
Abstract
Background:
Small-diameter semitendinosus-gracilis tendon autografts may be encountered intraoperatively during anterior cruciate ligament reconstruction (ACLR); these have been shown to be at increased risk of graft rupture. One option that surgeons have pursued to reduce the theoretical failure rate of these smaller-diameter grafts is augmenting them with allograft material, thereby forming a larger-diameter hybrid autograft-allograft construct.
Purpose/Hypothesis:
The purpose of this study was to compare outcomes in adolescent athletes of primary ACLR using a hybrid autologous hamstring tendon and soft tissue allograft construct versus ACLR using small-diameter hamstring tendon autograft. The hypothesis was that the hybrid hamstring autograft-allograft construct would provide superior short-term results.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We performed a retrospective analysis of 47 patients aged between 12 and 20 years who underwent hybrid graft ACLR (mean diameter, 9.1 mm) at a single institution. Electronic medical records including clinic notes, radiographic images, operative notes, and pathology reports were reviewed for study analysis. A control group of 64 patients who underwent small-diameter hamstring reconstruction (mean diameter, 7.1 mm) without allograft supplementation was compiled. Corresponding clinical, radiographic, and surgical characteristics were collected for the control group to allow for comparative analysis.
Results:
Mean follow-up was 2.7 years for the hybrid cohort and 2.3 years for the control group. Despite a significantly larger mean graft diameter in the hybrid group as compared with the control group (P < .001), no significant difference in retear rate was seen between cohorts (hybrid, 9%; control, 13%; P = .554). Patients with hybrid anterior cruciate ligament constructs also underwent a comparable number of reoperations overall (P = .838). Functionally, all patients with adequate follow-up returned to sports, with no significant difference in time to return to sports between the groups (P = .213). Radiographically, hybrid graft constructs did not undergo a significantly larger degree of tunnel lysis (P = .126).
Conclusion:
A cohort of adolescents with hybrid anterior cruciate ligament grafts was shown to have retear rates and overall clinical results comparable with those of a control group that received small-diameter hamstring tendon autografts alone.
Keywords
With increasing rates of participation in youth sports, the incidence of anterior cruciate ligament (ACL) injury and subsequent reconstruction continues to rise in adolescent populations. 5,10,14 Numerous graft options for reconstruction exist. While the use of autologous grafts has inherent drawbacks, such as harvest-site morbidity, increased pain, and longer operating times, literature comparing isolated ACL autograft and isolated ACL allograft techniques has clearly shown that ACL reconstruction (ACLR) using allograft material as the primary graft leads to worse functional outcomes and substantially higher rates of graft failure. 8,9,16,17,19 –21 Therefore, autograft techniques using bone–patellar tendon–bone and quadruple semitendinosus-gracilis tendon constructs have been the most commonly used. However, the use of bone–patellar tendon–bone grafts is largely limited to the subset of adolescents who are near or at skeletal maturity, to avoid the potential for growth disturbance in those with open growth plates. Therefore, soft tissue grafts—by far the most common of which is the quadruple hamstring tendon construct—are often preferred for adolescents undergoing transphyseal techniques. 6
The strength of hamstring autografts has been shown to be proportional to graft diameter, with smaller-diameter grafts having increased failure rates. 3,15 Although the ideal hamstring graft size has not been firmly established, higher failure rates in adolescents have been observed with grafts measuring <8 mm in diameter. 13 Tendon size is difficult to predict preoperatively, and some surgeons may deem harvested hamstring autografts <8 mm to be of inadequate size and consider additional intraoperative steps to address graft size.
One possible technical solution to small harvested autografts is to augment the autologous tissue with allograft tendon material, thereby creating a hybrid graft. Limited research comparing clinical outcomes and failure rates of such hybrid grafts with quadruple hamstring autografts alone has demonstrated somewhat conflicting results, with even fewer studies investigating the adolescent population. 2,7,11,12,17,19,22
The purpose of this study was to analyze the surgical data and postoperative outcomes of adolescent athletes who underwent primary ACLR using a hybrid autologous hamstring and soft tissue allograft construct versus ACLR using a small-diameter autologous hamstring construct. We hypothesized that in this population, hybrid graft ACLR would provide superior results. The aims were to assess the rationale for utilization of hybrid grafts, their dimensions, subsequent radiologic features, and clinical outcomes, particularly when compared with reconstructions using small-diameter hamstring tendon autograft alone.
