
Abstract
Background:
Lesions of the long head of the biceps can be successfully treated with biceps tenotomy or tenodesis when surgical management is elected. The advantage of a tenodesis is that it prevents the potential development of a cosmetic deformity or cramping muscle pain. Proponents of a subpectoral tenodesis believe that “groove pain” may remain a problem after suprapectoral tenodesis as a result of persistent motion of the tendon within the bicipital groove.
Purpose/Hypothesis:
To evaluate the motion of the biceps tendon within the bicipital groove before and after a suprapectoral intra-articular tenodesis. The hypothesis was that there would be minimal to no motion of the biceps tendon within the bicipital groove after tenodesis.
Study Design:
Controlled laboratory study.
Methods:
Six fresh-frozen cadaveric arms were dissected to expose the long head of the biceps tendon as well as the bicipital groove. Inclinometers and fiducials (optical markers) were used to measure the motions of the scapula, forearm, and biceps tendon through a full range of shoulder and elbow motions. A suprapectoral biceps tenodesis was then performed, and the motions were repeated. The motion of the biceps tendon was quantified as a function of scapular or forearm motion in each plane, both before and after the tenodesis.
Results:
There was minimal motion of the native biceps tendon during elbow flexion and extension but significant motion during all planes of scapular motion before tenodesis, with the most motion occurring during shoulder flexion-extension (20.73 ± 8.21 mm). The motion of the biceps tendon after tenodesis was significantly reduced during every plane of scapular motion compared with the native state (P < .01 in all planes of motion), with a maximum motion of only 1.57 mm.
Conclusion:
There was a statistically significant reduction in motion of the biceps tendon in all planes of scapular motion after the intra-articular biceps tenodesis. The motion of the biceps tendon within the bicipital groove was essentially eliminated after the suprapectoral biceps tenodesis.
Clinical Relevance:
This arthroscopic suprapectoral tenodesis technique can significantly reduce motion of the biceps tendon within the groove in this cadaveric study, possibly reducing the likelihood of groove pain in the clinical setting.
Pathology of the long head of the biceps tendon is a frequent cause of shoulder pain and can be caused by various pathologies, such as tendinitis, tendon subluxation, tendon dislocation, and superior labrum anterior-posterior lesions. These lesions can be managed nonoperatively or operatively, with nonoperative management often resulting in little functional impairment in the elderly and low-functioning patients. 7 Operative management of the biceps tendon is indicated when nonoperative management has failed or when biceps pathology is encountered during surgical intervention for other intra-articular pathology. Surgical options include tenotomy or tenodesis, with tenodesis typically recommended in younger, more active patients, or when a cosmetic deformity is unacceptable. 5 –7,25
Clinical studies have demonstrated little difference in elbow flexion strength or forearm supination strength between tenotomy and tenodesis. 7,22 The potential advantage of tenodesis over tenotomy is to avoid the development of a cosmetic deformity (“Popeye sign”) 2,15,16,24 and reduce the risk of postoperative cramping, 16,24 which can occur in up to 20% of patients. 2,9
Multiple techniques have been described for biceps tenodesis; the procedure can be performed arthroscopically or in an open fashion, and the tendon can be anchored in either a suprapectoral or a subpectoral position using one of several different methods. ‡ Sanders et al 20 examined several fixation techniques and implicated motion of the biceps tendon in the groove as the cause of tenosynovitis and the ultimate origin of persistent groove pain. To our knowledge, however, to date, no work has quantified the extent of motion of the tendon in the bicipital groove, especially after biceps tenodesis.
The objective of this study was therefore to evaluate the motion of the biceps tendon within the bicipital groove before and after a suprapectoral, intra-articular tenodesis performed using a simple, all-arthroscopic technique. 4 We hypothesized that this proximal biceps tenodesis technique would result in minimal to no motion of the biceps tendon within the bicipital groove after this tenodesis.
