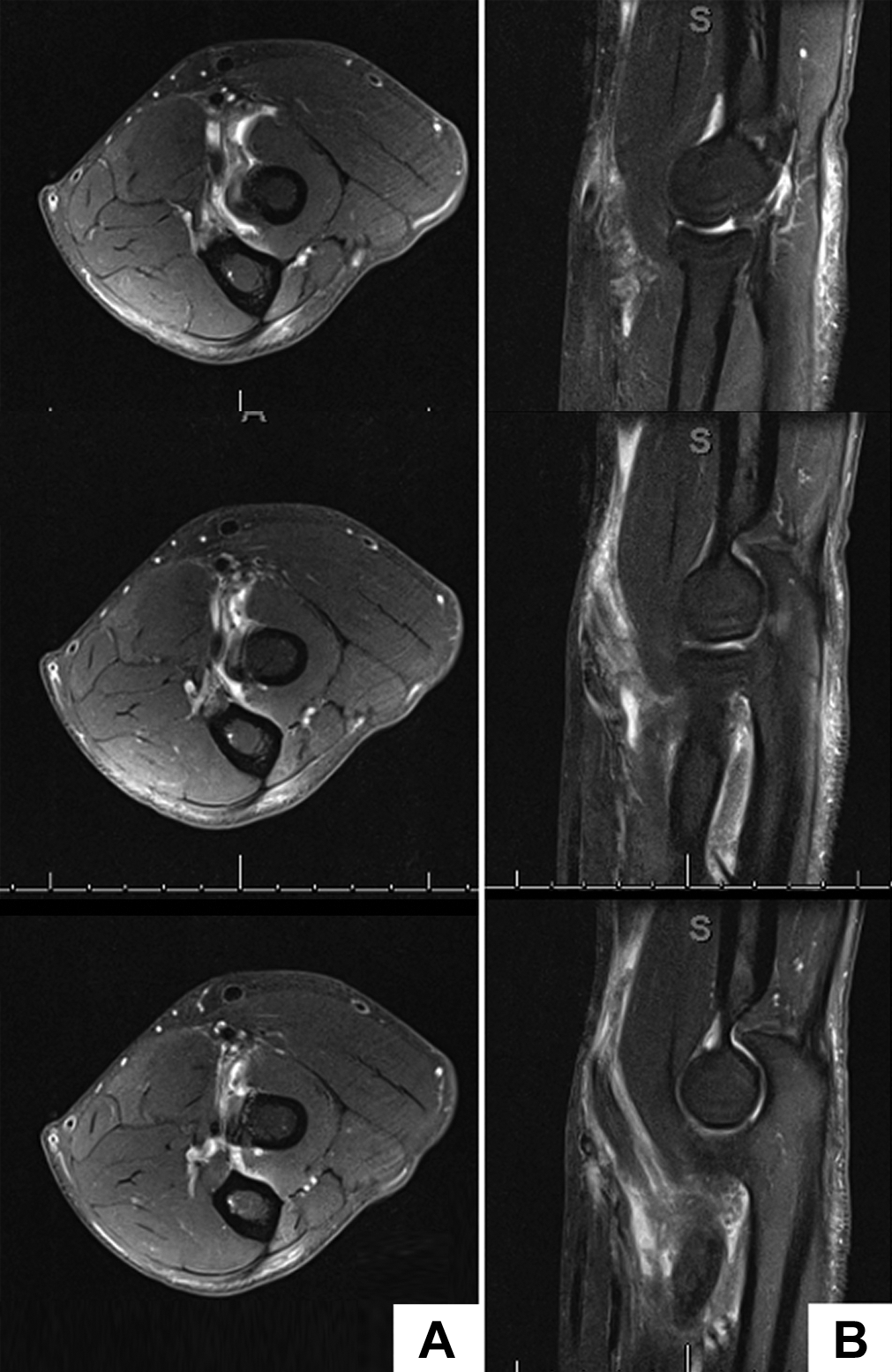
Partial distal biceps brachii tendon rupture on (A) axial and (B) coronal magnetic resonance imaging sequences.
Comparing the results from this study with published data is challenging given the lack of generally accepted standards for follow-up 9 and the small sample sizes 12 found in current literature. For partial DBBT tears, Bain et al 3 reported favorable outcomes with 100% return to normal activities and restoration of muscle strength and normal range of motion in patients treated with a single anterior incision and internal button fixation. Others have advocated for satisfactory outcomes in those patients with partial distal biceps ruptures treated with suture anchors, although this may be at the expense of slight active elbow extension loss. 11 Dürr et al 13 demonstrated that nonoperative treatment in the form of 2 weeks of immobilization and subsequent physical therapy was successful in patients with tears <50% of the insertion. Total functional recovery was achieved in cases refractory to nonoperative management for which tendon reinsertion was carried out. 13 Still, it can be difficult to determine what percentage of the tendon is affected preoperatively. In such cases, surgical treatment is preferred, regardless of the amount of damage.
For complete DBBT, the literature overwhelmingly recommends surgical treatment, despite only limited data being available for a nonoperative approach. 1,3,4,7,9,15,26 In general, depending on the surgical technique, outcomes are satisfactory to excellent, 6,17,21,23,29,32 with low complication rates expected. 2,12
There are several limitations to the study. First, the retrospective study design prohibits a randomized comparison and lends itself to potential selection bias. Moreover, a considerable number of patients did not meet study criteria or were lost to follow-up. This may be due in part to a subset of patients who clinically progressed to the point where further follow-up to see their surgeon (or vice versa) was not felt to be necessary. Still, this is a potential source for transfer bias. Third, minimum follow-up in the current study design was only 6 months, and there were no equal numbers of patients between groups, possibly influenced by the current literature’s portrayal of surgical treatment of DBBT ruptures as the gold standard. Furthermore, cosmesis, rather than true functional deficit, may be a reason to pursue surgical intervention. Additionally, comparing the results using statistical tests between the nonoperative and surgical groups was not possible because of the small sample size of the nonoperative group. Last, the current data set does not include strength testing or power analyses.
Conclusion
In our cohort, patients treated nonoperatively or surgically via an anatomic single-incision approach for complete or partial ruptures of the DBBT achieved satisfactory results at final follow-up.
Footnotes
Notes
Final revision submitted October 8, 2020; accepted November 24, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.A.A. has received research support from Arthrex and consulting fees from Biorez and DePuy. A.D.M. has received research support from Arthrex, consulting fees from Arthrex and Astellas, honoraria from Arthrosurface, and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Connecticut (IRB No. 19-034-2).