
Abstract
Background:
There is currently no optimal method for cartilage restoration in large, full-thickness cartilage defects in older patients.
Purpose:
To determine whether implantation of a composite of allogeneic umbilical cord blood–derived mesenchymal stem cells and 4% hyaluronate (UCB-MSC-HA) will result in reliable cartilage restoration in patients with large, full-thickness cartilage defects and whether any clinical improvements can be maintained up to 5 years postoperatively.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A randomized controlled phase 3 clinical trial was conducted for 48 weeks, and the participants then underwent extended 5-year observational follow-up. Enrolled were patients with large, full-thickness cartilage defects (International Cartilage Repair Society [ICRS] grade 4) in a single compartment of the knee joint, as confirmed by arthroscopy. The defect was treated either with UCB-MSC-HA implantation through mini-arthrotomy or with microfracture. The primary outcome was proportion of participants who improved by ≥1 grade on the ICRS Macroscopic Cartilage Repair Assessment (blinded evaluation) at 48-week arthroscopy. Secondary outcomes included histologic assessment; changes in pain visual analog scale (VAS) score, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and International Knee Documentation Committee (IKDC) score from baseline; and adverse events.
Results:
Among 114 randomized participants (mean age, 55.9 years; 67% female; body mass index, 26.2 kg/m2), 89 completed the phase 3 clinical trial and 73 were enrolled in the 5-year follow-up study. The mean defect size was 4.9 cm2 in the UCB-MSC-HA group and 4.0 cm2 in the microfracture group (P = .051). At 48 weeks, improvement by ≥1 ICRS grade was seen in 97.7% of the UCB-MSC-HA group versus 71.7% of the microfracture group (P = .001); the overall histologic assessment score was also superior in the UCB-MSC-HA group (P = .036). Improvement in VAS pain, WOMAC, and IKDC scores were not significantly different between the groups at 48 weeks, however the clinical results were significantly better in the UCB-MSC-HA group at 3- to 5-year follow-up (P < .05). There were no differences between the groups in adverse events.
Conclusion:
In older patients with symptomatic, large, full-thickness cartilage defects with or without osteoarthritis, UCB-MSC-HA implantation resulted in improved cartilage grade at second-look arthroscopy and provided more improvement in pain and function up to 5 years compared with microfracture.
Registration:
NCT01041001, NCT01626677 (ClinicalTrials.gov identifier).
Keywords
Articular cartilage defects remain a challenging clinical problem. Currently available treatment options are generally more applicable to localized, focal defects in relatively young patients rather than the large, full-thickness, often bipolar lesions typically found in the osteoarthritic joints of older patients. 25,29 Microfracture is a popular option for small cartilage defects, but the results are usually inferior for large chondral defects. 10,20,39 Moreover, microfracture generally leads to fibrous repair tissue with limited durability, just up to 1 or 2 years. 1,48 Autologous chondrocyte implantation (ACI) is typically recommended for large lesions, particularly in younger patients, but ACI procedures are less often indicated in the older population because of the diminished reparative potential of the autologous chondrocytes. 12 Therefore, neither microfracture nor ACI is generally recommended in large chondral defects in older patients. However, many older patients have an active lifestyle and are reluctant to undergo joint replacement, so an innovative regenerative treatment option for this population is needed.
Mesenchymal stem cells (MSCs) have recently been proposed as a potential option for cartilage restoration in elderly patients. MSCs are known to have unique biological characteristics, including immunomodulatory and anti-inflammatory properties and secretion of proregenerative cytokines and chemokines. 3,30 MSCs can be obtained from various tissues of the human body. 13,26 Umbilical cord blood–derived MSCs (UCB-MSCs) have advantages over other MSCs, including noninvasive cell collection, hypoimmunogenicity, and high expansion capacity. 8,19 Moreover, allogeneic MSC implantation has the advantages of 1-step surgery and better quality control of the cells compared with a 2-step procedure such as ACI or a 1-step procedure using autologous cell concentrate such as bone marrow aspirate concentrate or autologous adipose tissue–derived cell therapy, which have heterogeneous cell populations. 18,49
Several preclinical studies have evaluated human UCB-MSCs combined with hyaluronic acid (HA) hydrogels for the restoration of full-thickness cartilage defects. 4,11,33,34,38 A phase 1/2, first-in-human clinical trial has suggested the safety and efficacy of UCB-MSCs when combined with 4% HA hydrogel (UCB-MSC-HA) for the cartilage repair of osteoarthritic defects in older patients; durable improvement was found up to 7 years after treatment. 36 The current study was a randomized controlled phase 3 clinical trial conducted to determine whether implantation of UCB-MSC-HA results in reliable cartilage restoration compared with microfracture (control) in patients with symptomatic, large, full-thickness cartilage defects. The study and control populations were observed for 5 years to determine whether any clinical improvements could be maintained for that duration.
Methods
Study Design
This randomized, active controlled, phase 3, multicenter trial was conducted at 10 tertiary-care hospitals between February 2, 2009, and January 24, 2011. The trial evaluated surgical implantation of an allogeneic UCB-MSC-HA composite versus microfracture for treating full-thickness cartilage defect of the femoral condyle in patients who had knee pain. An observational, extended follow-up study (36, 48, and 60 months) was performed on participants of the phase 3 portion who consented to the follow-up portion.
The trials were conducted according to current Good Clinical Practices and principles of the Declaration of Helsinki (1989). Study protocols were approved by institutional review boards at each institution and the Ministry of Food and Drug Safety (MFDS) of South Korea (equivalent to US Food and Drug Administration) through the investigational new drug pathway.