Methods
After institutional review board approval, a retrospective study was conducted to identify all patients who underwent hybrid ACLR at a large tertiary care pediatric hospital between January 2003 and December 2017, with this end date selected to ensure an adequate follow-up period to capture potential early retear events. Because the chart review was retrospective, no long-term patient outreach was conducted, and no patient-reported outcome measures were collected. Patients between the ages of 12 and 20 years who underwent primary ACLR using standard tunnel placement after an athletic noncontact or contact ACL tear were included in this study. Patients who had unconventional tunnel placement (eg, all-epiphyseal technique modification), a congenital absence of the ACL, or a diagnosed collagen disorder (eg, Marfan syndrome or Ehlers-Danlos syndrome) or who initially presented to the study institution for a revision ACLR procedure were excluded.
Electronic medical records including clinic notes, radiographic images, operative notes, and pathology reports were reviewed for study analysis. Patient demographic and presenting clinical features including age, sex, height, weight, body mass index (BMI), sport, and method of injury were recorded. Preoperative magnetic resonance imaging and plain radiographs were reviewed for coexisting meniscal tears and other pathology, such as bone bruising, chondral lesions, and concomitant medial or lateral collateral ligament injury.
All patients underwent ACLR by 1 of 6 sports fellowship–trained orthopaedic surgeons. Intraoperative details including the presence of any meniscal pathology and ensuing management, tourniquet time, and fixation method were recorded. Dimensions of the initial autograft and those of the subsequent hybrid construct were obtained. Hybrid grafts were constructed by adding 1 of the following soft tissue allograft options: tibialis anterior, tibialis posterior, semitendinosus, or gracilis tendon. In each case, the tendon was folded at the midpoint over the loop of the suspensory loop fixation construct. Postoperative records were reviewed for details related to rehabilitation; timing of return to sports; pain; and complications, such as retear or the need for additional surgery. Patients who underwent meniscal repair were restricted to touchdown weightbearing with crutches and flexion to 90° for 6 weeks. If no meniscal repair was performed, no range of motion or weightbearing restrictions were utilized. Any postoperative imaging obtained ≥6 months was assessed for evidence of tunnel lysis.
A control group of adolescent patients who underwent primary ACLR (mean age, 16.1 years) using solely hamstring autograft with a diameter measuring 7 or 7.5 mm was identified. Postoperatively, patients were treated via rehabilitation programs comparable with those prescribed for the hybrid cohort. The same demographic, clinical, and radiographic measures were obtained for this group over the same study period as that for the hybrid cohort.
Measures of clinical, surgical, and imaging characteristics were summarized using descriptive statistics. The cohort of patients who received hybrid ACLR was compared with the cohort of patients who received small-diameter hamstring autografts alone using Fisher exact tests for categorical variables and independent-sample t tests and Wilcoxon rank sum tests for continuous variables. The significance level was established at P < .05. A power analysis revealed that to detect a difference in retear rate of 5%, a sample size of 1250 patients would be required.
Results
Demographic, clinical, and surgical measures for the hybrid cohort and control cohort are summarized in Table 1.
Clinical and Surgical Characteristics of the Hybrid and Control Cohorts a

a Data are reported as mean ± SD, No. (%), or median [IQR]. Bold P values indicate statistically significant difference between groups (P < .05). IQR, interquartile range; MCL, medial collateral ligament.
b Calculated from patients who received postoperative imaging of the knee at a minimum 6 months (n = 22 for the hybrid cohort; n = 40 for the control cohort).
Hybrid Cohort
A total of 47 patients with a mean age of 15.8 years (range, 12.6-20.0 years; 64% female) and median BMI of 23.8 (interquartile range, 21.2-26.5) were included in the hybrid group. All patients were self-reported athletes who participated in a variety of sports. Of 47 patients, 32 experienced noncontact twisting injuries, 12 experienced collisions, and 3 did not have a documented mechanism of injury.
Intraoperatively, concomitant pathology was appreciated in a majority of patients, as summarized in Table 1. Meniscal tears were seen in 29 of 47 patients (62%), with 8 patients having medial, 13 having lateral, and 8 having medial and lateral meniscal pathology. Eleven patients with meniscal tears underwent partial meniscectomy, while 20 underwent meniscal repair. One medial collateral ligament tear and 1 lateral collateral ligament tear were each treated using open repair. One patient with 1 full-thickness chondral lesion (5 × 10 mm) and 1 patient with 2 lesions (10 × 10 mm and 6 × 8 mm) were treated using microfracture.
