
Abstract
Background:
Although many studies have examined allograft extrusion after medial meniscal allograft transplant (MMAT), it is unclear whether allograft extrusion progresses at midterm follow-up.
Hypothesis:
After MMAT, allograft extrusion would not progress during the midterm follow-up period.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 30 patients who underwent MMAT between December 1996 and March 2016 were enrolled. Allograft extrusion was measured on magnetic resonance imaging scans obtained at 6 weeks, 1 year, and 3 to 7 years postoperatively. In the coronal plane, the absolute allograft extrusion and relative percentage of extrusion were measured. In the sagittal plane, the absolute and relative anterior cartilage meniscal distance and posterior cartilage meniscal distance were measured. The joint-space width (JSW) on radiographic Rosenberg view was measured at 3 time points. The axial alignment was measured preoperatively and at the midterm follow-up.
Results:
In the coronal plane, there were no significant differences in absolute and relative coronal extrusions between 6 weeks and 1 year postoperatively; however, the values were significantly increased at midterm follow-up compared with both of the earlier follow-up periods. Similarly, in the sagittal plane, the mean absolute and relative anterior and posterior cartilage meniscal distances were not significantly different between 6 weeks and 1 year postoperatively but showed significant increases at midterm follow-up compared with both of the earlier follow-up periods. The mean preoperative axial alignment showed a positive correlation with the delta value of relative percentage of extrusion in the coronal plane (r = 0.378; P = .036). The mean JSW was 4.42 ± 0.88 mm preoperatively, 4.30 ± 0.83 mm at 1-year follow-up, and 3.96 ± 1.06 mm at the midterm follow-up. No significant difference was found between the preoperative and postoperative 1-year values, but the mean JSW was significantly decreased at midterm follow-up compared with both of the other time points (P = .001 for both).
Conclusion:
Allograft extrusion did not progress until 1 year after MMAT; however, by midterm follow-up, extrusion had progressed in both the coronal and the sagittal planes. Preoperative axial alignment showed a positive correlation with allograft extrusion in the coronal plane.
The meniscus plays important roles in the knee joint, such as load sharing and transmission, shock absorption, joint stability, lubrication, and proprioception. 2,7,24,29 Meniscectomy changes the normal contact mechanics in the tibiofemoral joint. For example, after total medial meniscectomy, the contact stress of the medial compartment of the knee joint is doubled compared with that of the normal joint. 2 Meniscal allograft transplant (MAT) is an effective treatment option for subtotal or total meniscectomized knees in relatively young patients. 15 Several studies have shown that MAT reduces pain and improves knee function during activities of daily living, and favorable clinical outcomes have been reported in short-, mid-, and long-term follow-up studies. 11,22,27,31,33 In some studies, MAT appears to prevent the progression of osteoarthritic change in the affected compartment, although it does not completely restore the function of the native meniscus. 30
Allograft extrusion is a relatively common finding in magnetic resonance imaging (MRI) evaluations conducted to confirm the postoperative status of the allograft after MAT, and many studies have attempted to find the related factors. 14,16 –19 In the native knee joint, meniscal extrusion is associated with underlying meniscal tear or joint degeneration. 5 Various factors, such as anatomic horn position 12 and osteophytes in the tibial plateau, have been reported to be related to allograft extrusion 10 ; however, the exact cause of extrusion is unknown. Allograft extrusion can lead to a biomechanical disadvantage that can cause failure of the allograft to perform functions, such as shock absorption and load distribution, thus reducing the benefits of MAT. 6,8
In a previous study, it was reported that allograft extrusion in patients who underwent lateral MAT (LMAT) did not progress in both the coronal and sagittal planes during the short-term and midterm follow-up periods. 13 In a study on medial MAT (MMAT), allograft extrusion in the coronal plane did not increase until 1 year after surgery. 12 However, no study has analyzed allograft extrusion during the midterm period after MMAT. A previous study comparing extrusion after MMAT and LMAT reported that the incidence of major graft extrusion postoperatively was higher in the MMAT group than in the LMAT group. 19 The objectives of our study were to investigate whether there is an increase in allograft extrusion at midterm follow-up after MMAT, whether there are factors affecting allograft extrusion, and whether increased allograft extrusion has clinical significance. On the basis of these theoretical backgrounds, we hypothesized that allograft extrusion in the midterm follow-up period would not increase in the coronal and sagittal planes in patients who underwent MMAT, similar to results reported in patients who underwent LMAT.