Participants
Eligible participants were patients aged >18 years with a symptomatic, large, full-thickness femoral condyle or trochlear cartilage defect (2-9 cm2), International Cartilage Repair Society (ICRS) 23 grade 4, in a single compartment of the knee joint as confirmed by arthroscopy, regardless of whether the defect was focal or osteoarthritic. For patients with multiple lesions, the defect in the most symptomatic compartment was considered. Major exclusion criteria included ligament instability of >5 mm or chronic inflammatory articular disease, Kellgren-Lawrence grade 4 osteoarthritis, or significant deformity (>10° varus/valgus). More details of the primary inclusion and exclusion criteria are provided in Appendix Table A1. Informed consent was obtained from all participants.
Microfracture is not the gold standard for large chondral defects, especially in older patients; however, the participants in this clinical trial had experienced failure of previous nonoperative treatment, and another year of placebo control during the trial was not considered ethical or practical by the investigators and the regulatory body (MFDS). Thus, after a discussion with the MFDS and a thorough review of previous reports that showed some clinical benefit of microfracture in similar disease states, 1,48 microfracture was determined as the active control. Patients were recommended not to take nonsteroidal anti-inflammatory drugs, pain relievers, or injections; however, these agents were allowed if needed by the patients, after consultation with their physicians.
After enrollment, participants were randomized 1:1 through use of a stratified, random, permuted block design with block size of 4 to 6. Participants who met the inclusion and exclusion criteria were assigned to either the UCB-MSC-HA group or the microfracture group, randomly as described above. All outcomes were assessed by blinded evaluators. Surgeons and participants could not be double-blinded because of the differences in surgical scars—arthrotomy for UCB-MSC-HA and arthroscopy for microfracture—however, the macroscopic and histologic evaluations were performed in a completely blinded manner by independent evaluators.
Cell Preparation and Characterization
Allogeneic UCB-MSCs were produced at a cell manufacturing facility operated by MEDIPOST Co Ltd, in full compliance with the Good Manufacturing Practice requirements of the MFDS as well as with donor screening, cell isolation and expansion, and quality control measures. In brief, donor umbilical cord blood was collected from full-term infants after informed maternal consent and stored in bags containing anticoagulant. The cord blood was processed within 24 hours of collection. Mononuclear cells in the low-density fraction were separated over Histopaque (density 1.077 g/cm3; Sigma-Aldrich) and then cultured according to a previously published method. 47 The ex vivo culture-expansion manufacturing process of the UCB-MSCs is a scaled adaptation of the technique described by Yang et al 47 and involves initial isolation steps to remove hematopoietic elements, followed by MSC expansion of the nucleated cells in culture medium (alpha-Minimal Essential Medium; Gibco BRL) supplemented with 10% fetal bovine serum. After multiple passage expansion, the UCB-MSCs are cryopreserved at –150°C or colder in the presence of 10% dimethyl sulfoxide. For use in the clinical trial, cryopreserved UCB-MSCs were carefully thawed and subjected to the final passage with harvested cells vialed at a concentration of 7.5 × 106 cells per 1.5 mL and released. Potency, sterility, mycoplasma, and endotoxin testing during the manufacturing process and upon final release were performed in compliance with requirements by the MFDS.
Interventions
For the study population, the UCB-MSC-HA composite was prepared at the time of surgery in the operating room (Appendix Figure A1) and implanted as previously reported in the phase 1/2 clinical trial. 35,36 After a standard arthroscopic examination to assess cartilage defects, during which arthroscopic procedures such as debridement of the cartilage flaps or meniscectomy were performed, a small longitudinal arthrotomy incision was made alongside the patellar tendon to expose the cartilage defect on the femoral condyle. Multiple drill holes (5 × 5 mm [diameter × depth]; approximately 2 mm apart) were made in the subchondral bone for insertion of the UCB-MSC-HA composite. In addition, multiple small drill holes (1.4 × 5 mm [diameter × depth]) were made between the 5-mm drill holes for better lateral integration between the repair tissues from the 5-mm drill holes, based on experience from a previous clinical trial. 36 The UCB-MSC-HA composite was carefully implanted into the 5-mm drill holes to completely fill in the holes (Figure 1). 36 The wound was then closed, and a splint was applied. In the active control group, the traditional microfracture technique was performed, which entailed making multiple awl holes arthroscopically at the subchondral bone. 41