Hybrid graft supplementation was used in 42 of 47 patients per the surgeon’s subjective designation of an “inadequate” autograft diameter of the combined semitendinosus-gracilis complex (without recorded details of the 2 tendons’ relative contributions), while length of the gracilis tendon was judged to be insufficient in 5 of 47 patients. In no patient was suture-based doubling, tripling, or quadrupling of the semitendinosus pursued to increase the graft diameter. The mean diameter of the initial autograft was 6.6 mm (range, 5-9 mm) in the 30 patients in whom the exact size was documented. The mean diameter for these allograft portions alone, as reported in the packaging by the external tissue bank, was 6.7 mm (range, 4-8.5 mm). Autograft and allograft hybrid constructs had a mean diameter of 9.1 mm (range 7-11 mm). Tibial interference screw fixation was used in all patients, with a mean screw diameter of 9.8 mm (range, 8-12 mm). Among 22 patients who received postoperative imaging of the knee at a minimum of 6 months after surgery, the tibial tunnel was found to have expanded 33% ± 17% (mean ± SD) from the original size.
Mean follow-up after surgery for patients receiving hybrid graft reconstruction was 2.7 years (range, 0.1-8.4 years). All patients with adequate follow-up detailed in the medical records had documented return to sports, with a median interval after injury of 9.5 months. Revision surgery was performed in 16 patients (34%), with 4 patients requiring a second revision (Table 2).
Number of Complications in the Hybrid and Control Cohorts a
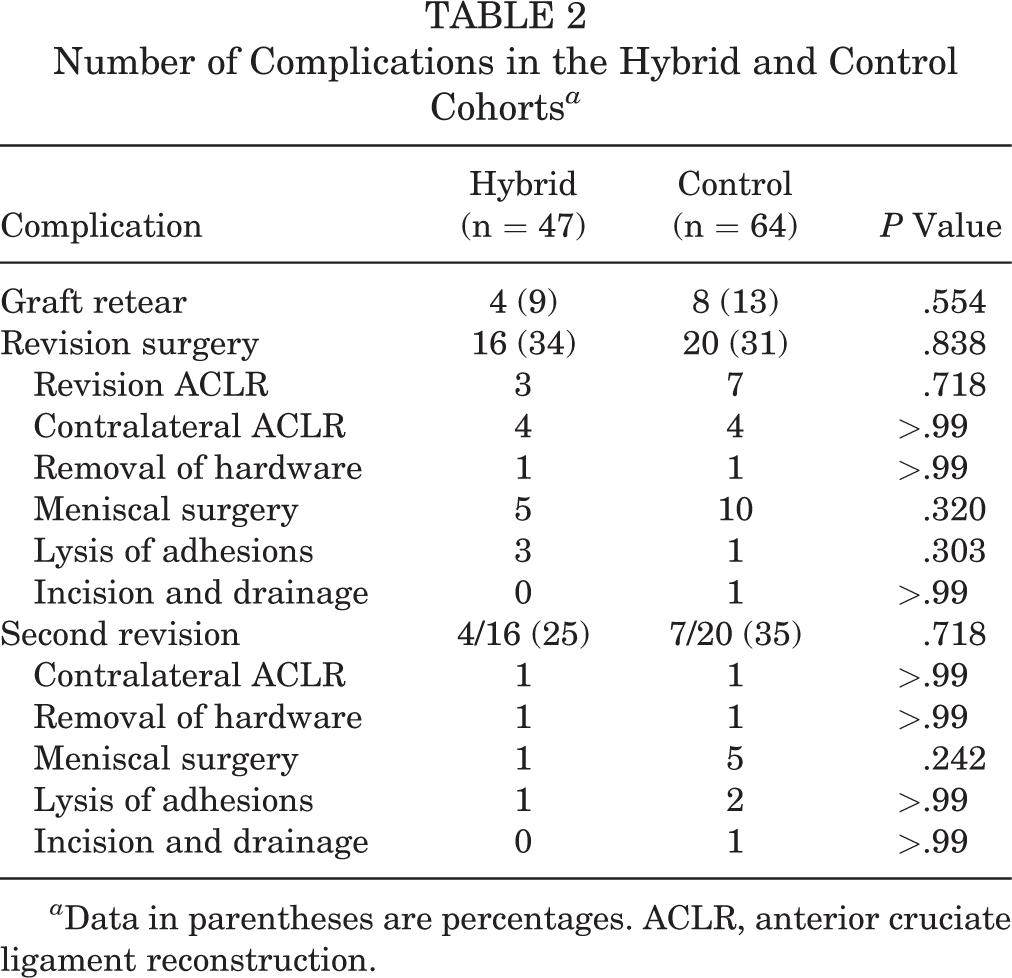
a Data in parentheses are percentages. ACLR, anterior cruciate ligament reconstruction.
