
Abstract
Background:
No study has investigated the treatment outcomes of isolated subscapularis tears with advanced fatty infiltration and tear progression to the supraspinatus tendon.
Purpose:
To assess the natural progression of isolated subscapularis tears with advanced fatty infiltration and compare clinical outcomes between nonoperative and operative treatment.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study included 52 patients who received either operative (group A) or nonoperative (group B) treatment at our institution for isolated subscapularis full-thickness tears with grade 3 or 4 advanced fatty infiltration. All study patients had a minimum 2-year follow-up. The following 4 functional measures were used: visual analog scale for pain, Subjective Shoulder Value, American Shoulder and Elbow Surgeons score, and University of California Los Angeles score. The modified belly-press test was used to assess subscapularis muscle strength. In group A, structural integrity was evaluated using magnetic resonance imaging at 6 months after surgery. In addition, ultrasonographic evaluation was performed on both groups during the follow-up period to assess tear progression into the supraspinatus tendon.
Results:
At initial presentation, all functional assessment scores were significantly worse in group A versus group B (P ≤ .05 for all 4 scores). When we compared the mean change in scores before treatment versus after treatment, the group A patients were found to have significantly greater improvement than group B patients (P < .001 for all 4 scores); however, no significant difference was seen in final outcome scores between the groups. Although a high retear rate of 78.6% (22/28) was identified in group A, both groups showed no further tear progression to the supraspinatus tendon at the final ultrasonographic evaluation.
Conclusion:
For isolated subscapularis tears with advanced fatty infiltration, clinical improvement was seen with both nonoperative and operative treatment. Although the operatively treated group started with lower baseline scores, there were no significant differences in outcomes at final follow-up. Considering the high retear rate even after repair, surgical treatment of these lesions may not be warranted. Early detection and prompt repair of subscapularis tears, before the lesion becomes advanced with grade 3 or 4 fatty infiltration, are important for better outcomes.
Subscapularis tears combined with other rotator cuff tears are relatively common, with a reported incidence ranging from 19% to 49%. 12,23,24 However, an isolated tear of the subscapularis tendon is rarely found and has an incidence of 5% or less. 2,9,24,27 Because of inherent anatomic differences between the subscapularis tendon and the posterosuperior cuff tendons, isolated subscapularis tears do not present typical rotator cuff symptoms. Their primary symptom is weakness during internal rotation, rather than during forward flexion, of an affected arm; anterior shoulder pain; and symptoms related to the long head of the biceps tendon with its pulley lesions. 1,6 Other characteristics include little or no retraction even with full-thickness tear in many cases because the tendon is attached to the transverse ligament over the bicipital groove. 21,34 This characteristic may delay the diagnosis until the neglected tear becomes more advanced and accrues severe retraction over time.
The subscapularis tendon forms an important axis in the transverse force couple of the shoulder, and its muscle represents a large proportion of the rotator cuff and plays a significant role in the overall function of the shoulder. 4,29,32,33 Burkhart 5 emphasized the importance of the transverse force couple early on, and many ensuing authors reported satisfactory outcomes after achieving acceptable force coupling reconstruction even with massive rotator cuff tears, when complete repair was not feasible. 7,11,15,30,31
In contrast, despite a broken force couple by advanced isolated subscapularis tear, many patients maintain relatively good overall shoulder function with tolerable levels of pain. However, few studies are available on the prognoses and outcomes after nonoperative or operative treatment of advanced isolated subscapularis tears. Additionally, no study has investigated the tear progression to the supraspinatus tendon in advanced isolated subscapularis tears. Therefore, this study aimed to assess the natural progression of isolated subscapularis tears with advanced fatty infiltration and to compare clinical outcomes between nonoperative and operative treatment groups. We hypothesized that (1) despite clinical improvement after repairs, there would be no significant differences between the 2 groups at final follow-up, and (2) the nonoperative treatment group would experience tear progression into the supraspinatus tendon during the study period.
