
Abstract
Background:
Controversy exits regarding performing a tenotomy versus a tenodesis of the long head of the biceps tendon (LHBT).
Purpose:
To evaluate the complications after arthroscopic tenotomy of the LHBT and characterize the incidence of cosmetic deformity, cramping, subjective weakness, and continued anterior shoulder pain (ASP). Additionally, to identify patient-related factors that may predispose a patient to these complications.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Records of patients who underwent an arthroscopic LHBT tenotomy at an integrated health care system under the care of 55 surgeons were retrospectively reviewed. Exclusion criteria included LHBT tenodesis, arthroplasty, neoplastic, or fracture surgery; age younger than 18 years; incomplete documentation of physical examination; or incomplete operative reports. Characteristic data, concomitant procedures, LHBT morphology, and postoperative complications were recorded. Patients with and without postoperative complications—including cosmetic deformity, subjective weakness, continued ASP, and cramping—were analyzed by age, sex, dominant arm, body mass index (BMI), smoking status, workers’ compensation status, and intraoperative LHBT morphology to identify risk factors for developing these postoperative complications.
Results:
A total of 192 patients who underwent LHBT tenotomy were included in the final analysis. Tenotomy was performed with concomitant shoulder procedures in all but 1 individual. The mean ± SD patient age was 60.6 ± 9.5 years, and 55% were male. The overall complication rate was 37%. The most common postoperative complications include cosmetic (Popeye) deformity (14.1%), subjective weakness (10.4%), cramping (10.4%), and continued postoperative ASP over the bicipital groove (7.8%). Every 10-year increase in age was associated with 0.52 (95% CI, 0.28-0.94) times the odds of continued ASP and 0.59 (95% CI, 0.36-0.98) times the odds of cramping pain. Male patients had 3.9 (95% CI, 1.4-10.8) times the odds of cosmetic (Popeye) deformity. Patients who had active workers’ compensation claims had 12.5 (95% CI, 2.4-63.4) times the odds of having continued postoperative ASP. Tenotomy on the dominant arm, BMI, and active smoking status demonstrated no statistically significant association with postoperative complications.
Conclusion:
Patients experiencing complications after tenotomy were significantly younger and more likely to be male and to have a workers’ compensation injury. LHBT tenotomy may best be indicated for elderly patients, female patients, and those without active workers’ compensation claims.
The long head of the biceps tendon (LHBT) is a common source of shoulder pain and can result in significant morbidity. Pathology of the LHBT can be due to primary isolated tendinopathy owing to inflammatory, degenerative, and traumatic causes; however, it is more frequently associated with other shoulder pathology, such as impingement, rotator cuff disorders, and glenohumeral arthritis. Clinically, patients often present with anterior shoulder pain (ASP) and loss of forward flexion. 13,15
Patients with symptoms refractory to nonoperative management may benefit from arthroscopic biceps tenotomy or tenodesis. Favorable outcomes have been reported for both procedures, and no clinical studies have definitively demonstrated the superiority of either arthroscopic technique. 2,5 –8,14 Advocates of biceps tenodesis cite its ability to better maintain length and tension of the proximal LHBT, thereby potentially preserving elbow flexion and supination strength and decreasing the risk of cosmetic deformity or cramping pain. 2,3,9,10,14
Compared with LHBT tenodesis, arthroscopic tenotomy is a less technically demanding surgery, decreases operative time, and requires little postoperative rehabilitation, allowing patients to return to full activity sooner. 5 However, complications associated with tenotomy of the LHBT include cosmetic deformity (Popeye deformity), muscle cramping, continued ASP, and weakness in forearm supination and elbow flexion. 2,5,7,9,11,12,15 Prior studies 2,4,7,9,11,12,15 have assessed complications and outcomes associated with LHBT tenotomy, but these studies have been limited in sample size and length of follow-up and have been largely single-institution studies.