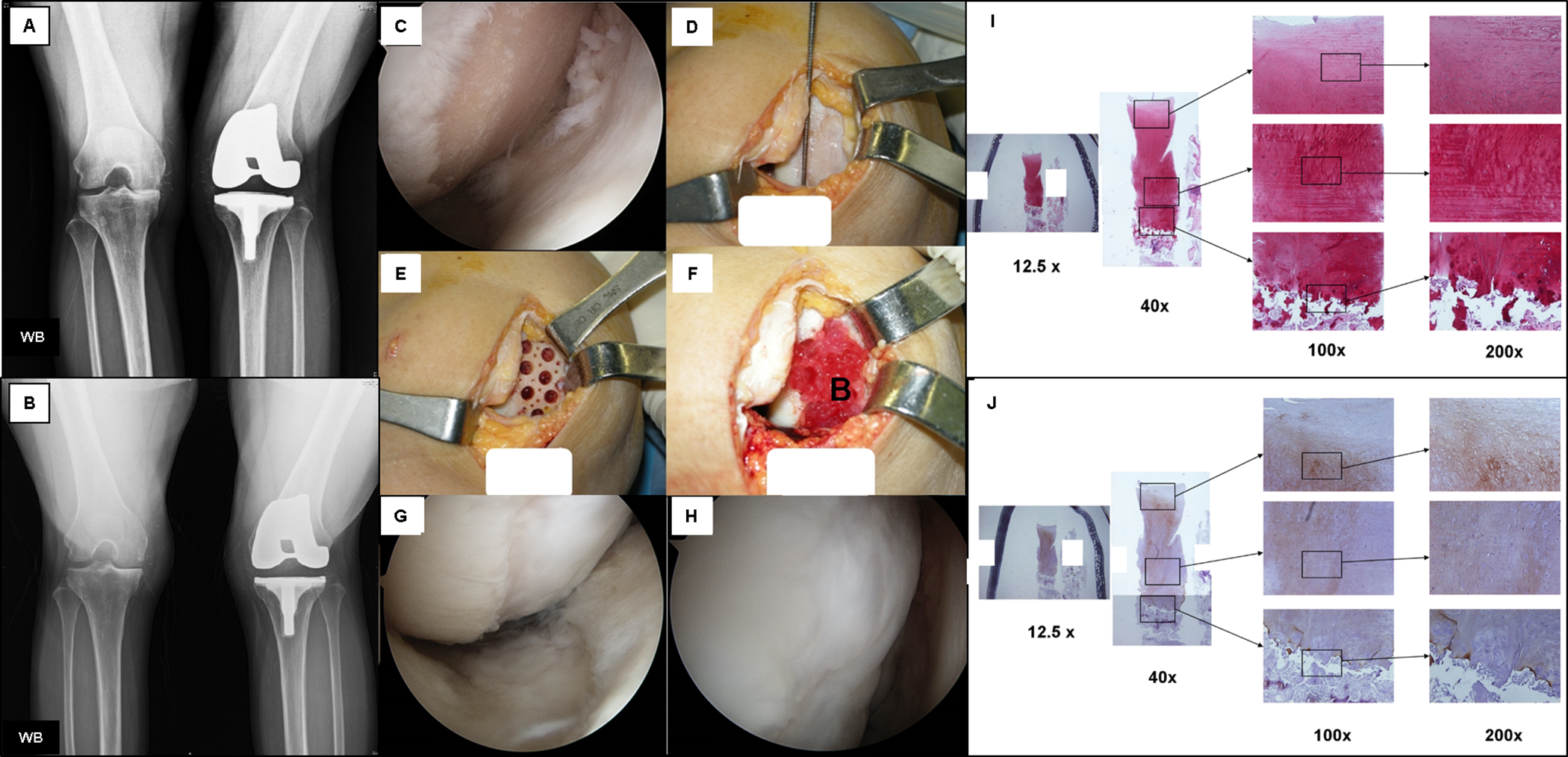
Surgical implantation procedure for the allogeneic human umbilical cord blood–derived mesenchymal stem cell and 4% hyaluronate (UCB-MSC-HA) composite. (A) Preoperative weightbearing (WB) posteroanterior radiograph (Rosenberg view) shows osteophyte formation of the right knee of a 54-year-old female patient. She had previously undergone a total knee arthroplasty for her left knee. (B) The same radiographic view taken at 5-year follow-up shows maintenance of restored medial joint space without significant deterioration. (C) Arthroscopic inspection and confirmation of International Cartilage Repair Society (ICRS) grade 4 cartilage defect at the initial examination. (D) Mini-arthrotomy and measurement of the size of the full-thickness cartilage defect in the medial femoral condyle of the patient’s right knee. (E) Multiple drilling with a drill bit of 5-mm diameter, which is larger than the diameter of holes made during standard microfracture at the subchondral bone. The large drill holes were mainly made for containment of the UCB-MSC-HA composite. (F) Implantation of the UCB-MSC-HA composite in the 5-mm drill holes. (G, H) Restored articular cartilage at 48 weeks after implantation, which was assessed as ICRS grade 3 in this case. (I) Safranin O staining showing abundant presence of glycosaminoglycan in the restored cartilaginous tissue. (J) Type II collagen immunostaining showing abundant type II collagen in the restored cartilaginous tissue.
All participants complied with standardized posttreatment rehabilitation. Quadriceps sitting and straight leg–raising exercises were performed from the day of surgery. Participants were allowed to start active, passive, and active-assisted range of motion exercises from postoperative day 1, progressing as tolerated. Nonweightbearing walking with crutches or a walker was encouraged for the first 12 weeks for the UCB-MSC-HA group and the first 8 weeks for the microfracture group. After the nonweightbearing period had passed, partial weightbearing for 4 weeks followed. We educated participants about the rehabilitation protocol and emphasized the importance of compliance for successful outcome after cartilage repair surgery, as is routine practice for other standard cartilage repair procedures.
Outcome Measures
The primary outcome of the phase 3 clinical trial was the proportion of participants with cartilage restoration equivalent to at least 1 grade improvement on the ICRS Macroscopic Cartilage Repair Assessment at 48-week arthroscopic evaluation (see Appendix Table A2 for scoring). 43 Secondary outcomes were the ICRS II Histological Evaluation System score from tissue biopsies 23,24 and changes in 100-mm visual analog scale (VAS) for pain, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), 2 and International Knee Documentation Committee (IKDC) scores 15 from baseline to 48 weeks. Biopsies of the repair tissue taken from the center of the lesion site during the 48-week arthroscopic evaluation were used for the histologic assessment.
Owing to differences in the surgical scars, the ICRS Macroscopic Cartilage Repair Assessment was conducted in a blinded fashion as follows: Arthroscopic images were captured and videos were recorded during both the initial surgical procedure and the second-look arthroscopy for efficacy evaluation at 48 weeks. Ten investigators were divided into 2 groups (group 1: HC Lim, BK Lee, HJ Jeong, CH Choi, CW Ha; group 2: MK Kim, SI Bin, CH Choi, JD Yoo, JR Yoon), and each group assessed the arthroscopic images and videos of the other group without any information regarding the treatment assignment. The 5 investigators in each group initially assessed preoperative and postoperative images and videos independently using the ICRS Macroscopic Cartilage Repair Assessment. The evaluations were collected and compared to arrive at a final consensus. If agreement was reached by at least 3 of the 5 reviewers, the 3 matching results were selected as the final ICRS grade. For cases of agreement by <3 reviewers, the final grade was determined through an open discussion among the 5 investigators in each group.