Control Cohort
Table 1 summarizes the demographic, surgical, and clinical information regarding the 64 patients in the control group who underwent primary ACLR using autologous hamstring grafts with documented diameters of 7 or 7.5 mm. There were no significant differences between this cohort and the hybrid cohort in age, BMI, affected side, or mechanism of injury. The mean graft diameter of the control group was 7.1 mm, significantly smaller than that of the hybrid cohort (P < .001).
Mean follow-up time was 2.3 years (range, 0.1-6.7 years). All patients with adequate follow-up documentation had returned to sports at a median interval of 9.9 months (interquartile range, 8.4-12.2 months) after injury, an interval not significantly different from that of the hybrid cohort. For the 40 patients who received postoperative imaging at a minimum 6 months after surgery, tibial tunnels had expanded a mean 25% ± 18%, which was not significantly different from that of the hybrid group.
Twenty patients underwent revision surgery, with 7 requiring a second revision. Eight patients (13%) sustained graft rupture, 7 of whom underwent revision ACLR (Table 2). There was no significant difference in graft retear rate between this cohort and the hybrid group.
Discussion
The present study demonstrates that supplementation of insufficient hamstring autografts with soft tissue allograft during ACLR in adolescent athletes produced a slightly lower retear rate, which did not reach statistical significance, when compared with a small-diameter hamstring autograft (9% vs 13%; P = .554). While allograft supplementation may be clinically safe and technically effective in generating a larger-diameter graft, it was not found to enhance outcomes in a statistically significant way. The early retear rates, clinical results, reoperations, and radiographic findings (in the form of tunnel lysis or expansion) were not found to be significantly different from those of a control group receiving small-diameter hamstring autografts alone. Functionally, all patients with adequate documentation of their postoperative follow-up period were reported to have returned to sports, with no significant difference in the time of return to sports between the groups. In addition, both groups had lower retear rates than those previously reported in studies involving hamstring autograft ACLR, 4,18 suggesting that graft size may not be the most important factor in retear rate. Importantly, the mean graft diameter of the autograft before supplementation (6.6 mm) was smaller than that of the autograft of the control group (7.1 mm), so the supplementation may have provided a clinical benefit not detected by the current study methods.
Previous literature comparing hybrid autograft-allograft and autograft-only reconstructions have demonstrated mixed results. Burrus et al 2 and Wang et al 22 found that graft failure, knee stability, and patient-reported outcome scores were all poorer in hybrid groups than in autograft groups. Conversely, Leo et al 11 and Li et al 12 found no significant differences in retear rates or clinical outcomes. Although it is not clear what contributed to the differences in results reported by these authors, possible explanations include variations in surgical technique and use of allograft irradiation rather than chemical-based or non–irradiation based sterilization techniques, which may have affected graft strength or durability. Additionally, these studies were performed primarily on adult populations, with biologic responses to allograft tissue and activity levels that may be markedly different from that of adolescents.
Only 3 previous studies with somewhat conflicting results have investigated the efficacy of hybrid grafts in adolescent patients. Jacobs et al 7 compared 42 patients who received hybrid graft constructs with 46 patients who received hamstring autografts alone. The mean diameter was 9.9 mm for the hybrid graft cohort and 7.8 mm for the autograft cohort. The authors found a significantly lower rate of graft failure among hybrid grafts (12%) versus autografts alone (28%). Explanations for this difference may include the shorter follow-up in the hybrid group or the more recent use of the technique by the authors, who may have optimized other aspects of the overall ACLR or rehabilitation. Pennock et al 17 compared 26 adolescents with allograft supplementation with a mean graft diameter of 8.9 mm and 24 patients with autograft with a mean graft diameter of 6.4 mm. The authors reported that, of patients with initial autografts measuring 6 or 6.5 mm, only larger-sized patients participating in high-risk cutting activities underwent augmentation, suggesting perhaps noncomparable treatment cohorts with different stress levels on augmented versus nonaugmented grafts. At a mean follow-up of 3.0 years, there were 6 hybrid failures (30%) as opposed to 1 autograft failure (5%). Finally, Perkins et al 19 compared 3 adolescent cohorts: 65 patients with 6-strand doubled gracilis and semitendinosus autograft augmented with soft tissue allograft, 198 patients with 4-strand doubled semitendinosus and gracilis autograft, and 91 patients with 5-strand tripled semitendinosus and doubled gracilis autograft. Mean final graft diameters were 8.3 mm for the 4-strand, 8.9 mm for the 5-strand, and 9.2 mm for the 6-strand graft. After adjusting for age and graft size, patients who received hybrid grafts had increased odds of failure when compared with patients who received the 4-strand graft. These authors therefore recommended tripling the semitendinosus graft as opposed to allograft supplementation. Other surgeons have considered supplementation from hamstring harvest on the contralateral knee. Notably, hamstring autografts with a diameter ≥8 mm, as was the average size in the study by Perkins et al, would typically not be considered for supplementation. In contrast, the current study utilized a comparison group with small-diameter autografts to replicate the characteristic decision scenario experienced by surgeons intraoperatively.