The purpose of this study was to review a large series of LHBT tenotomy cases and characterize the incidence of complications such as cosmetic deformity, cramping, subjective weakness, and continued ASP. Furthermore, we sought to compare patients with and without these postoperative complications and identify patient-related factors that may predispose an individual to develop them. We hypothesized that certain patient-related characteristics would be associated with increased risk of developing postoperative complications.
Methods
Institutional review board approval was obtained before initiation of the study. LHBT tenotomies performed between January 1, 2006, and December 31, 2014, by 55 surgeons from 14 hospitals in a multispecialty integrated healthcare system were identified and retrospectively reviewed. All patients undergoing an arthroscopic shoulder procedure where the LHBT was surgically released were identified. Biceps tenodesis, conversion of tenodesis to tenotomy, spontaneous ruptures of the LHBT, arthroplasty, tenotomy in the setting of neoplastic or fracture surgery, age younger than 18 years, and patients with incomplete documentation of the pre- and postoperative physical examinations or operative report were excluded. During the study period, 1795 patients underwent arthroscopic shoulder surgery involving an LHBT procedure; 1526 patients who had a tenodesis and 77 patients with incomplete data were excluded, resulting in 192 patients undergoing tenotomy available for analysis. The tenotomy was generally performed as a component of multiple procedures during arthroscopic shoulder surgery; therefore, patients were not excluded for concomitant shoulder procedures.
Data were collected via an integrated electronic medical record chart review of patient characteristics, including age, sex, body mass index (BMI), smoking status, workers’ compensation status, arm dominance, side of procedure, date of procedure, and date of most recent follow-up. Concomitant procedures performed at the time of tenotomy were recorded, including rotator cuff repair, labral repair, glenohumeral debridement, subacromial decompression, distal clavicle resection, and subscapularis repair. In addition, the operative reports and, when available, intraoperative arthroscopic photos were reviewed to classify the morphology of the LHBT as normal, mild hypertrophy, or severe hypertrophy before tenotomy. Classification was performed by the senior author (R.M.).
Pre- and postoperative ASP over the bicipital groove, biceps cosmetic (Popeye) deformity, cramping, and subjective weakness were recorded. ASP was defined as patients with bicipital groove pain to palpation or with Yergason testing. We defined “persistent” ASP as residual (continued) ASP that did not resolve after surgery, indicating that the procedure failed to alleviate ASP. All postoperative clinical documentation was reviewed for additional complications, including nerve injury, superficial and deep infection, revision biceps procedure, hospitalization, pulmonary embolism, and deep vein thrombosis.
Patients with and without postoperative complications, including cosmetic deformity, subjective weakness, continued ASP, and cramping, were analyzed by age, sex, dominant arm, BMI, smoking status, workers’ compensation status, and intraoperative LHBT morphology to identify risk factors for developing these postoperative complications.
Statistical Analysis
Patient age and BMI were treated as continuous variables, and sex, arm dominance, smoking status, workers’ compensation status, and intraoperative LHBT morphology (normal or mild hypertrophy vs severe hypertrophy) were dichotomized. The association between categorical patient-related factors and postoperative complications was assessed with the chi-square or Fisher exact test, as appropriate. For significant associations of interest, crude odds ratios and Wald 95% CIs were calculated. Medians of continuous variables were compared with the Kruskal-Wallis test. All P values were 2-sided with an alpha of 0.05. Statistical analyses were performed using SAS Version 9.3 (SAS Institute).
Results
Characteristics
A total of 192 patients who underwent arthroscopic LHBT tenotomy were included in the final analysis. Characteristic data are presented in Table 1.
Characteristic Data (N = 192)

Tenotomy was performed with concomitant shoulder procedures in all but 1 individual. The frequency of concomitant shoulder procedures is presented in Table 2.
Operative Data

Complications
The overall complication rate was 37%. The most common postoperative complications were cosmetic (Popeye) deformity (14.1%), subjective weakness (10.4%), cramping (10.4%), and continued postoperative ASP (7.8%). Seven (3.6%) patients underwent revision surgery to convert the LHBT tenotomy to a tenodesis, 6 of 7 (86%) being for postoperative cosmetic deformity. The frequency of all postoperative complications is presented in Figure 1.