Methods
Specimen Preparation
Six fresh-frozen cadaveric arms (5 male; average age, 75.2 years; and 1 female; age, 63 years) stored at –20°C were obtained from the Allegheny-Singer Research Institute using funds from an educational grant for resident research. Each specimen was thawed for 24 hours prior to testing. Each thawed specimen was dissected, free of skin and subcutaneous tissue, to expose the long head of the biceps tendon and the bicipital groove, from the transverse humeral ligament to the pectoralis major tendon insertion. Care was taken to maintain the rotator cuff insertion and glenohumeral joint capsule. The medial half of the scapula was dissected completely to the level of the bone, and the medial aspect of the supraspinatus and scapular spine were removed with a saw. This removal was required for the scapula to be fixed into a custom-made apparatus: the scapula was held stable using 2-part polyester resin adhesive (3M) with 2 wood screws through the medial border and inferior angle. The apparatus was then affixed with 2 inclinometers (A2T; US Digital) to measure scapular motion in the axial and sagittal planes. Two fiducials (DMAS; Spica Technology) were attached with cyanoacrylate adhesive on each side of the bicipital groove 10 mm apart, beginning 10 mm distal to the distal edge of the transverse humeral ligament; 3 additional fiducials were placed on the center of the biceps tendon 10 mm apart, beginning 15 mm distal to the distal edge of the transverse humeral ligament (Figure 1). The 2-camera (ProSilica GC1350C; 1360 × 1024 resolution) system tracked fiducial markers 3-dimensionally using Spicatek software at 10 Hz. The system was calibrated with a 3-dimensional frame measured with an accuracy of 0.005 mm and was tested to measure movements with 0.06-mm accuracy. A third inclinometer (X3Q; US Digital) was affixed to the ulnar shaft with screws to measure elbow flexion and extension (Figure 2).
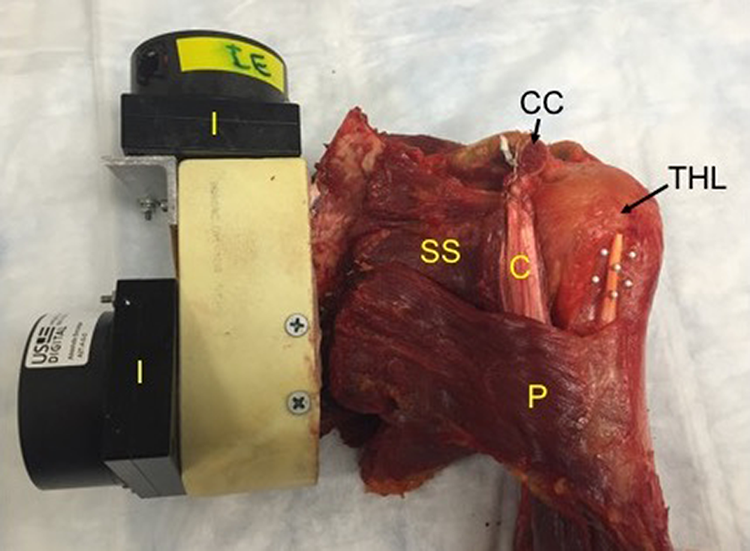
The proximal specimen has been mounted in the custom-made apparatus with inclinometers to measure internal-external rotation and flexion-extension. The long head of the biceps tendon and bicipital groove are marked with white fiducials that can be easily tracked by the cameras. C, conjoined tendon; CC, coracoid; I, inclinometer; P, pectoralis major; SS, subscapularis; THL, transverse humeral ligament.

The middle third of the ulnar shaft was affixed with a third inclinometer (I) to measure elbow flexion-extension.