The WOMAC is a well-validated, disease-specific measure of osteoarthritis of the hip or knee that includes pain, stiffness, and function subscales and addresses activities of daily living. 2 The IKDC subjective knee form 15 is designed to measure symptoms and limitations in function and sports activity for various knee conditions, including cartilage injuries, and has demonstrated strong psychometric characteristics. The IKDC has shown adequate internal consistency and no remarkable floor or ceiling effects. 5
At 48 weeks, cylindrical biopsies (2-mm diameter) included both restored cartilage tissue and subchondral bone. The biopsies were fixed (4% paraformaldehyde) and embedded in paraffin. Then, 4 μm--thick sections were obtained and stained with hematoxylin and eosin for general morphologic features, Safranin O for glycosaminoglycan, and Masson trichrome for general collagen distribution. Immunohistochemical staining for collagen types I and II was also performed. Biopsies were assessed by 2 blinded, independent professional pathologists according to the ICRS II Histological Evaluation System. 24
Safety was assessed by physical examinations, laboratory tests, adverse event (AE) monitoring, and 24-week ex vivo mixed lymphocyte reaction to allogeneic cells. All of the AEs were categorized using the World Health Organization Common Toxicity Criteria for Adverse Events. 42
In the observational extended follow-up study of 60 months, longer term safety was assessed by any AEs incurred, and longer term efficacy was assessed by VAS pain, WOMAC, 2 and IKDC scores 15 as well as surgical reintervention rates.
Statistical Analysis
We assumed that approximately 40% of the microfracture-treated participants would have an improved ICRS grade based on previous reports, 10,28 and we sought to determine whether the ICRS grade would improve in 70% of UCB-MSC-HA implanted participants. A total of 84 participants (42 per group) would provide 80% power to detect a difference of 40% versus 70% in ICRS grade improvement with a 5%, 2-sided alpha level. With a possible 20% dropout rate, target enrollment was at least 104 participants (52 per group).
Between-group differences for the primary efficacy outcome and subgroup analyses (age and lesion size) were performed using the Fisher exact test. ICRS grade distribution at 48 weeks was compared between groups using the Wilcoxon rank-sum test. For secondary endpoint comparisons, the Wilcoxon rank-sum test or 2-sample t test was used for continuous variables, and the Fisher exact test was used for binary variables. The last observation carried forward was used for missing data at 36, 48, and 60 months. All analyses were performed using SAS 9.3 (SAS Institute), and all P values were 2-sided.
Results
In the 48-week clinical trial, 124 participants were screened and 10 participants were excluded after screening; thus, 114 participants were enrolled and randomized to UCB-MSC-HA (n = 57) or microfracture (n = 57) (Figure 2A). Of these participants, 11 did not receive intervention, leaving 103 participants (50 in the UCB-MSC-HA group and 53 in the microfracture group). Ultimately, 89 participants (86.4%; 43 in the UCB-MSC-HA group and 46 in the microfracture group) completed the 48-week primary endpoint assessment by second-look arthroscopy (Figure 2A), and 87 participants (84.5%) had biopsy samples taken (tissue acquisition failed in 2 participants).

CONSORT (Consolidated Standards of Reporting Trials) flow diagram of study participants. (A) Phase 3 clinical trial of 48 weeks. (B) Observational extended follow-up study of 60 months. *Some of the participants were lost to follow-up at specific follow-up time points only (eg, a participant who was “lost to follow-up” at the 36- and 48-month timepoints could have been included at the 60-month timepoint, and vice versa). AE, adverse event; UCB-MSCs-HA, umbilical cord blood–derived mesenchymal stem cells and 4% hyaluronate.
Demographics, lesion characteristics, and baseline scores were comparable between the 2 groups (Table 1). The mean age of participants was 55.3 years in the UCB-MSC-HA group and 54.4 years in the microfracture group; mean body mass index was 52.7 (UCB-MSC-HA) and 26.7 (microfracture); the male-to-female ratio was similar in both groups; and osteoarthritis was the most prevalent diagnosis in both groups: 95.4% in the UCB-MSC-HA group and 91.3% in the microfracture group (Table 1). The mean lesion size was 4.9 cm2 in the UCB-MSC-HA group and 4.0 cm2 in the microfracture group (P = .051). All treated defects were on the femur, mostly on the medial femoral condyle (83.1%).