Postoperative complications after long head of the biceps tendon arthroscopic tenotomy. ASP, anterior shoulder pain.
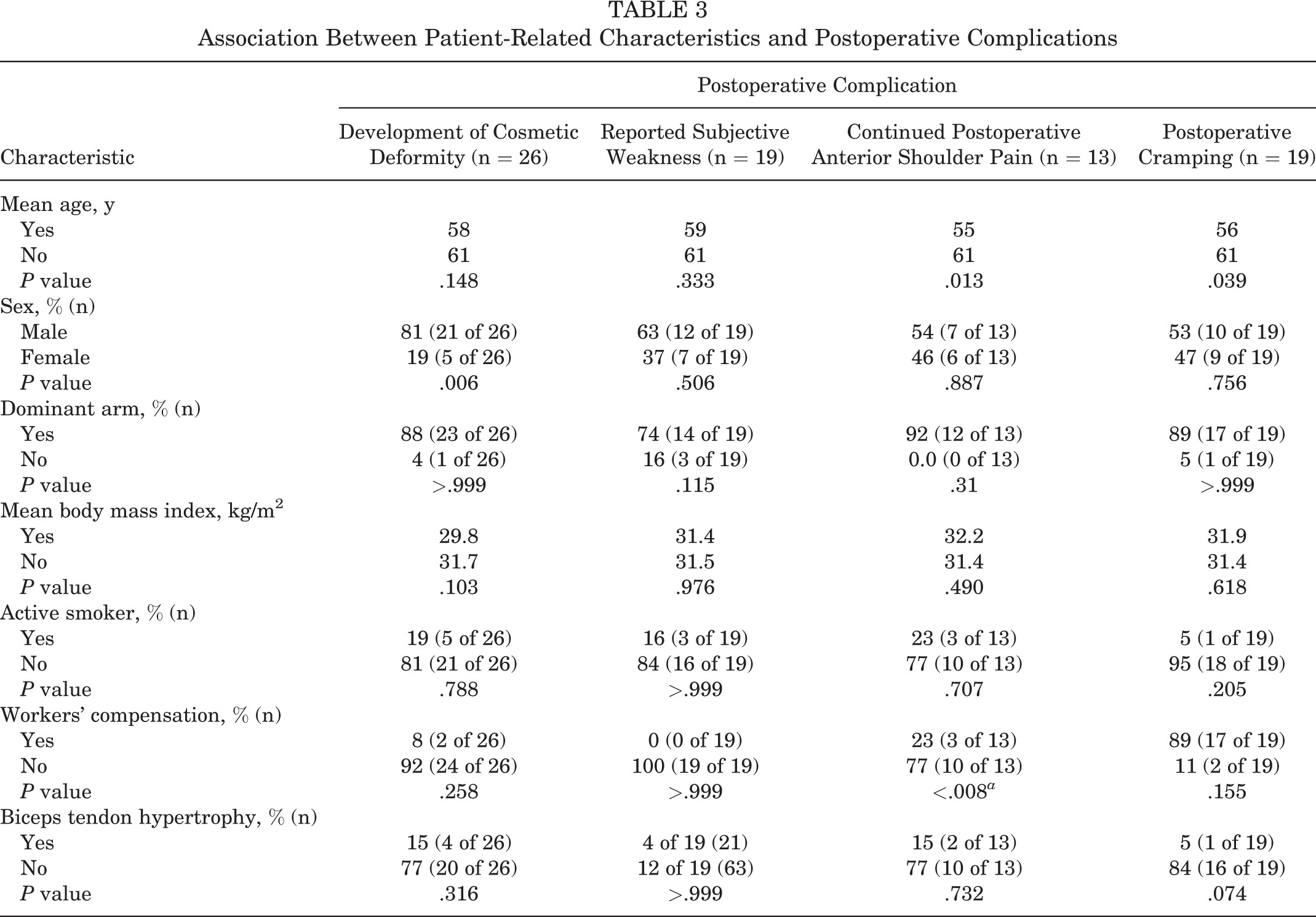
Every 10-year increase in age was associated with 0.52 (95% CI, 0.28-0.94) times the odds of continued ASP and 0.59 (95% CI, 0.36-0.98) times the odds of cramping pain. Male patients had 3.9 (95% CI, 1.4-10.8) times the odds of cosmetic (Popeye) deformity. Patients who had active workers’ compensation claims had 12.5 (95% CI, 2.4-63.4) times the odds of having continued postoperative ASP. Subjective weakness was seen among 9.3% of those with tenotomy on the dominant arm and 25.0% of those with tenotomy on the nondominant arm (P = .115). Cramping was seen among 2.4% of those with hypertrophy and among 12.6% of those with no or mild hypertrophy (P = .074) (Table 3).