The distal third of the humeral shaft was exposed via a posterior approach, removing the central portion of the triceps. The humerus was then mounted in the testing apparatus with a clamp anterior and posterior to the exposed bone. Two cameras (Spica Technology) were calibrated to track the motion of the biceps tendon within the groove and mounted above the biceps tendon. The distal biceps tendon was exposed in the antecubital fossa, and a looped stitch was placed into it to allow a resting tension at all times through the distal portion of the tendon to be applied as 5 N in order to reproducibly remove slack and redundancy from the tendon (Figure 3). When the specimen was taken through a full range of motion during preliminary testing, including shoulder flexion, extension, internal and external rotation, and abduction, it was found that the distal tip of the coracoid and the conjoined tendon blocked the visualization of the long head of the biceps tendon during portions of glenohumeral motion. To eliminate this problem, the distal 20 mm of the coracoid was osteotomized and the conjoined tendon was reattached through drill holes in the remaining coracoid while maintaining the length-tension relationship (Figure 1). Abduction and adduction were in the horizontal plane because the humerus was held in a fixed position parallel to the ground and the scapula was moved to adjust motion in this plane. We constructed a large protractor; the center was placed directly under the center of rotation of the humeral head, with the 0° line parallel to the humeral shaft. A large wire was drilled through the scapula, from the inferior angle toward the center of rotation of the humeral head, to visually measure the abduction angle (Figure 4).

A resting tension of 5 N was applied to the distal biceps tendon (DBT) using a manual tensionometer.
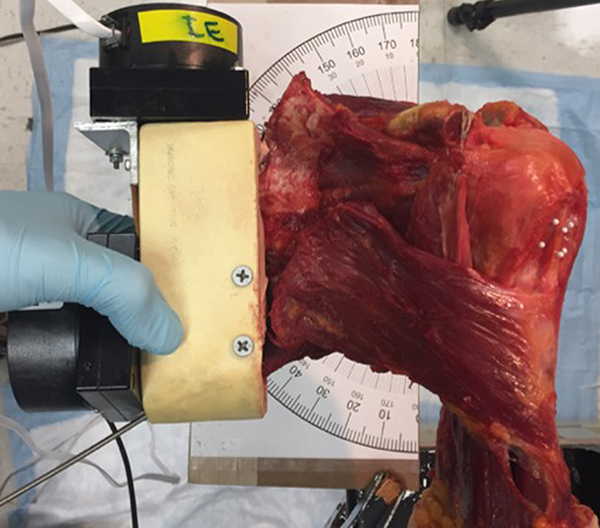
A large protractor was centered under the center of rotation of the humeral head, with the 0° line parallel to the humeral shaft. A wire was drilled through the scapula, from the inferior angle toward the center of rotation of the humeral head.
Measurement of Native-State Tendon Motion
The baseline position of the scapula was defined as 0° of abduction, 0° of internal-external rotation, and 0° of forward flexion-extension; the baseline position of the elbow was defined as full extension and neutral pronation-supination. The inclinometers were all zeroed at this position, and the scapula and forearm were taken through full ranges of motion to ensure proper functioning of the inclinometers and cameras. A resting tension of 5 N was applied to the distal biceps tendon using a spring tensiometer controlled manually, maintained throughout all testing conditions (Figure 3). The exact range of motion that could be achieved in each plane differed slightly for each cadaver, but it was always taken through the maximum allowable range for each plane of motion. Each range of motion cycle described below was repeated 3 separate times for each plane of motion, and the full protocol was repeated for all 6 cadaveric specimens.
Measurements of biceps motion were made using the change in distance between the fiducials on the tendon compared with the ones on the bicipital groove. The motion of the biceps tendon after tenodesis was tested first during elbow motion, with the scapula held in the baseline position throughout all testing conditions. First, the elbow was maintained in neutral pronation-supination and taken through 1 cycle from full extension, to full flexion, and back to full extension. Second, the forearm was maintained in full pronation, and the flexion-extension cycle was repeated. Third, the forearm was maintained in full supination, and the flexion-extension cycle was repeated.
The motion of the biceps tendon during glenohumeral motion was tested second, with the elbow held in the baseline position throughout all testing conditions. First, the scapula was taken from the baseline position, to full internal rotation, to full external rotation, and back to the baseline position. Because the humerus was held in a fixed position, internal rotation of the scapula corresponded to external rotation of the humerus; the results were documented in this way, as range of motion is clinically referenced to the scapula, not the humerus. Second, the scapula was forward flexed from the baseline position, to full flexion, to full extension, and back to the baseline position. To achieve full forward flexion from the baseline position, simulation of scapular protraction was necessary. 18 For this reason, maximum forward flexion was achieved by combining forward flexion with internal rotation of the scapula to re-create scapulothoracic protraction. The range of motion for this third glenohumeral condition was from the baseline position, to full forward flexion with protraction, and back to the baseline position. Fourth, the scapula was abducted from the baseline position, to full abduction, to full adduction, and back to the baseline position. Abduction and adduction were then able to be visually measured and recorded in 10° increments.