One potential concern with reconstructions using allografts, in addition to the higher midsubstance rupture rate than that with reconstructions using autograft tissue, is that the foreign tissue may be associated with slower tendon-to-bone healing, poorer incorporation in bony tunnels, or an adverse osteolytic response. To investigate this, previous studies have used postoperative imaging to assess for tunnel enlargement in autograft and allograft reconstructions. Interestingly, some studies have demonstrated a larger degree of expansion in allografts than autografts, while others have suggested no difference. 20,23 The current study demonstrated slight but not significantly greater tunnel expansion in the hybrid group as compared with the control group. More important, there were no directly observed differences in the clinical outcomes between the groups.
Limitations
One limitation of the current study was that the sample size of the hybrid group was relatively small and therefore underpowered, given the binomial primary outcome measure of retear. Future studies with greater sample size and level 1 evidence methodology may allow for better understanding of relative retear risk, as well as substratified analyses of subcohorts and investigation of particular patient characteristics. Given the emerging findings regarding allograft use in this and similar studies, ethical considerations for such studies are complex. The retrospective nature of the current study, which was nonblinded and nonrandomized, introduced inherent elements of bias, and lacked prospective patient-reported outcome measures; long-term monitoring of complication; and follow-up physical examination maneuvers, such as Lachman or pivot-shift test.
Another limitation was the inherent differences between the study cohorts. While the difference in injury-to-surgery time was statistically significant between graft groups, a difference of approximately 3 weeks should not likely be considered clinically significant. The difference in sex distribution stemmed from the fact that the control group was selected specifically for small graft size. Thus, female participants were likely to be overrepresented in the control group, owing to smaller statures. According to previous literature demonstrating higher rates of ACL injury in female athletes, 1 if a greater percentage of hybrid patients were female, the retear rates may have been higher than those reported in this study, thereby further questioning the advantage of allograft supplementation. Next, the long study period likely incorporated refinements to ACLR technique over time, the effect of which was not assessed. Finally, the control group did not include autografts <7 mm, so no clear conclusions can be made for this rare group. While cohorts matched by preoperative autograft diameter would strengthen the study conclusions, we believe that this investigation still provides valuable insights into the utility of hybrid graft constructs. Continued investigation into the optimal graft choice for adolescent athletes is warranted to minimize postoperative risks, which remain considerable, and to optimize return to activity and quality of life in this young subpopulation.
Conclusion
The current study demonstrated that a cohort of adolescent patients who had undergone ACLR using a hybrid graft consisting of autologous hamstring tendons and soft tissue allograft had comparable outcomes and retear rates with those of a control group that received a smaller-diameter autologous hamstring tendon autograft alone. Despite these results, further investigation to find the optimal graft choice for adolescent athletes is warranted.
Footnotes
Final revision submitted June 11, 2020; accepted July 7, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.E.H. has received educational support from Kairos Surgical, consulting fees from Imagen Technologies, educational consulting fees from Arthrex, and royalties from Springer; has stock in Imagen Technologies; and is a study group member for ROCK, which receives unrestricted educational grant funding from Allosource and Vericel. D.E.K. has received educational support from Kairos Surgical. M.S.K. has received consulting fees from OrthoPediatrics and Ossur; speaking fees from Smith & Nephew; and royalties from OrthoPediatrics, Ossur, Elsevier, and Wolters Kluwer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Boston Children’s Hospital (protocol No. IRB-P00015610).