Methods
Patients
Patients who underwent MMAT via the bone-plug technique between December 1996 and March 2016 were retrospectively reviewed. Those who received follow-up care during the midterm period (3-7 years after surgery) and who underwent MRI of the operated knee at the 6-week, 1-year, and midterm follow-ups were included. All MMAT surgeries were performed by a single experienced orthopaedic surgeon (S.-I.B.) who had performed >100 MMAT surgeries. The indications for MMAT were as follows: patient age 16 to 55 years, normal axial alignment of the lower extremities without an apparent varus or valgus deformity on standing radiographs, and persistent medial knee pain or swelling attributed to the absence of the medial meniscus. The contraindications for MMAT included grade III or IV generalized or medial compartment degenerative osteoarthritis, uncorrected knee instability, axial malalignment (>5° deviation toward the involved compartment) of the lower extremities, skeletal immaturity, and patient age >55 years. This study was approved by our institutional review board and each patient provided written informed consent.
Preoperative Sizing of the Meniscal Allograft
For allograft sizing, true anteroposterior and lateral radiographs of the knee were taken. To minimize magnification and avoid the risk of inaccurate bony landmark measurements, a 100-mm radio-opaque rod was used. The medial meniscal allograft size was measured using the method described by Pollard et al. 25 On anteroposterior radiographs, the medial meniscal width was equal to the coronal length from the peak of the medial tibial eminence to the medial margin of the tibial plateau. The sagittal length of the medial meniscus was 80% of the sagittal tibial plateau (measured at the joint between a line parallel to the anterior tibia above the tibial tuberosity and a line tangent to the posterior plateau margin perpendicular to the joint line). After we determined the appropriate size of the meniscal allograft, the desired meniscal size was communicated to the tissue bank (Cellumed; Seoul, Republic of Korea), which provides fresh-frozen medial meniscal allografts (without irradiation and chemical processing) that never exceed a 5% mismatch of coronal or sagittal length.
Surgical Technique and Postoperative Rehabilitation
All medial menisci were transplanted using a fresh-frozen meniscal allograft through the double bone-plug technique. All knees were arthroscopically examined to determine the status of the meniscus, ligaments, and cartilage. Debridement of the host menisci was performed, leaving a 1- to 2-mm bleeding peripheral rim. A 10 mm--diameter anterior bone plug and an 8 mm--diameter posterior bone plug were prepared. Two No. 2 Ethibond sutures (Ethicon) were placed using a whipstitch at each horn, and the posteromedial side of the allograft was sutured using 2 leading sutures. Posterior and anterior bone tunnels were created at the center of each horn’s footprint. The meniscal allograft was passed through an anteromedial arthrotomy. After the optimal allograft position was confirmed, a traditional inside-out meniscal repair was performed using No. 2-0 nonabsorbable sutures (Multi-Fix double armed needle; Ortho Tech) placed 3 to 5 mm apart, then the anterior and posterior bone-plug stitches were tied firmly together.
The patients were instructed to perform isometric muscle strengthening exercises and calf pumps immediately after surgery. Continuous passive range of motion (ROM) exercise was initiated 1 day after MAT. The goal of the ROM exercise was to achieve 90° of flexion within 4 weeks and 120° of flexion at 6 to 8 weeks. Attempting full extension was encouraged from the beginning of the ROM exercise. Patients were allowed toe-touch weightbearing during the first 2 weeks. Full weightbearing was gradually allowed during postoperative weeks 6 through 8. With a focus on restoring full ROM and quadriceps strength, rehabilitation continued for 3 months after the surgery.
MRI Evaluation of Allograft Extrusion
MRI of the transplanted knee joint was performed at 6 weeks, 1 year, and 3 to 7 years postoperatively. Coronal and sagittal images were acquired at slice thicknesses of 2.5 and 1.5 mm, respectively. Meniscal subluxation was measured using the method described by Verdonk et al. 32 All measurements were performed using a digital caliper in a Picture Archiving and Communications System via sagittal and coronal proton density-weighted, fast spin echo MRI. The image showing the longest subluxation was used for the measurement because the amount of subluxation beyond the margin of the tibial articular cartilage may differ among MRI scans. A meniscal subluxation of >3 mm was considered extrusion. The meniscal subluxation distance in the coronal plane was defined as the distance between the outer edge of the articular cartilage of the tibial plateau and the outer edge of the meniscus. Because the individual knee sizes were different, allograft extrusion was measured as relative and absolute values. The relative value was defined as relative percentage of extrusion (RPE) and measured by dividing the absolute value of allograft extrusion by the entire meniscal width (Figure 1A).