Intra-articular Biceps Tenodesis
The suprapectoral biceps tenodesis was performed with a simple, intra-articular, all-arthroscopic technique: the loop ‘n’ tack tenodesis. 4 For the purposes of this biomechanical study, the procedure was performed through a small capsulotomy in the rotator interval in the cadaveric specimens; however, the instruments, technique, and implants were identical to the arthroscopic procedure. See Figure 5 for illustrations of the technique. To summarize the technique, a looped suture was cinched around the biceps tendon near the insertion on the superior labrum. The tail of the suture was then retrieved using a penetrator passed through the center of the biceps tendon, tacking the suture distal to the loop. The biceps tendon was then cut at the labral insertion, and a 3.5-mm Push Lock suture anchor (Arthrex) was used to fix the tendon in the most distally visualized intra-articular portion of the bicipital groove, just above the insertion of the subscapularis tendon. This anchor was placed after a standard drilling technique established the location for the anchor. By cutting the tendon as close to the superior labrum as possible and fixing it right above the subscapularis tendon insertion, this procedure results in taking the biceps tendon slightly off tension. 4

A left shoulder in the lateral decubitus position viewing with a 30° arthroscope from the posterior portal. (A) The suture loop has been cinched around the biceps tendon (BT), and an arthroscopic tissue penetrator is being passed through the BT just distal to the looped suture. (B) The suture has been looped around the BT, and it is tacked in place just distal to the loop. (C) The BT has been secured with a suture anchor at the most distally visualized portion of the intra-articular bicipital groove. The cut end of the BT is marked with an asterisk. The cut end of the BT is seen distally translated from its original insertion at the superior labrum (chevron). G, glenoid; H, humerus.
Measurement of Post-tenodesis Tendon Motion
The fiducials were removed from the proximal tendon and reapplied based on the new tendon position. They were applied in the same configuration as used in the native state; the fiducials on the bicipital groove did not need to be changed, as they remained in their baseline position. The data collection for the tenodesis condition followed the protocol used for the native state.
Statistical Analysis
Seven individual paired t tests (Minitab) were performed, 1 for each motion, to determine whether maximum biceps tendon translation in the bicipital groove was a function of tendon condition (native vs post-tenodesis). Differences were deemed significant if P < .05.
Results
Results of tendon motion for the native and tenodesed tendons are shown in Table 1. The highest standard deviation in achievable range of motion, 24.6°, was in shoulder flexion-extension.
Tendon Range of Motion for the Native and Post-tenodesis Conditions a

a Data are reported as mean ± SD. Boldface P values indicate statistically significant differences between conditions (P < .05).
There was minimal motion of the biceps tendon during elbow flexion and extension in the native state, regardless of forearm position. The native-state tendon motion ranged from 1.73 ± 1.43 mm to 3.03 ± 1.55 mm, with the largest amount of motion occurring with the forearm fully pronated (Table 1, Figure 6). Larger motion of the biceps tendon occurred during glenohumeral motion in the native state, during all planes of scapular motion. The tendon motion ranged from 5.14 ± 2.67 mm to 20.73 ± 8.21 mm, with the largest amount of motion occurring during shoulder flexion and extension (Table 1, Figure 6).