Methods
Study Population
We retrospectively reviewed the data of 69 patients to be included in this study. These patients received operative or nonoperative treatment for isolated subscapularis full-thickness tear with Goutallier grade 3 or 4 advanced fatty infiltration at our institution. 14 The study period was between March 2009 and February 2018. The indications for repair were pain and disability refractory to nonoperative treatment and a tear that was considered reparable. We defined the tendon as reparable when the retraction of the torn tendon resided lateral to the glenoid on the axial image of magnetic resonance imaging (MRI). The patients who underwent arthroscopic repair were assigned to group A (Figure 1). Patients with irreparable tears (torn tendons retracted further medial to the glenoid) were treated with nonoperative treatment and assigned to group B (Figure 2). Exclusion criteria were (1) lack of minimum 2-year follow-up or ultrasonographic rotator cuff evaluations (15 patients); (2) severely retracted subscapularis tendon tear wherein reattaching the upper tendinous portion of the torn tendon was not feasible and partial repair of lower portion was possible (3 patients); (3) surgical history on the affected shoulder (1 patient); and (4) workers’ compensation claims (2 patients). Our institutional review board approved this study and waived the requirement for informed consent.
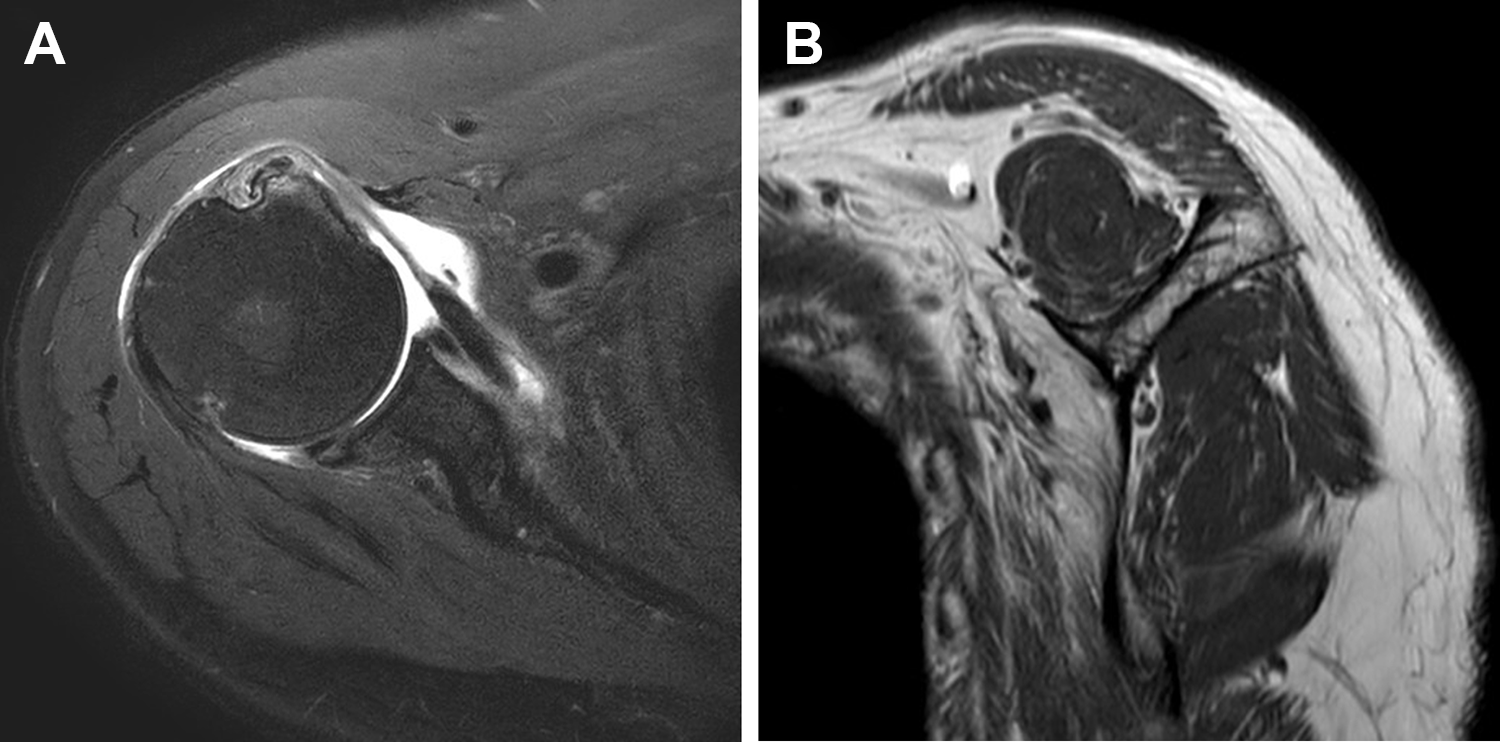
(A) The torn subscapularis tendon located within the lateral side of the glenoid. (B) Grade 3 fatty infiltration of the subscapularis muscle. These tears were considered reparable.

(A) The torn subscapularis tendon retracted more medial to the glenoid. (B) Grade 4 fatty infiltration of the subscapularis muscle. These tears were considered irreparable.
Overall, 52 patients (28 patients in group A and 24 patients in group B) were included in this study. Nonoperative treatment encompassed rehabilitation exercises and pain management. Rehabilitation exercises included stretching and passive range of motion (ROM) exercises to preserve supple ROM of the affected shoulder. Internal and external rotation strengthening exercises were also performed using an elastic bandage. Pain management consisted of intermittent intra-articular corticosteroid injection, anti-inflammatory medication, and narcotic skin patches. Regular examination was performed every 3 to 6 months during the study period.
Surgical Procedure