Association Between Patient-Related Characteristics and Postoperative Complications
Discussion
This is the largest series of LHBT tenotomy cases in the literature assessing postoperative complications, and the results of this study suggest that male sex, young age, and workers’ compensation status are associated with increased complications following tenotomy. These results may help guide surgeons to choose an alternative procedure in patients with risk factors.
LHBT tenotomy has been reported to provide reliable pain relief and is a relatively simple procedure that requires little postoperative rehabilitation 2,5,7,16 ; however, clear indications for the procedure have yet to be determined, and tenotomy has been associated with clinically relevant postoperative complications. Cosmetic (Popeye) deformity was the most frequent postoperative complication noted in our study, at 14.1%. This incidence is within the range reported in the literature (3%-70%). 7,9 Given the retrospective nature of our study, surgeons did not actively screen for cosmetic deformity postoperatively; thus, the 14.1% reported in our study likely excludes deformities that are of such little clinical significance to not be noted by the patient. The only patient-related factor associated with developing a cosmetic deformity was male sex. Other studies 9 –11 have demonstrated similar associations between male sex and cosmetic deformity. While prior studies 12,15 have speculated that cosmetic deformity may be less detectable in patients with higher BMI, tenotomy on the nondominant arm, or older patients, owing to age-related muscle atrophy or tone, the present study, as well as the study by Lim et al, 11 did not demonstrate an association between these patient-related factors and cosmetic deformity after LHBT tenotomy.
Aside from male sex, younger age and active workers’ compensation claims demonstrated a significant association with certain postoperative complications. Continued postoperative ASP has been reported to occur in up to 46% of patients after LHBT tenotomy, a higher frequency than observed in the current study (10.4%). 2 Patients with active workers’ compensation claims were more likely to continue to have ASP. A prior study 8 has recommended against LHBT tenotomy in patients pursuing workers’ compensation, but this is the first study, to our knowledge, to identify a specific complication after tenotomy associated with active workers’ compensation claims.
The association between younger age and postoperative complications after LHBT tenotomy remains controversial. In the current study, older age was associated with decreasing odds of postoperative ASP. This is consistent with the results by Kelly et al, 9 who demonstrated a higher incidence of complications such as cosmetic deformity or weakness in younger patients. However, Duff and Campbell 4 demonstrated no difference among cramping, weakness, or deformity based on age (59 vs 66 years).
Finally, biceps tendon hypertrophy demonstrated a decreased association with developing postoperative cramping, but the study was underpowered to detect a significant difference. Ahmad et al 1 previously demonstrated that diseased tendons with greater presumed hypertrophy and flattening require more force to travel through the bicipital groove and thereby are more likely to undergo autotenodesis within the bicipital groove. The autotenodesis, more likely to occur in hypertrophic tendons, may in part explain the decreased association with postoperative cramping. However, a protective effect was not seen with respect to other complications assessed. A possible reason for the lack of a difference in complications between hypertrophic LHBTs and LHBTs with minimal or no hypertrophy is that in the latter group the diseased part of the tendon may be extra-articular and therefore not visualized during simple arthroscopic tenotomy.