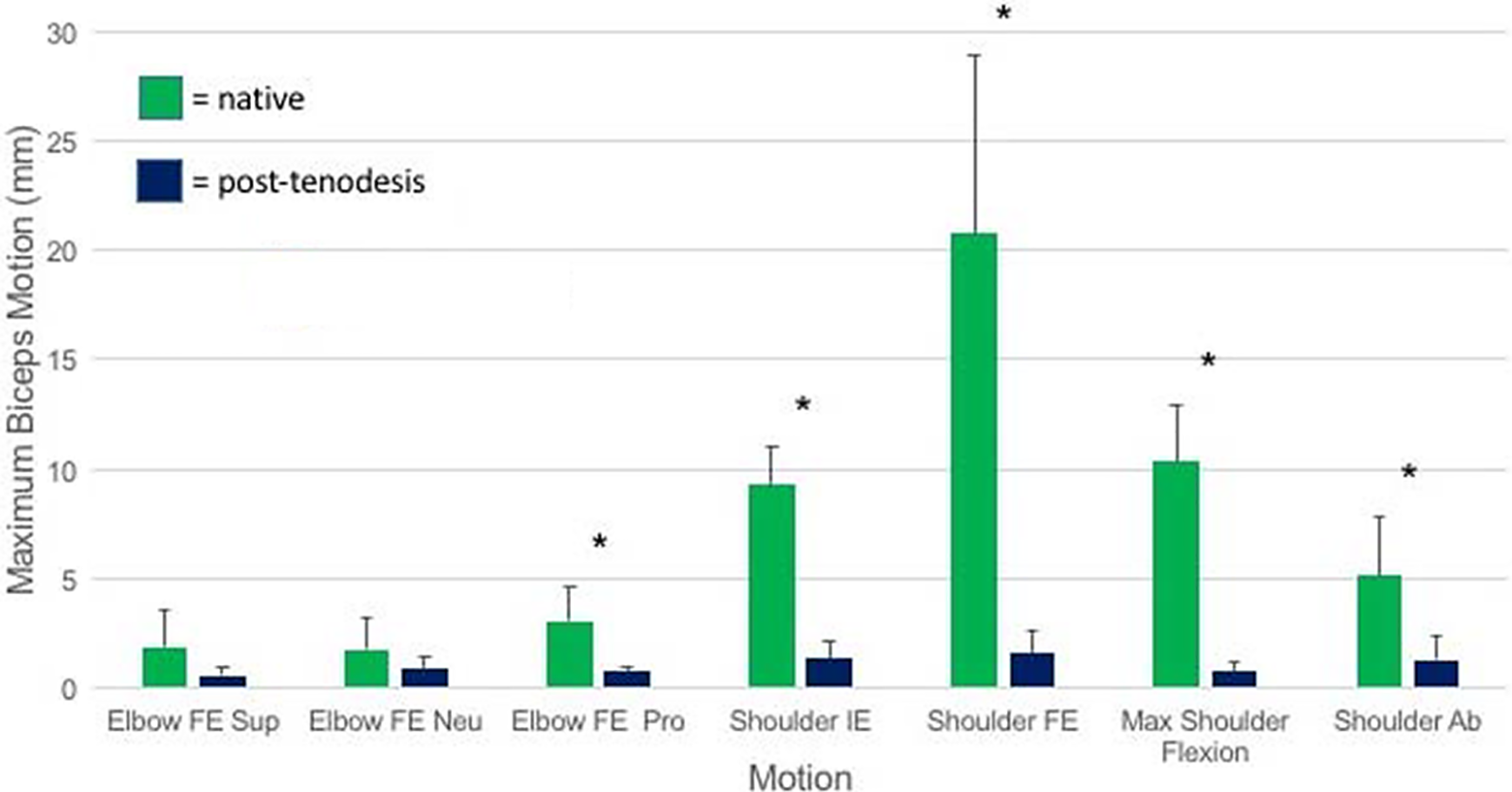
The mean tendon motion for each motion tested under both the native and post-tenodesis conditions. The SD is represented by the bars, and differences that achieved statistical significance are marked with an asterisk. Ab, abduction; FE, flexion-extension; IE, internal-external rotation; Neu, neutral forearm; Pro, pronated forearm; Sup, supinated forearm.