Arthroscopic repair was performed with the patient under general anesthesia in the beach-chair position. Standard posterior, anterior, and superior portals were created. After biceps tenotomy, the upper tendinous portion of the subscapularis tendon, which was medially retracted, was identified. A traction suture was then placed in the thickened biceps medial sling. The rotator interval was opened, and the adhesion around the coracoid was released. Viewed from the lateral portal with a 70° scope, the soft tissue on the bursal side of the subscapularis tendon and footprint (lesser tuberosity) was prepared. After we examined the mobility of the tendon, the suture anchors were inserted through the anterior portal. The sutures were passed in a row using a suture passer via the anterolateral working portal. The knots were then secured in single-row fashion. All surgically treated patients had biceps tendon subluxation/dislocation or degenerative tears. With the exception of those patients with spontaneous ruptures, we performed either a biceps tenotomy or tenodesis in all patients.
Postoperative Rehabilitation
The affected arm was maintained with a sling in internal rotation for 6 weeks without any exercise. Then, self-assisted passive ROM, including forward flexion in the supine position, and table sling stretching exercises were initiated. Self-assisted active ROM exercises were encouraged after 8 weeks. Isotonic strengthening exercises using an elastic band began 3 months after surgery. Gradual return to the patients’ premorbid level of sports activities was allowed after 6 months.
Functional and Radiological Assessments
For functional evaluation, we used the visual analog scale (VAS) pain score (ranging from 0 to 10), Subjective Shoulder Value (SSV; patient’s estimate of the value of the affected shoulder as a percentage of the normal shoulder), American Shoulder and Elbow Surgeons (ASES) shoulder score, and University of California Los Angeles (UCLA) shoulder score. The modified belly-press test was used to assess subscapularis muscle strength. 24
Active ROM was measured based on forward flexion in the scapular plane, external rotation with the elbow at the side, and internal rotation. Internal rotation was estimated by recording the highest spinal segment that a patient could reach with his or her thumb. For statistical analyses, the spinal segment level reached by the patient was converted to a number: T1 to T12 levels were represented by 1 through 12; L1 to L5 levels were indicated by 13 through 17; and the sacrum was designated by 18. 19,20,22,28 An independent examiner (H.-S.K.), who was blinded to the patient data, evaluated the functional values and active ROM.