Schematic view of meniscal allograft extrusion on magnetic resonance imaging scan. (A) In the coronal plane, absolute extrusion, a, was defined as the distance between the outer edge of the tibial articular cartilage and the outer edge of the meniscal allograft. The relative percentage of extrusion was defined as the percentage of the width of absolute extrusion, a, relative to the width of the entire meniscus, b. (B) In the sagittal plane, absolute anterior horn extrusion, a, was defined as the maximum distance from the anterior articular cartilage margin to the anterior border of the anterior horn. This value was defined as the anterior cartilage meniscal distance. Similarly, absolute posterior horn extrusion, c, was defined as the maximum distance from the posterior articular cartilage margin to the anterior border of the posterior horn. This value was defined as the posterior cartilage meniscal distance. The relative value of sagittal extrusion was determined by dividing the width of extrusion by the entire meniscal width, b or d ([a/b × 100] or [c/d × 100]). Extrusion was indicated as a positive value, and intrusion was defined as a negative value.
The extrusion of transplanted allografts relative to the anterior and posterior horns was evaluated on sagittal MRI scans. Anterior extrusion of the graft in the sagittal plane was defined as the maximum distance from the anterior articular cartilage margin to the anterior border of the anterior horn of the transplanted meniscus (anterior cartilage meniscal distance [ACMD]). Likewise, posterior extrusion of the graft in the sagittal plane was defined as the distance from the posterior articular cartilage margin to the posterior border of the posterior horn of the transplanted meniscus (posterior cartilage meniscal distance [PCMD]). The relative ACMD and PCMD values were calculated as absolute extrusion divided by the width of the entire meniscus in the sagittal plane (Figure 1B). Extrusion of the ACMD or PCMD outside the anterior or posterior border of the articular cartilage was expressed as a positive value, whereas extrusion inside these borders was expressed as a negative value. These MRI measurements were performed by 2 orthopaedic surgeons (H.K. and Tae-Hyuk Kim, MD), and the mean values of the measured data at intervals of 3 weeks were used.
Radiographic Evaluation of the Joint-Space Width and Axial Alignment
To evaluate the progression of degenerative change of the knee joint, the joint-space width (JSW) was measured on weightbearing posteroanterior radiographs at 45° of flexion (Rosenberg view) by 2 orthopaedic fellowship specialists (H.K. and Tae-Hyuk Kim, MD). All images were acquired with the knee in 10° of internal rotation and centered midway between both knees at the level of the popliteal crease on a 14 × 17–inch film. The distance between the focus and film was 72 inches (182.88 cm), and the x-ray beam was angled 10° caudally. The JSW on radiographs was measured at 3 time points: 2 days before surgery, 1 year after surgery, and at the midterm follow-up. The JSW was measured at the point at which the distance between the femur and the tibia was the narrowest. To measure preoperative axial alignment, long-standing hip-knee-ankle radiographs with the patella facing forward were conducted 2 days before the surgery. In the same way, the axial alignment was measured at the midterm period. Varus alignment was indicated as a positive value, and valgus alignment was indicated as a negative value.
Clinical Assessment
To compare clinical outcomes, a physician assistant who was blinded to the study details measured the Lysholm score preoperatively, 1 year postoperatively, and at the midterm follow-up. If the ipsilateral knee had a previous history of surgery, the Lysholm score after the previous surgery was measured. In addition, the correlation between the Lysholm score and other radiologic findings, such as the absolute values of allograft extrusion, the RPE, and the JSW, was investigated.
Statistical Analysis
The absolute values of allograft extrusion, the RPE, the JSW, and the Lysholm score at different time points were compared across time points (6 weeks, 1 year, and 3-7 years postoperatively) using repeated-measures analysis of variance. Correlation between coronal extrusion and axial alignment was measured using the Pearson correlation coefficient. The Pearson correlation coefficient was also used to determine the correlation between Lysholm scores and radiologic findings. The reliability of measurements of extrusion and the JSW was assessed using the intraclass correlation coefficient (ICC), which quantifies the proportion of the difference due to measurement variability. According to ICC values, reliability was judged as follows: >0.9, excellent; 0.76-0.9, good; 0.5-0.75, moderate; and <0.5, poor. All statistical analyses were performed using SPSS Version 21.0 (IBM Corp). A P value of <.05 was considered statistically significant.
Results
A total of 87 patients who underwent MMAT between December 1996 and March 2016 were initially enrolled in this study; of these, 57 patients were lost to follow-up at 6 weeks, 1 year, or the midterm period or did not undergo MRI at these time points. Ultimately, 30 patients were included in the study. The mean midterm follow-up duration was 62.4 ± 12.7 months (range, 42-78 months). Patient characteristics are included in Table 1.
Patient Characteristics (N = 30)

Reliability of Measurements
The interobserver reliability for measurements of the extrusion and the JSW ranged from 0.751 to 0.837, and the intraobserver reliability ranged from 0.827 to 0.909. In all cases, these values indicated good reliability (Table 2).