Demographics and Baseline Characteristics of Study Participants a
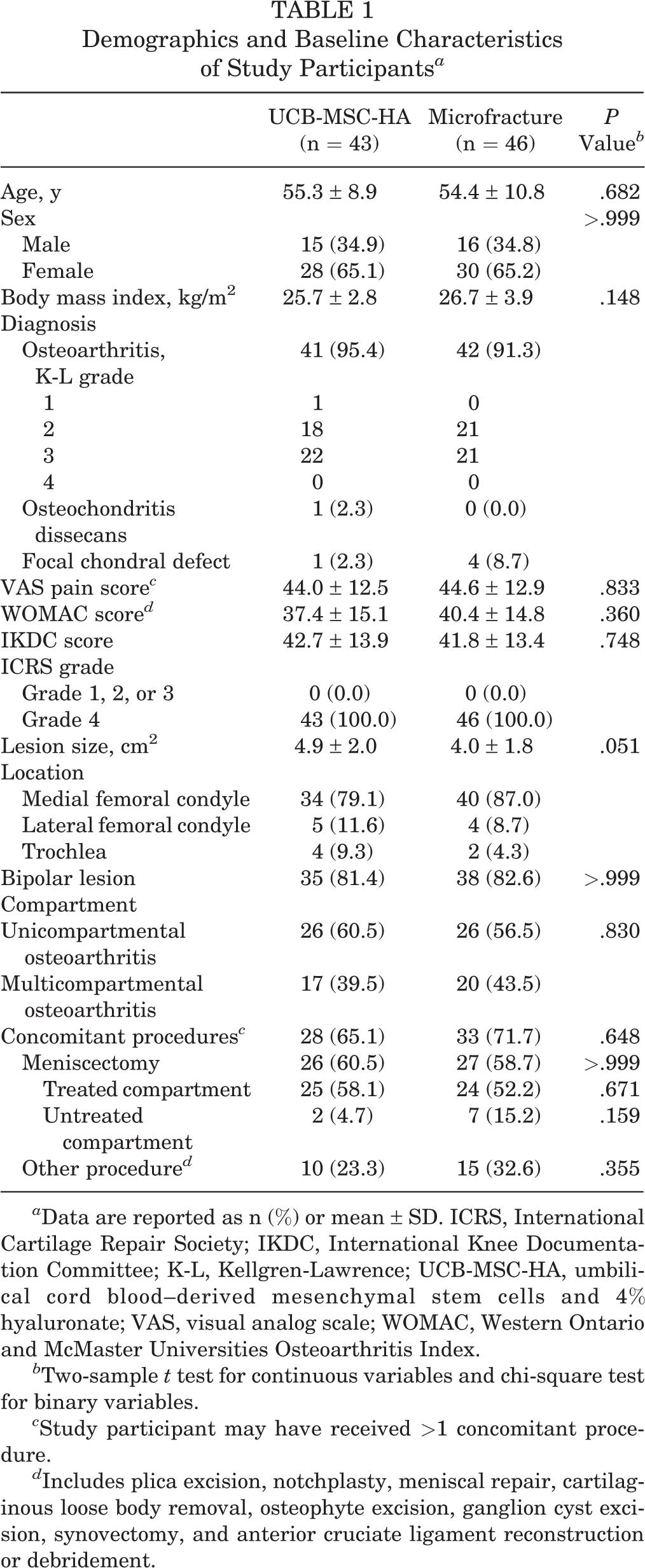
a Data are reported as n (%) or mean ± SD. ICRS, International Cartilage Repair Society; IKDC, International Knee Documentation Committee; K-L, Kellgren-Lawrence; UCB-MSC-HA, umbilical cord blood–derived mesenchymal stem cells and 4% hyaluronate; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Two-sample t test for continuous variables and chi-square test for binary variables.
c Study participant may have received >1 concomitant procedure.
d Includes plica excision, notchplasty, meniscal repair, cartilaginous loose body removal, osteophyte excision, ganglion cyst excision, synovectomy, and anterior cruciate ligament reconstruction or debridement.
Among the 89 participants who completed the initial 48-week clinical trial, 73 were enrolled in the extended observational 60-month follow-up study (Figure 2B). Detailed information on participants of the extended follow-up study is provided in Appendix Table A3. There were no significant differences in baseline characteristics between the groups at 60-month follow-up.
Efficacy Outcomes
Phase 3 Clinical Trial at 48 Weeks
The primary outcome analysis revealed that the proportion of participants showing improvement of ≥1 ICRS grade at 48 weeks was 97.7% (42/43) in the UCB-MSC-HA group and 71.7% (33/46) in the microfracture group (odds ratio, 16.55; 95% CI, 2.06-133.03; P = .001) (Table 2). The proportion of participants showing the restored cartilage status as ICRS Macroscopic Cartilage Repair Assessment grade 1 or 2 was 65.1% in the UCB-MSC-HA group and 45.7% in the microfracture group (Table 2). The distribution of ICRS repair assessment grade for UCB-MSC-HA versus microfracture was significantly different (P = .008). Subgroup analyses according to age (<50, 50-59, and ≥60 years) demonstrated that the improvement in ICRS grade was affected by age in the microfracture group (100%, 61.9%, and 64.3%, respectively) but not in the UCB-MSC-HA group (100%, 95.5%, and 100%, respectively) (Table 2). Subgroup analyses according to size of cartilage defect (2.0 to 3.0, >3.0 to <6.0, and ≥6.0 cm2) also demonstrated that the efficacy of microfracture decreased as the lesion size increased (100%, 63.6%, and 44.4%, respectively), but that tendency was not noticeable in the UCB-MSC-HA group (100%, 100%, and 93.3%, respectively) (Table 2).
Primary Outcome of Phase 3 Clinical Trial (48 weeks) a

a Data are reported as n (%) unless otherwise indicated. 9/9 means that 9 patients showed minimum grade 1 improvement in ICRS grade among 9 patients less than 50 years old. ICRS, International Cartilage Repair Society Macroscopic Cartilage Repair Assessment; NA, not applicable; UCB-MSC-HA, umbilical cord blood–derived mesenchymal stem cells and 4% hyaluronate.
b Pearson chi-square test.
c Wilcoxon rank-sum test.
Scores on the ICRS Macroscopic Cartilage Repair Assessment were significantly higher in the UCB-MSC-HA group, both overall and for every subcategory (degree of defect repair, integration to border zone, and macroscopic appearance) (Table 3). Histologic assessment according to the ICRS II Histological Evaluation System also revealed that the UCB-MSC-HA group had better histologic restoration in terms of the overall score, the subchondral bone assessment, and the mid-/deep zone assessment (Table 3). Both groups had significantly improved VAS pain, WOMAC, and IKDC scores at 48 weeks versus baseline (P < .05). No significant difference was seen between the 2 groups regarding these clinical parameters at 48 weeks (Figure 3).