Preoperative radiological evaluations included true anteroposterior, axial radiography, and shoulder MRI or magnetic resonance arthrography (MRA). Postoperative MRA or computed tomographic arthrography (CTA) was performed 6 months after surgery for group A. During a regular follow-up, ultrasonography was performed on patients in both groups to assess tear progression to the supraspinatus tendon.
Statistical Analysis
Statistical analyses were performed using SPSS software (Version 25; IBM Corp). The Wilcoxon signed-rank test was used to compare the initial and final follow-up values within each group. The Mann-Whitney U test was used to compare continuous or continuous ranked values between the groups. The Fisher exact test was used for categorical values. Significance was set at P < .05. Sample size was calculated taking the ASES score as the primary variable, and the calculation was performed in accordance with previously published results on the minimal clinically important difference in ASES score. 10 With an effect size of 17, a confidence level of 95% (α = .05), and a power of 90%, a power calculation indicated the need for a minimum of 22 patients per group.
Results
Patient Demographic Characteristics
Patient demographic characteristics are shown in Table 1. No statistically significant differences were noted in demographic characteristics between the 2 groups, however there was a significant difference in fatty infiltration grade (Table 1).
Patient Demographic Characteristics a

a Group A, arthroscopic repair; Group B, nonoperative treatment. Data are reported as mean ± SD (range) unless otherwise indicated. Bolded P value indicates statistically significant difference between groups.
Functional and Radiologic Assessments