Intraclass Correlation Coefficients of Interobserver and Intraobserver Reliability a
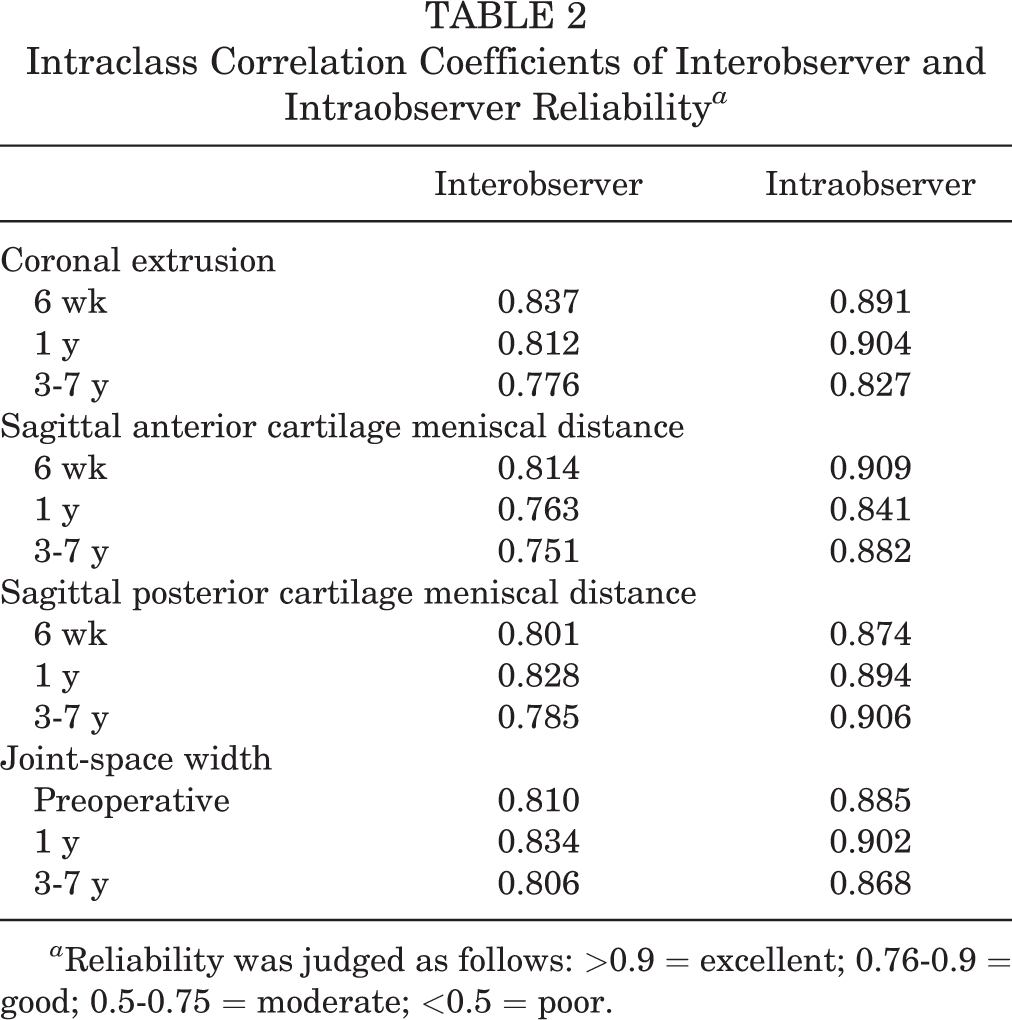
a Reliability was judged as follows: >0.9 = excellent; 0.76-0.9 = good; 0.5-0.75 = moderate; <0.5 = poor.
Radiologic Allograft Extrusion in the Coronal Plane
In the coronal plane, the mean absolute allograft extrusion was 3.61 ± 1.15 mm at 6 weeks postoperatively, 3.81 ± 0.96 mm at 1 year postoperatively, and 4.31 ± 1.53 mm at midterm follow-up (Figure 2, A and B). No significant difference was seen between 6 weeks and 1 year after surgery; however, there was a significant difference between these 2 time points and the midterm period. The mean RPE was 40.4% ± 11.8%, 42.9% ± 10.7%, and 53.7% ± 20.8% at the 6-week, 1-year, and midterm follow-ups, respectively. We found no significant difference between 6 weeks and 1 year after surgery, but RPE was significantly increased at the midterm follow-up compared with both of the earlier follow-up periods (Table 3).

(A) Coronal magnetic resonance imaging (MRI) scan of a 37-year-old male patient at 6 weeks after surgery, showing 2.55 mm of graft extrusion (white arrow). (B) MRI scan at midterm follow-up showing 4.46 mm of graft extrusion in the same patient (red arrow).