Summary of Macroscopic and Histologic Evaluation of Phase 3 Clinical Trial (48 weeks) a

a Data are reported as mean ± SD. ICRS, International Cartilage Repair Society; UCB-MSC-HA, umbilical cord blood–derived mesenchymal stem cells and 4% hyaluronate.
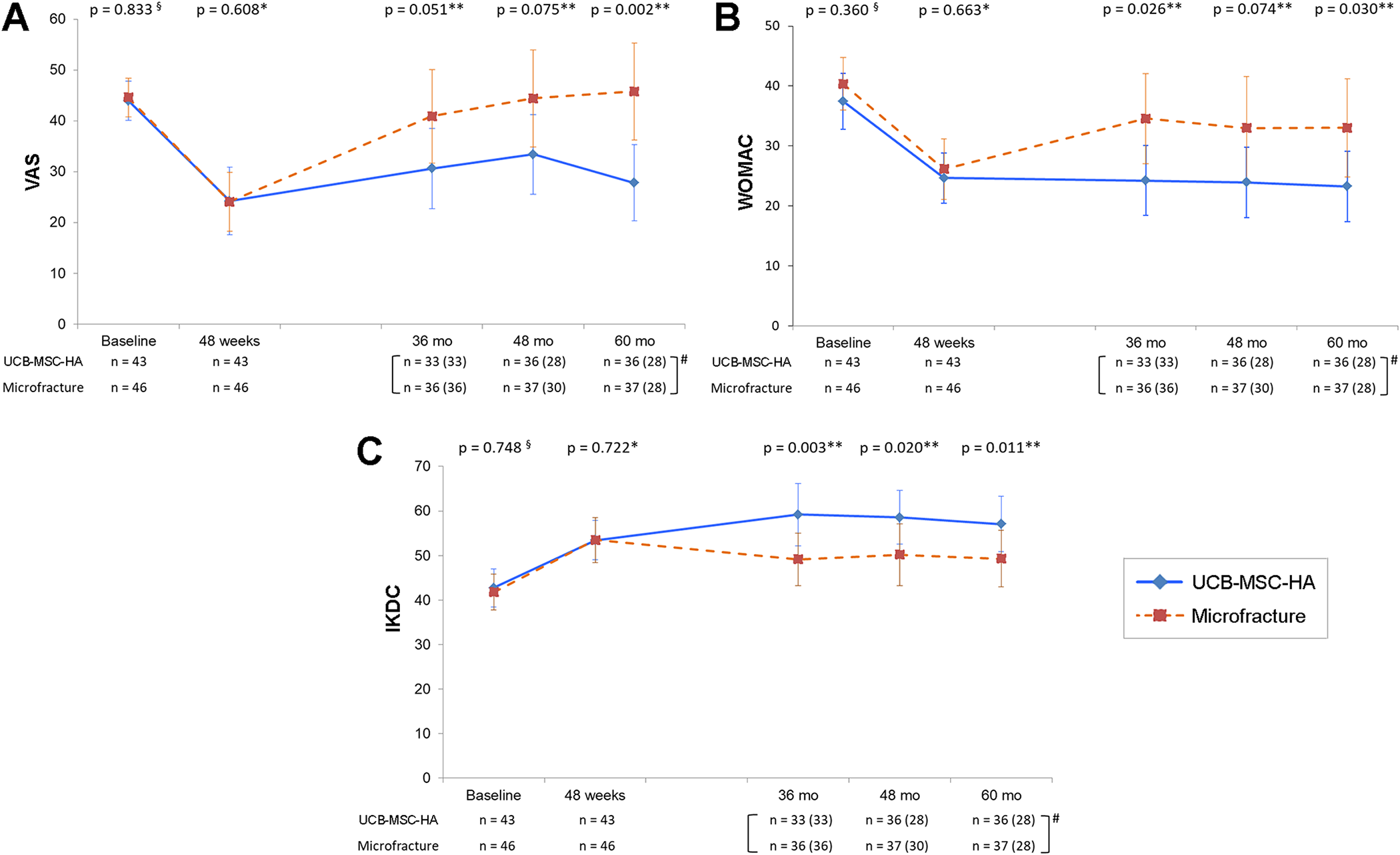
Clinical outcomes from baseline to 60-month follow-up in the umbilical cord blood–derived mesenchymal stem cells and 4% hyaluronate (UCB-MSC-HA) versus microfracture groups. Vertical bars indicate 95% CIs for the mean scores. (A) Visual analog scale (VAS) for pain; (B) Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC); and (C) International Knee Documentation Committee (IKDC) score. §2-sample t test. *Wilcoxon rank-sum test on score changes from baseline to the time point. **2-sample t test on score changes from baseline to the time point. #Sample sizes for follow-up study (36, 48, and 60 months) include missing data replacements using last observation carried forward (LOCF). The numbers in parentheses indicate the participants assessed at each time point.
Observational Extended Follow-up Study of 60 Months
From 36 to 60 months after intervention, the significant improvements from baseline regarding VAS pain, WOMAC, and IKDC scores were maintained in the UCB-MSC-HA group, whereas the improvements in VAS pain and WOMAC deteriorated in the microfracture group (Figure 3). The VAS pain score was significantly better in the UCB-MSC-HA group compared with the microfracture group at the 60-month follow-up (Figure 3A). The WOMAC and IKDC scores were significantly better in the UCB-MSC-HA group than in the microfracture group at the 36- and 60-month follow-up (Figure 3, B and C). In addition, improvement in VAS pain, WOMAC, and IKDC scores at 36- and 60-month follow-up in the UCB-MSC-HA group was greater than the minimal clinically important difference (MCID; VAS 13.7, 14 IKDC 11.5, 16 and WOMAC 11.5 9 ), but this was not the case in the microfracture group (Appendix Table A4).