At initial presentation, all functional outcomes (VAS pain, SSV, ASES, and UCLA scores) were significantly different between groups (P ≤ .05 for all), with group A having increased symptoms and worse function compared with group B (Table 2). All functional outcome scores improved from initial assessment to final follow-up in both groups. When evaluating the mean change in scores before treatment versus after treatment within each group, we noted a greater improvement in group A versus group B, which was statistically significant (P < .001 for all 4 scores). However, the between-group comparison of the final follow-up scores showed no statistical difference in outcomes (Table 2).
Comparison of Functional Outcome Scores Between Groups a
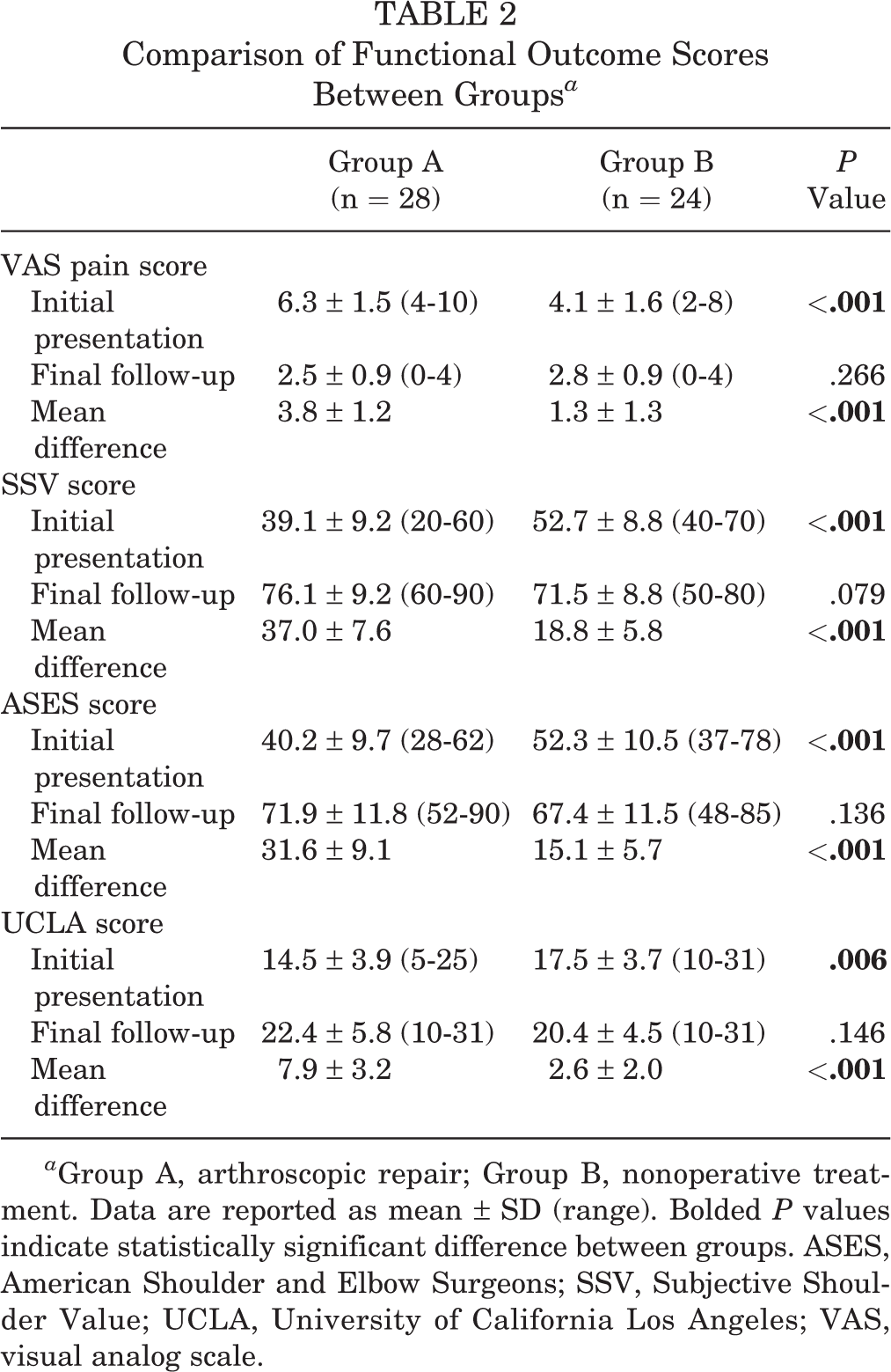
a Group A, arthroscopic repair; Group B, nonoperative treatment. Data are reported as mean ± SD (range). Bolded P values indicate statistically significant difference between groups. ASES, American Shoulder and Elbow Surgeons; SSV, Subjective Shoulder Value; UCLA, University of California Los Angeles; VAS, visual analog scale.
Regarding ROM at initial presentation, internal rotation was the only area in which there was a statistically significant difference between the groups (16.4° in group A vs 14.7° in group B; P = .001) (Table 3). At final follow-up, although patients in both groups saw significant improvement in mean forward flexion, external rotation, internal rotation, and modified belly-press test results (P < .05 for all), we found no statistically significant differences between the groups on any measure (Table 3).
Preoperative and Final Follow-up of the Active Ranges of Motion of Shoulders in Both Groups a

a Group A, arthroscopic repair; Group B, nonoperative treatment. Data are reported as mean ± SD (range). Bolded P values indicate statistically significant difference between groups.
b Measured by recording the highest spinal segment that the patients could reach with their thumb. This spinal segment level was then converted to a number: T1 through T12 are represented by 1 through 12; L1 through L5 are represented by 13 through 17; and the sacrum is represented by 18.