The motion of the biceps tendon after tenodesis was reduced in every plane of motion compared with the native state, with a range in tendon motion from 0.56 ± 0.37 mm to 1.57 ± 0.98 mm with either elbow or shoulder range of motion. A statistically significant reduction in tendon motion was achieved during elbow flexion in full forearm pronation. The reduction in tendon motion during elbow flexion in the neutral position and in full supination did not achieve statistical significance (Table 1, Figure 6). There was a significant decrease in biceps motion with shoulder motion in all planes (Table 1, Figure 6). The largest amount of motion in any plane after the tenodesis was 1.57 ± 0.98 mm during shoulder flexion and extension, significantly reduced from the native state of 20.73 ± 8.21 mm (P < .01) (Figure 7).
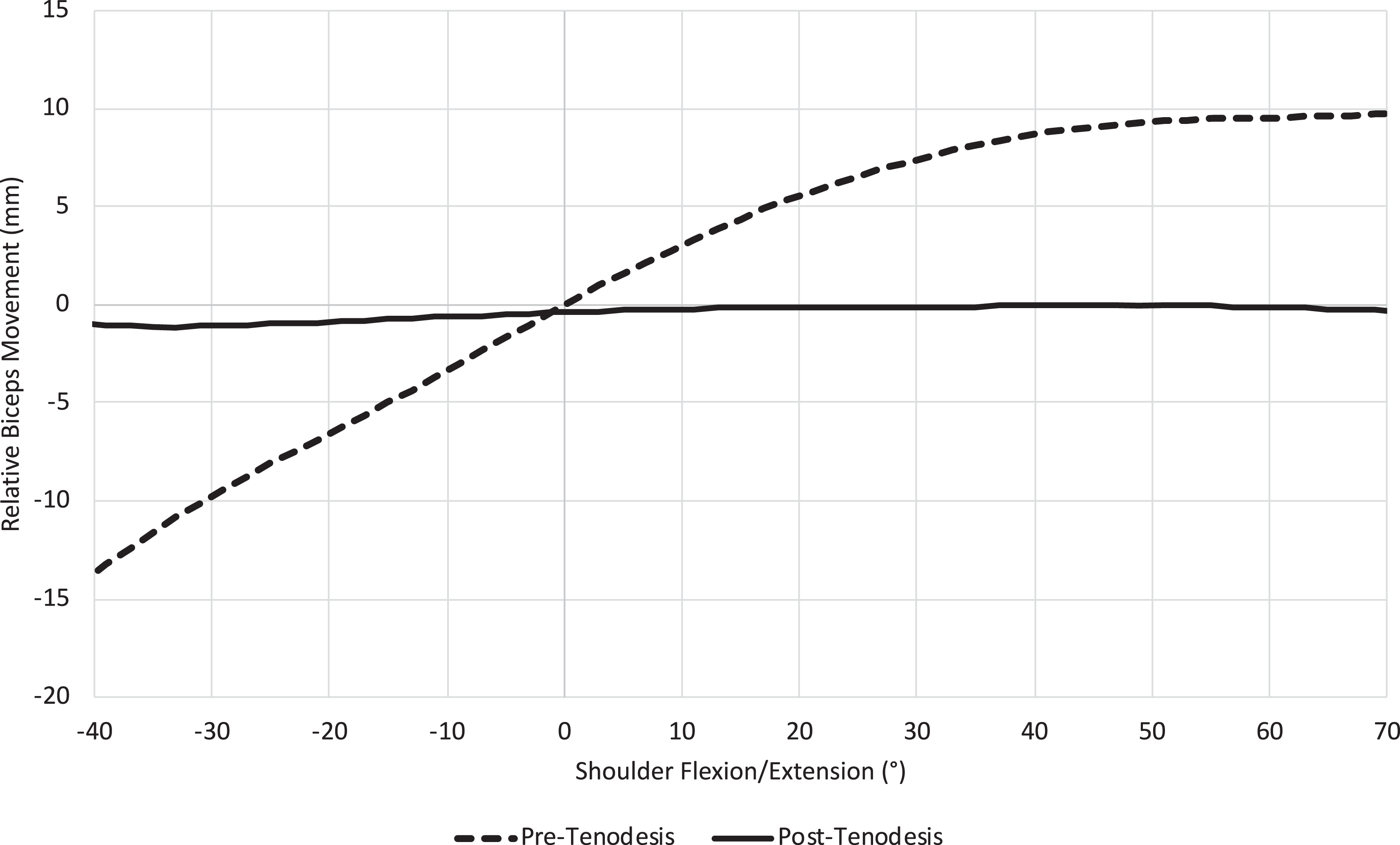
A graphical representation of tendon motion as a function of shoulder flexion and extension in the native (preoperative) and post-tenodesis conditions. Zero is the baseline tendon position. This plane of motion exhibited the largest amount of motion under both conditions.