By the 60-month follow-up, 2 total knee replacements and 1 osteotomy had been performed in the UCB-MSC-HA group, whereas 3 total knee replacements, 1 osteotomy, and 1 meniscectomy had been performed in the microfracture group (P = .481) (Table 4).
Serious Adverse Events of Phase 3 Clinical Trial (48 weeks) and Extended Follow-up Study (60 months) a

a Data are reported as n (%). UCB-MSC-HA, umbilical cord blood–derived mesenchymal stem cells and 4% hyaluronate.
Safety
No significant differences were observed between the UCB-MSC-HA group and the microfracture group with regard to overall or specific treatment-emergent AEs in the initial 48-week clinical trial (Appendix Table A5) or the 60-month follow-up study (Appendix Table A6). No participant was withdrawn from the study because of AEs.
Three serious AEs (SAEs) occurred in 3 participants in the UCB-MSC-HA group, whereas 2 SAEs occurred in 1 participant in the microfracture group within the initial 48 weeks (Table 4). Surgical site pain in the UCB-MSC-HA group was the only SAE considered by the investigator as “probably related” to treatment (due to arthrotomy). In the 60-month follow-up, 8 SAEs occurred in 7 participants in the UCB-MSC-HA group and 7 SAEs in 5 participants in the microfracture group (Table 4). None of the SAEs were considered treatment related by the investigators. The patients who underwent total knee arthroplasty and high tibial osteotomy were considered to have required the procedure as a natural course of osteoarthritis and not because of implantation of the UCB-MSC-HA composite or microfracture. One death due to myocardial infarction (at 41 months postintervention) was reported in the UCB-MSC-HA group. No immunological reactions were observed in any of the 43 participants treated with UCB-MSC-HA, according to the mixed lymphocyte reaction test.
Discussion
The results of the present study demonstrated that implantation of UCB-MSC-HA provides superior cartilage restoration compared with microfracture at 48 weeks after intervention, meeting the a priori primary endpoint in patients with symptomatic, large, full-thickness cartilage defects. The UCB-MSC-HA group demonstrated consistent improvement in ICRS grade of cartilage repair, even in the patients and those with larger lesions, whereas microfracture resulted in unreliable improvement in these groups. Of note, baseline IKDC score and cartilage restoration with microfracture in this study were inferior to those of at least 1 other study, 40 likely due to older patient age (mean age, 56 vs 34 years) and inclusion of large, full-thickness lesions in osteoarthritic knees in the present study versus focal chondral defects treated in the other study. A reliable regenerative treatment option is not currently available for large cartilage defects in older patients with osteoarthritis, and our study results indicate that this novel application of UCB-MSC-HA may be applicable to these patients. UCB-MSC-HA may be an alternative treatment option to unicompartmental knee arthroplasty for those who desire joint preservation and the maintenance of an active lifestyle.
Despite the superior structural restoration after implantation of UCB-MSC-HA as assessed macroscopically and histologically, clinical outcomes such as pain and function at 48 weeks were not significantly superior to those experienced by patients who underwent microfracture. That both groups showed significant improvement in clinical outcomes at 48 weeks compared with baseline seemed to justify our decision to use microfracture as an active control rather than placebo.
No reliable gold standard is available to be used as the active control in studies of large, full-thickness cartilage defects; however, the results of the current study support previous findings that microfracture can provide clinical benefit for this condition for at least 1 year. In this study, the microfracture group showed deterioration in clinical outcomes after 3 years, which is compatible with many previous reports. 21,27,28 In the UCB-MSC-HA group, the improvements in pain and knee function were maintained without significant deterioration until 5 years after implantation. However, improvements in IKDC score were relatively low, and VAS pain scores of 20 to 30 were found at final follow-up. Although it is difficult to pinpoint the reason for the relatively low clinical outcomes, the status of knee osteoarthritis in the older patients in this study population could have affected the results.
In this study, clinical outcome improvements were greater than the MCID only in the UCB-MSC-HA group. Moreover, most of the clinical outcomes that were significantly superior in the UCB-MSC-HA group occurred in the 3 to 5 years after the intervention. We believe the difference may stem from the better quality of the restored cartilage tissue in the UCB-MSC-HA group compared with the microfracture group, as demonstrated by histologic testing at 48 weeks.
To date, few cartilage repair methods have been clinically successful in large, full-thickness cartilage defects, which are typical in patients with osteoarthritic knees. 6 In this regard, a novel regenerative strategy is needed for the treatment of such defects, especially in elderly patients. The UCB-MSC-HA in this study has the advantage of being available off-the-shelf and requiring only a single-stage procedure. The previous phase 1/2, single-arm study of UCB-MSC-HA implantation demonstrated that the improved clinical outcomes had not significantly deteriorated >7 years after treatment. 36 The results of the present study confirmed that cartilage restoration by UCB-MSC-HA leads to sustained clinical improvement until 5 years postintervention, which is encouraging for joint preservation. As osteoarthritic cartilage defects were present in about 90% of the study participants (see Table 1), we believe that UCB-MSC-HA is a viable treatment option for the regenerative treatment of large, full-thickness cartilage defects, even in osteoarthritic conditions.