Among the 28 patients in group A, 22 (78.6%) showed retear on the follow-up MRA or CTA. No progression of fatty infiltration was observed on follow-up MRI scans. Final follow-up ultrasonography at regular checkup was performed at a mean of 53.6 ± 21.5 months for all patients (55.7 months for group A and 51.3 months for group B). Although 2 patients in group A were diagnosed with a persistent grade 2 (<6 mm) partial articular supraspinatus tendon avulsion lesion that was identified during the arthroscopic examination, the final ultrasonogram revealed no newly developed posterosuperior rotator cuff tears in either group.
Discussion
This study compared clinical outcomes and the integrity of the remaining rotator cuff between operative and nonoperative treatment for isolated subscapularis tears with advanced fatty infiltration. Both study groups showed substantial clinical improvements from initial to final follow-up; in particular, the operative treatment group had a statistically significantly greater improvement in clinical scores compared with the nonoperative treatment group. Nevertheless, a high retear rate (78.6%; 22/28) was identified in the operative treatment group on follow-up MRA/CTA, and no significant differences in clinical outcomes were seen between the groups at final follow-up. Moreover, follow-up ultrasonography revealed no tear progression to the supraspinatus tendon in either group, which did not support our hypothesis.
Many investigators have reported that a torn rotator cuff should be repaired before an advanced stage of damage is reached. If left untreated, an individual is likely to experience retear and suboptimal clinical outcomes, even after repair. 13,18,31 However, in our outpatient clinic, we sometimes encounter patients who tolerate rehabilitation well despite grade 4 fatty infiltration of the subscapularis muscle where little muscle remains and the transverse force couple is broken. We speculated whether repair of the subscapularis tendon in the advanced stage would be effective compared with nonoperative treatment, because a high retear rate had been expected, and whether the tear progressed to the supraspinatus tendon. The current study began from this question. As hypothesized, retear rates were considerably high. Nonetheless, although we noted significant improvement in clinical outcomes compared with preoperative values at final follow-up, there was no significant difference in clinical outcomes between operative and nonoperative treatment groups.
There are certainly beneficial effects of repairing isolated subscapularis tears even in advanced stages, and clinical improvement can be obtained after an operation. However, when discussing treatment options, the clinician should inform the patient that rates of retear are high, and the eventual outcome of repair may be similar to that of nonoperative treatment. When patients present with signs and symptoms of subscapularis dysfunction, it is considered essential to achieve early detection and perform a prompt repair, before the tear further progresses to grade 3 or 4 fatty infiltration. We find this practice interesting, because it is well known that the severity of symptoms does not necessarily correspond with the severity of disease. First, one of the causes of pain in the operative treatment group was the biceps lesion, which became degenerative and hypertrophic during either subluxation or dislocation medially from the bicipital groove, along with progression of the subscapularis tear. Second, it is supposed that patients in the nonoperative treatment group had adapted to their condition during progression of their subscapularis tears to the end stage. For the operative group, it is supposed that the remnant portion of the subscapularis tendon was partially present and the functions of other tendons were not coordinated, leading to imbalance among these tendons. On the contrary, patients in the nonoperative group, who had mostly advanced to the end stage of grade 4, had achieved some degree of stabilization and balance among the remaining cuff muscles through compensation.
Collin et al 8 published an interesting study regarding the relationship between pseudoparalysis and chronic rotator cuff tear with severe muscle degeneration. They found that the dysfunction of the supraspinatus with an entire subscapularis tear or combined tears of the supraspinatus, infraspinatus, and teres minor was highly related to pseudoparalysis. In the current study, despite the broken transverse force couple by an entire subscapularis tear with severe muscle degeneration, only 2 patients in the operative treatment group showed preoperative pseudoparalysis. These patients had an additional acute trauma history on existing chronic tears. Moreover, none of the patients in the nonoperative treatment group showed pseudoparalysis. Supposedly, the transverse force couple theory in isolated subscapularis tear may not be applicable in cases where the remaining cuff (supraspinatus, infraspinatus, and teres minor) is intact. In addition, despite broken transverse force couples, satisfactory outcomes in the current study may be attributed to intact function of the remaining rotator cuff tendons that preserves the coronal plane force couple between the cuff and deltoid muscle. As well, other muscles may function effectively as internal rotators of the arm.