Discussion
The present study demonstrated that for a particular technique of intra-articular, suprapectoral fixation (loop ‘n’ tack), post-tenodesis movement of the tendon within the groove was minimal and significantly less than that of a native shoulder. Although no studies have established a relationship between motion within the groove and tenosynovitis, it is logical that movement of the tendon within the groove would likely be more symptomatic than a static placement of the tendon or having it out of the groove altogether. Clinical studies are warranted to evaluate the incidence of groove pain after use of this technique and also to compare it with other tenodesis methods.
There has been significant debate as to the optimal site of the tenodesis. Proponents of subpectoral (or “out-of-the-groove”) tenodesis techniques stress the presence of groove pathology (ie, tenosynovitis, tearing of the biceps within the groove, and osteophytes within the groove) as a potential source of continued pain with proximal “above-the-groove” tenodesis techniques. 17 Theoretically, some of these potential pathophysiologic conditions would be mitigated by a technique that limited motion within the groove. Given the biomechanical accomplishment of this based on the present study, clinical studies are needed to evaluate the validity of that postulation.
Prior biomechanical and clinical studies of biceps tenodesis techniques have found generally favorable outcomes for multiple techniques. Biomechanical analyses of different constructs have found similar loads to failure for multiple different types of intra-articular techniques compared with a traditional subpectoral technique. 12,13 Complications from subpectoral tenodesis, however, may be greater because of the risk for humeral fracture. 8 No biomechanical studies, however, have quantified movement of the tendon within the bicipital groove for any arthroscopic technique.
In terms of clinical results, equivalent outcomes have been found when comparing all arthroscopic techniques with a traditional subpectoral technique. This previous comparison by Kahlenberg et al 13 used an arthroscopic technique that differed from the present study in that the tendon was tenodesed outside of the groove. Again, further research into this for the technique presented in this study is needed.
Limitations
There are some limitations to the current study. One, our biomechanical model did not account for or re-create muscle activation of all the periscapular and arm muscles; however, it is worth noting that muscles were not activated during the preoperative evaluation of shoulder and elbow motion, and significant motion occurred during passive range of motion. The drastic reduction (20.7 mm before tenodesis vs 1.5 mm after) in motion post-tenodesis indicates that the loop ‘n’ tack tenodesis technique will clinically contribute to reduce motion within the groove. Two, as part of our experimental setup, the tenodesis was performed open, whereas the technique is meant to be performed arthroscopically. We minimized variations from the arthroscopic technique by using identical anchors, technique, and instruments as would have been used arthroscopically. Three, the experimental setup necessitated an osteotomy of the tip of the coracoid to fully visualize the biceps tendon throughout the full range of motion. We believe this had minimal effect, however, as we reattached the short head of the biceps tendon to the remaining coracoid.
Conclusion
The loop ‘n’ tack tenodesis technique resulted in a statistically significant reduction in motion of the biceps tendon in all planes of scapular motion, with a maximum motion of 1.57 mm compared with 20.73 mm in the native shoulder before tenodesis. Future clinical studies should evaluate the correlation between biceps tendon motion within the groove and clinical symptoms.
Footnotes
Notes
Final revision submitted July 1, 2020; accepted August 6, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: The anchors used for tenodesis in this study were donated by Arthrex. B.J.K. has received research support from Arthrex; educational support from Mid-Atlantic Surgical Systems and Smith & Nephew; and hospitality payments from Biomet and Exactech. S.A. has received research support, consulting fees, and speaking fees from Arthrex and educational support from Mid-Atlantic Surgical Systems. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.