Mean Absolute and Relative Coronal Extrusion a
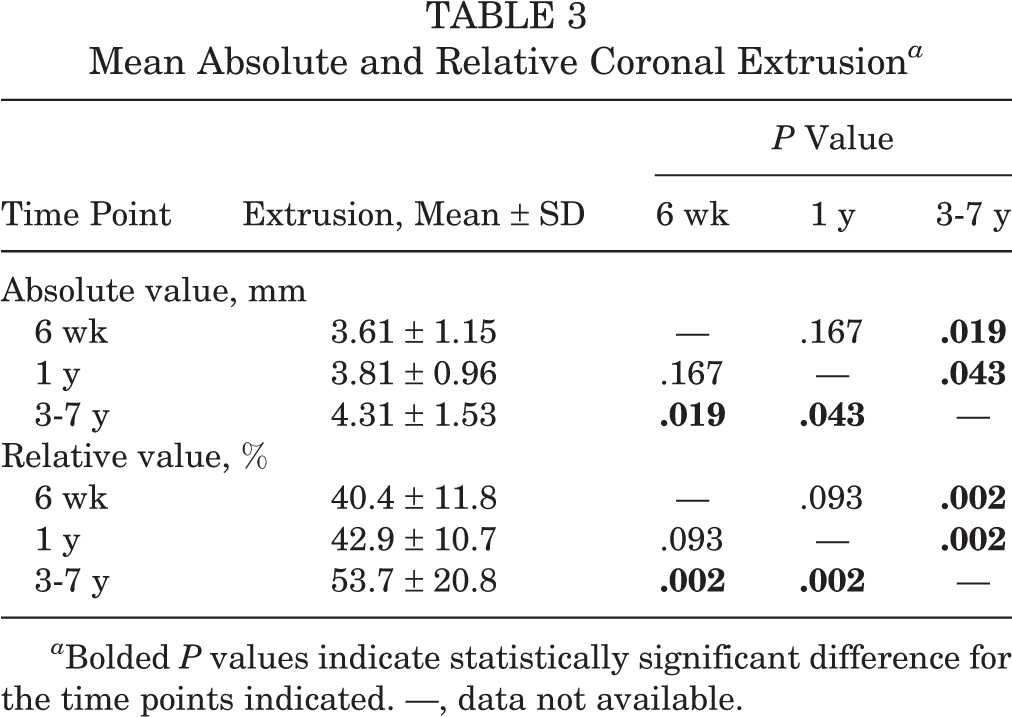
a Bolded P values indicate statistically significant difference for the time points indicated. —, data not available.
Radiologic Allograft Extrusion in the Sagittal Plane
In the sagittal plane, the mean absolute ACMD was 3.48 ± 1.62 mm at 6 weeks postoperatively, 3.93 ± 1.84 mm at 1 year postoperatively, and 4.88 ± 1.96 mm at midterm follow-up. The mean relative ACMD was 36.6% ± 17.6% at 6 weeks postoperatively, 38.8% ± 18.3% at 1 year postoperatively, and 48.1% ± 22.1% at midterm follow-up. No significant difference was noted for either absolute or relative values between 6 weeks and 1 year after surgery, but both increased significantly at the midterm period compared with both of the earlier follow-up periods (Table 4). The mean absolute PCMD was 1.01 ± 2.99 mm, 1.22 ± 2.71 mm, and 2.45 ± 2.84 mm at 6 weeks, 1 year, and midterm follow-up, respectively. At the same time points, the mean relative PCMD was 8.23% ± 21.5%, 10.9% ± 21.2%, and 19.2% ± 22.4%, respectively. The mean absolute PCMD and relative PCMD did not show any significant difference between 6 weeks and 1 year postoperatively but showed a significant increase at midterm follow-up compared with both of the earlier follow-up periods (Table 5).
Mean Absolute and Relative Anterior Cartilage Meniscal Distance a

a Bolded P values indicate statistically significant difference for the time points indicated. ACMD, anterior cartilage meniscal distance; —, data not available.
Mean Absolute and Relative Posterior Cartilage Meniscal Distance a

a Bolded P values indicate statistically significant difference for the time points indicated. PCMD, posterior catilage meniscal distance; —, data not available.
When we divided the patient sample into those with and without anterior cruciate ligament (ACL) reconstruction, we found no significant difference in the degree of allograft extrusion between the 2 groups in both coronal and sagittal planes (P > .05).