Several prior studies 2,7,9,12,15 have reported on the complications after arthroscopic tenotomy of the LHBT; however, the majority of these studies have been from single-center, single-surgeon experiences or are of small sample size. Only 2 prior studies examined associations between patient-related factors and postoperative complications after LHBT tenotomy. Duff and Campbell 4 assessed patient acceptance after LHBT tenotomy in 117 cases—specifically, for the presence of cosmetic deformity (27%), muscle weakness (31%), and biceps cramping (19%), all of which occurred with higher frequency than noted in our study. The only subgroup analysis performed was that between a “manually active” group and a “sedentary” group, and no differences across the 3 complications were noted. Lim et al 11 published the largest series examining complications after LHBT tenotomy in 132 patients; however, it was also a single-center, single-surgeon experience. The authors assessed for the presence of postoperative cosmetic deformity, cramping, and elbow flexion weakness. Subanalysis was completed comparing age, sex, arm dominance, and BMI. Lim et al 11 demonstrated a higher incidence of cosmetic deformity (45%) and a similar incidence of biceps cramping (8%) relative to the current study. As stated previously, only male sex was associated with cosmetic deformity; BMI and hand dominance had no association with the assessed complications, in agreement with the current study.
The findings of our study largely support the existing literature regarding postoperative complications after arthroscopic LHBT tenotomy, particularly with male sex being associated with cosmetic deformity. Additionally, we demonstrated that younger patients and those with workers’ compensation claims may be at increased risk for postoperative complications. This study differs from prior studies in that it was conducted using an integrated health system electronic medical record that analyzed complications across 14 hospitals and 55 surgeons. We also evaluated a range of complications and tested for an association with multiple patient-related factors. Additionally, the heterogeneity of the surgeons and patients in the current study increases the generalizability of our results and addresses some of the limitations of prior studies 4,11 focused on only a single surgeon’s outcomes. Last, given that our patient population was within an integrated health care system, we have the ability to capture primary care and emergency room visits as well, thus minimizing the risk of missing postoperative complications.
Although there are several strengths to our study, the findings must be interpreted within the limitations of our study design. First, this was a retrospective study, so physicians were not instructed to assess for the analyzed postoperative complications, thereby likely resulting in underreporting of the overall complication rate. Furthermore, the retrospective nature of this study lends it to selection bias. Second, the retrospective nature of the study limited us from controlling the indications for LHBT tenotomy (vs tenodesis). Third, all but 1 patient had a concomitant procedure, and this may be a confounding factor for developing a postoperative complication, particularly ASP. Fourth, only 13 to 26 patients sustained a given complication, therefore lending the study liable to type 2 error and limiting subgroup analysis. Fifth, mean follow-up was only 11 months. Last, we did not have objective outcome scores or strength measurements; therefore, many of our complications were subjective, thus limiting some of the reproducibility of this study.
Multiple studies 2,4,7,9,15 have reported high satisfaction rates after LHBT tenotomy, and surgeons may prefer tenotomy over tenodesis, as it is technically less demanding and allows quicker postoperative rehabilitation. However, the indications for tenotomy versus tenodesis remain unclear. The results of this study suggest that male sex, young age, and workers’ compensation have an increased association with postoperative complications. Tenotomy may best be indicated for elderly patients, female patients, and those without active workers’ compensation claims. The results of this study should be used to counsel patients and engage in informed decision making regarding surgical options and potential risk for postoperative complications after LHBT tenotomy.
Footnotes
Final revision submitted September 3, 2019; accepted September 10, 2019.
One or more of the authors declared the following potential conflict of interest or source of funding: R.M. has received research support from Arthrex and the Joint Restoration Foundation; grant support from DJO; educational support from Arthrex; royalties from Zimmer Biomet, Thieme, and Wolters Kluwer; and honoraria from Arthrex. C.M. has received grant support from Arthrex and educational support from Smith & Nephew and Pylant Medical. R.K.A. has received research support from Accumed, Trimmed, and Arthrex and has stock/stock options in Zimmer Biomet, Stryker, Medtronic, and Axogen. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kaiser Permanente Southern California Institutional Review Board.