Cartilage restoration using culture-expanded autologous MSCs has previously been attempted; however, the studies are limited to case reports or case series with small numbers of patients. 17,22,31,32,37,45 Two randomized clinical trials (RCTs) examined the efficacy of culture-expanded, autologous bone marrow–derived MSCs embedded in a collagen gel 45 or injected intra-articularly with hyaluronate 46 for the treatment of osteoarthritis. However, we believe that the clinical outcomes in those studies were confounded by concomitant high tibial osteotomy. In a double-blind RCT (N = 55) of intra-articular allogeneic, culture-expanded bone marrow MSCs versus hyaluronate after partial medial meniscectomy in patients with osteoarthritic changes, the authors reported no evidence of structural cartilage restoration at 1 year, which was the primary endpoint of the trial. 44 Our phase 3, 48-week study seems to be the first RCT of allogeneic, culture-expanded UCB-MSC implantation, and the results indicate cartilage restoration as well as improved pain and function until 5 years postintervention.
The rate of additional surgical intervention such as high tibial osteotomy and total knee arthroplasty was relatively low and was similar in both groups (6.0% in the UCB-MSC-HA group vs 7.6% in the microfracture group) during the extended follow-up period. Most of the study patients were middle-aged and physically active, and patients often consider knee replacement or osteotomy as a last resort. Therefore, we believe that only a few patients with severe deterioration during the extended follow-up period underwent replacement or osteotomy. Further long-term follow-up may reveal the need for surgical reintervention after treatment with UCB-MSC-HA composite compared with microfracture.
This study has certain limitations. First, this study was open-label to the patients and surgeons. However, it could not be double-blinded because arthrotomy was performed on the UCB-MSC-HA group and arthroscopy on the microfracture group. Sham surgery or microfracture using open arthrotomy could have been the best control group, but the regulatory authority and investigators agreed that such measures would have been unethical or too aggressive. We minimized bias by having blinded professionals assess the primary outcome (ICRS Macroscopic Cartilage Repair Assessment score) as well as the secondary outcome (ICRS II Histological Evaluation System score). Second, microfracture is not generally considered the standard care option for the restoration of large, full-thickness cartilage defects, especially in elderly patients. However, a placebo control was not ethical or practical for our study patients, as discussed in the Methods. Implantation of HA only without MSCs was also considered as a control intervention. However, the results of previous animal studies showed no meaningful cartilage restoration with such a method. 7,38 A third limitation was that the participants received the intervention for only the femoral cartilage defect in the “most symptomatic” compartment. Thus, the effect of any untreated lesion in the intervention joint could not be determined. However, the results of the present study reveal the clinical benefit of treating only the most symptomatic lesion. Further research on the treatment of multiple lesions is warranted.
Conclusion
Implantation of UCB-MSC-HA resulted in improved cartilage grade at second-look arthroscopy at 48 weeks and provided more durable improvement of pain and function compared with microfracture in patients with symptomatic, large, full-thickness cartilage defects. UCB-MSC-HA appears to be a viable regenerative treatment option for large, full-thickness cartilage defects of the knee in older patients with osteoarthritis.
Footnotes
Acknowledgment
The authors thank the study coordinators at the participating centers for their efforts in collecting clinical data and ensuring the accuracy and completeness of the data. The authors also thank Sin-Ho Jung, PhD, Joong Hyun Ahn, MS, and Seonwoo Kim, PhD, who contributed to the statistical analyses.
Authors
Jung-Ro Yoon, MD (Department of Orthopedic Surgery, Veterans Health Service Medical Center, Seoul, Republic of Korea); Jun-Young Chung, MD (Department of Orthopedic Surgery, Ajou University Hospital, Ajou University School of Medicine, Suwon, Republic of Korea).
Final revision submitted June 4, 2020; accepted June 17, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was sponsored and funded by Medipost, the manufacturer of Cartistem. Funding was also received from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number HI14C3484). B.J.C. has received research support from Aesculap/B.Braun, Arthrex, and Regentis; educational support from Medwest; consulting fees from Acumed, Anika Therapeutics, Arthrex, Bioventus, Flexion Therapeutics, Geistlich Pharma, Regentis, Smith & Nephew, Vericel, and Zimmer Biomet; speaking fees from Arthrex and Lifenet Health; royalties from Arthrex, DJO, Elsevier, and Operative Techniques in Sports Medicine; other financial or material support from Athletico and JRF Ortho; hospitality payments from GE Healthcare; and honoraria from Vericel; and he has stock/stock options in Bandgrip, Ossio, and Regentis. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Ministry of Food and Drug Safety of South Korea (ID No. MP-CRP-MSC005).
Most Frequently Reported (≥5%) Treatment-Emergent Adverse Events From the Follow-up Study (60 months) a

| Treatment-Emergent Adverse Event | UCB-MSC-HA |
Microfracture |
|---|---|---|
| Back pain | 2 (5.6) | 2 (5.4) |
| Toothache | 2 (5.6) | 1 (2.7) |
| Upper respiratory tract infection | 2 (5.6) | 1 (2.7) |
| Urinary tract infection | 2 (5.6) | 0 (0) |
| Nausea | 2 (5.6) | 0 (0) |
| Vomiting | 2 (5.6) | 0 (0) |
| Headache | 2 (5.6) | 0 (0) |
| Dysuria | 2 (5.6) | 0 (0) |
| Hematuria | 2 (5.6) | 0 (0) |
| Stress urinary incontinence | 2 (5.6) | 0 (0) |
| Allergic rhinitis | 2 (5.6) | 0 (0) |
| Arthralgia | 1 (2.8) | 3 (8.1) |
| Arthritis | 0 (0) | 2 (5.4) |
| Arthropathy | 0 (0) | 2 (5.4) |
| Hemorrhoids | 0 (0) | 2 (5.4) |
| Meniscal lesion | 0 (0) | 2 (5.4) |
| Blood glucose increase | 0 (0) | 2 (5.4) |
a Data are reported as n (%). UCB-MSC-HA, umbilical cord blood–derived mesenchymal stem cells and 4% hyaluronate.