JSW and Axial Alignment
The mean JSW on Rosenberg view was 4.42 ± 0.88 mm, 4.30 ± 0.83 mm, and 3.96 ± 1.06 mm at 2 days before surgery, 1 year after surgery, and midterm follow-up, respectively. No significant difference was seen between the preoperative and postoperative 1-year values; however, the mean JSW significantly decreased at midterm follow-up compared with both of the other time points (Table 6). The mean axial alignment was 1.41° ± 2.58° preoperatively and significantly increased to 1.91° ± 3.16° at midterm follow-up (P = .001).
Mean Joint-Space Width on Rosenberg View a
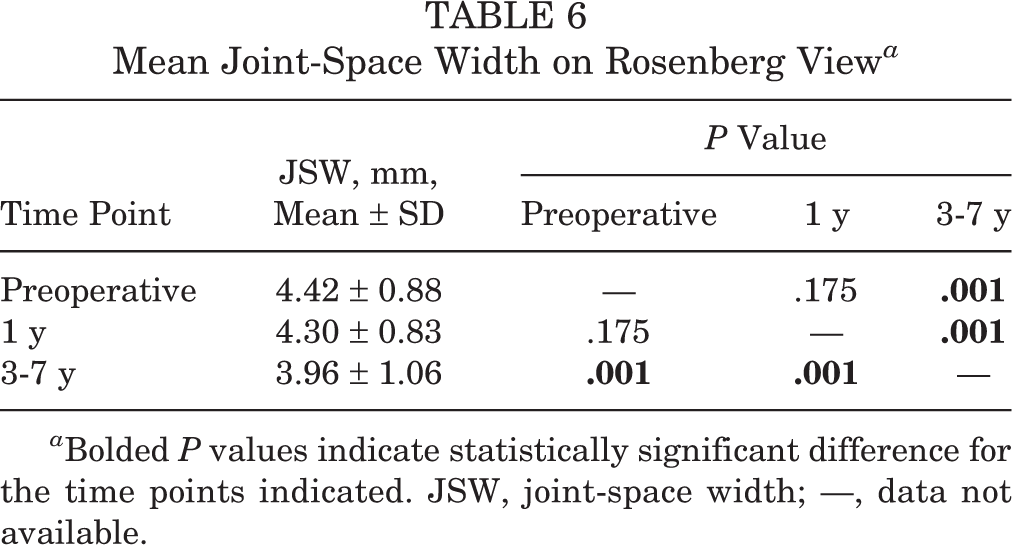
a Bolded P values indicate statistically significant difference for the time points indicated. JSW, joint-space width; —, data not available.
Clinical Outcomes
The mean Lysholm score increased from 65.5 ± 19.4 preoperatively to 88.3 ± 11.2 at 1 year postoperatively and 89.0 ± 10.9 at midterm follow-up. A significant difference was noted between the preoperative and 1-year postoperative scores as well as between the preoperative and midterm scores (Table 7). However, there was no significant difference between 1-year postoperative and midterm scores.
Mean Lysholm Score

a Lysholm scoring (0–100): 95-100 = excellent outcome, 84-94 = good outcome, 65-83 = fair outcome, and <65 = poor outcome. —, data not available.
b Bolded P values indicate statistically significant difference for the time points indicated.
None of the radiographic findings, such as absolute and relative allograft extrusion and the JSW, showed significant correlation with the Lysholm score. In addition, no significant difference was seen in the Lysholm score between the groups with and without ACL reconstruction.
Correlation Between Allograft Extrusion and the Preoperative Axial Alignment
In the coronal plane, the preoperative axial alignment showed a positive correlation with the delta value (calculated by subtracting the 6-week postoperative value from the midterm value) of RPE (r = 0.378; P = .036); however, no significant correlation was found between the preoperative axial alignment and the absolute delta value of coronal extrusion (Figure 3). In the sagittal plane, none of the parameters measured on MRI scans (absolute and relative ACMD and PCMD) were significantly correlated with the preoperative axial alignment.