We also investigated whether a subscapularis tear would extend to the supraspinatus. Regarding tear progression, several previous investigators have reported that typical rotator cuff tears beginning at or within the supraspinatus tendon propagate anteriorly or posteriorly. 16,17 Nové-Josserand et al 26 defined the anterosuperior rotator cuff tear and explained that the tear extends anteriorly to its border involving the subscapularis tendon. In case of subscapularis tear, it is well known that most subscapularis tendon tears begin at the articular side of the upper tendinous portion and, as with other rotator cuff tears, may progress in continuum from partial-thickness to full-thickness tear. 25 The tear may progress into the lower portion of the subscapularis tendon over time. However, no study has assessed whether isolated subscapularis tears in an advanced stage progress to the adjacent supraspinatus tendon. In the current study, at least during the study period, there was no progression to the supraspinatus tendon. We thus presume that the thickened medial biceps sling, which is observed in many chronic subscapularis tears, might provide a stress-shielding effect to prevent tear progression to the supraspinatus tendon, or the strong anterior rotator cable of the supraspinatus tendon might impede tear progression into the tendon. This occurs because of the pulling vector of the subscapularis tendon and the difference from the other components of the posterosuperior rotator cuff.
In the current study, the biceps tendon was always involved in the setting of advanced subscapularis full-thickness tear. Although the biceps tendon was ruptured spontaneously in some cases, many biceps tendons were subluxated or dislocated out of the bicipital groove as well as hypertrophied in the operative treatment group. As indicated by Boileau et al, 3 biceps tenotomy can improve symptoms in irreparable rotator cuff tears. Likewise, although there might be several factors affecting symptoms and pain level in advanced subscapularis tear, we believe that the spontaneous rupture of the biceps tendon can improve symptoms, and this may be associated with better preoperative pain level in the nonoperative treatment group as well as improved clinical outcomes in the operative treatment group, despite the high retear rate.
Several limitations need to be considered when interpreting the results of this study. Although we retrospectively compared outcomes between operative and nonoperative treatments, the initial values of the functional scores and fatty infiltration grades between the groups were different. The initial functional scores were worse in the operative treatment group than in the nonoperative treatment group, whereas the fatty infiltration grade was worse in the nonoperative treatment group. However, this study included only isolated subscapularis tears with grade 3 or 4 advanced fatty infiltration, and these advanced subscapularis tears were the basis of the study. Thus, this study provides some constructive understanding regarding clinical outcomes of lesions after operative and nonoperative treatment, as well as a chance to observe whether a given lesion further extends and involves other rotator cuff tendons. Additional limitations of the current study include the following: it was not a randomized study; no follow-up MRI evaluation was performed for the nonoperative treatment group; the pathology of the biceps tendons in relation to the subscapularis tears was not analyzed; and the modified belly-press test performed in this study was not sufficient to provide objective evaluation of internal rotation strength. Last, the lack of difference in outcome scores at the final follow-up may have resulted in a type II error owing to the low statistical power of a small sample size. However, the current study’s outcomes still provide some useful insights, because sample size calculation was performed through minimal clinically important difference before initiation of the study.
Conclusion
For isolated subscapularis tears with advanced fatty infiltration, clinical improvement was seen with both nonoperative treatment and surgical repair. Although the operatively treated group started with lower baseline scores, at final follow-up there was no significant difference in clinical outcomes between nonoperative and operative treatment. Considering the high retear rate even after repair, surgical treatment of these lesions may not be warranted. Early detection and prompt repair of the tears, before the lesion becomes advanced with grade 3 or 4 fatty infiltration, are considered imperative for better outcomes.
Footnotes
Final revision submitted July 17, 2020; accepted August 4, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Severance Hospital (study No. 4-2019-0533).