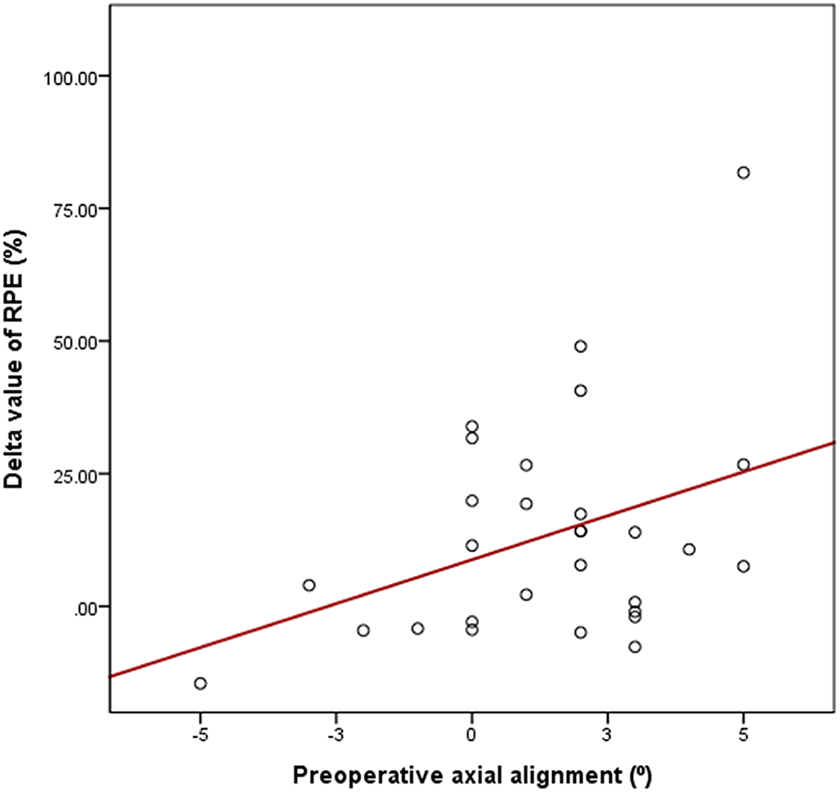
In the coronal plane, the Pearson correlation coefficient (r) between the preoperative axial alignment and the delta value of the relative percentage of extrusion (RPE) was 0.378 (P = .036).
Discussion
This study revealed that allograft extrusion during the midterm follow-up was increased in both the coronal and sagittal planes after MMAT. The absolute value of allograft extrusion and the RPE in the coronal plane did not show any significant difference until 1 year after the operation; however, extrusion progressed in the midterm follow-up period. In the sagittal plane, the mean absolute and relative values of ACMD and PCMD did not progress until 1 year after surgery, but extrusion increased in the midterm follow-up period. The mean JSW did not show a significant decrease until 1 year after surgery but significantly decreased in the midterm follow-up period. When the axial alignment measurements in the preoperative and midterm follow-up periods were compared, the varus alignment was found to be significantly increased. In addition, the degree of varus angulation of the preoperative axial alignment showed a significant correlation with the delta value of RPE in the coronal plane. The Lysholm score was measured preoperatively, 1 year postoperatively, and at midterm follow-up to assess the clinical outcome. The score was significantly increased at 1 year postoperatively and at the midterm follow-up compared with the preoperative value; however, there was no significant difference between 1-year postoperative and midterm follow-up scores. Furthermore, no correlation was found between the Lysholm score and the radiographic findings.
In a previous study, Kim et al 13 studied 46 patients who underwent LMAT via the keyhole technique and examined allograft extrusion during the midterm follow-up period. In that study, midterm was defined as 3 to 5 years, and the mean follow-up period was 51.1 ± 7.1 months. MRI was performed at 6 weeks, 1 year, and midterm follow-up, and extrusion was measured and compared. The investigators found no significant progression of allograft extrusion at midterm follow-up in both the coronal and sagittal planes. This study included only patients who underwent LMAT and did not include patients who underwent MMAT.
In a study by Lee et al 18 that investigated 21 patients who underwent MAT, serial MRI was performed at 6 weeks, 3 months, 6 months, and 12 months after MAT, and the progression of extrusion was analyzed. This study reported that a meniscus that extrudes early remains extruded and does not progressively worsen. Meanwhile, in the absence of early extrusion, extrusion does not increase within 1 year after surgery. This study included very few patients who underwent MMAT (18 LMAT cases and 3 MMAT cases) and analyzed the results only up to 1 year after the operation.
In another study, 68 patients who underwent MMAT were analyzed for the correlation between the horn position on the coronal and sagittal planes and allograft extrusion in the coronal plane. 12 The results showed that position change in the coronal plane affected allograft extrusion more than did changes in the sagittal plane. In addition, the progression of extrusion in the coronal plane was measured at 2 days and 1 year postoperatively. The mean absolute value and the mean RPE did not show any significant difference.
Lee et al, 19 in a study of 51 patients who underwent MMAT and 84 patients who underwent LMAT, compared extrusion in the coronal and sagittal planes on MRI scans at 2 days postoperatively. The amount and incidence of graft extrusion were greater after MMAT than after LMAT in both the coronal and sagittal planes. The investigators suggested several possible reasons including the possibility that MMAT involves a more complex surgical technique and the greater overstuffing of the inherently thicker medial allograft into a restricted joint space.
Although many studies have examined the progression of allograft extrusion, there has been no midterm follow-up study in patients who underwent MMAT. Our study revealed that allograft extrusion in the midterm follow-up period after MMAT was increased in both the coronal and sagittal planes, which was in contrast to the results of a previous study13 on patients who underwent LMAT.
Many factors have been found to be related to allograft extrusion after MAT. For example, in a study of 88 patients who underwent LMAT, Jeon et al 10 analyzed the relationship between osteophyte excision and extrusion at 1-year postoperatively and found that extrusion increased significantly in the nonexcision group. Lee et al 16 reported that increasing the bony trough angle in the axial plane increases the risk of graft extrusion and is associated with nonanatomic lateral placement of the posterior horn. As reported by Kim et al, 12 the anatomic horn position is also related to the progress of extrusion. As described above, various factors have been reported to be associated with allograft extrusion, but there has been no report on the relationship between axial alignment and extrusion.
In the current study, we found that the preoperative axial alignment showed a significant correlation with the delta value of RPE in the coronal plane. Varus malalignment and valgus malalignment have been shown to increase the risk of progression of osteoarthritic changes in the medial and lateral compartments of the knee, respectively, as shown on radiographs. 28 Even in neutrally aligned limbs, the medial compartment bears 60% to 70% of the force across the knee during weightbearing activity. The difference in load bearing between the medial compartment and the lateral compartment is believed to play a role in the prevalence of medial osteoarthritis above the lateral compartment. 1,4,9 In a biomechanical study, Lerner et al 21 found that the first peak medial compartment contact force was changed by 51 N for every 1° of deviation of tibiofemoral alignment. Therefore, as varus malalignment increases, the contact force is further increased in the medial compartment, leading to a subsequent progression of osteoarthritis in the medial compartment. Extrusion of the native meniscus is caused by degenerative changes of the articular cartilage or meniscus. Degeneration of the meniscus damages the integrity of the collagen fibers that make up the meniscus, leading to decreased radial stiffness. 5,6 Therefore, it is considered that the increased contact force and degenerative change of the medial compartment initiated by varus alignment may contribute to extrusion of the allograft.
To observe the progression of joint degeneration, we measured the JSW in this study. The JSW is an indirect indicator of cartilage status and a reproducible index for the evaluation of progressive degenerative changes in the knee joint. 3,23,26 This study showed that degenerative changes in the medial tibiofemoral compartment proceeded after MMAT. Lee et al 20 performed a long-term follow-up study that compared the JSW between extrusion and nonextrusion groups after MAT. Those investigators reported that the JSW was significantly reduced in the extrusion group compared with the nonextrusion group. These results provided indirect evidence that the meniscal allograft has the natural function of the native meniscus and that allograft extrusion after MAT may be associated with degenerative changes of the knee joint. The results of our study may also support these results.
We assessed clinical outcome by calculating the Lysholm score. The Lysholm score is a specific score reflecting knee function and is also suitable for evaluating the treatment outcome of knee joint chondral lesions. Although we had no comparative group, the mean Lysholm score at the final follow-up was 89.0, indicating good results (score, 84-94), despite the increase in allograft extrusion and the decrease in JSW. However, if the degenerative change gradually progresses owing to allograft extrusion, the clinical outcome can be expected to worsen during the long-term follow-up period. Therefore, a long-term study will be needed to clarify the relationship among allograft extrusion, degenerative change, and clinical outcome.
This study has several limitations. First, this was retrospective study with a relatively small sample size (30 patients). However, no previous study has reported on allograft extrusion at midterm follow-up based only on patients who underwent MMAT. Furthermore, this is the first study to analyze the relationship between axial alignment and extrusion. Second, the accuracy in measuring extrusion in the anterior and posterior horns was lower in the sagittal plane than in the coronal plane. This is because of the partial volume effect in which meniscal tissue may overlap with the anterior and posterior margins of the tibial plateau. However, the interobserver and intraobserver reliability measurements showed that our study data had good reliability. Third, of the 87 patients, only 30 patients were included in the study; thus, the exclusion of 57 patients may have created a bias. Fourth, 16 of the 30 patients previously underwent ACL reconstruction surgery, which may have affected the clinical outcomes. Fifth, we did not evaluate functional outcomes, such as Tegner or Marx activity scores, for these patients.
Conclusion
Allograft extrusion did not increase until 1 year after MMAT; however, during the midterm follow-up period, allograft extrusion progressed in both the coronal and sagittal planes. Preoperative axial alignment showed a positive correlation with the allograft extrusion in the coronal plane.
Footnotes
Acknowledgment
The authors acknowledge the language help of Vikas Narang and Editage.
Final revision submitted May 30, 2020; accepted June 16, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Asan Medical Center Institutional Review Board (project No. 2019-0975).