
Abstract
Background:
Studies with a low level of evidence (LOE) have dominated the top cited research in many areas of orthopaedics. The wide range of treatment options for patellar instability necessitates an investigation to determine the types of studies that drive clinical practice.
Purpose:
To determine (1) the top 50 most cited articles on patellar instability and (2) the correlation between the number of citations and LOE or methodological quality.
Study Design:
Cross-sectional study.
Methods:
The Scopus and Web of Science databases were assessed to determine the top 50 most cited articles on patellar instability between 1985 and 2019. Bibliographic information, number of citations, and LOE were collected. Methodological quality was calculated using the Modified Coleman Methodology Score (MCMS) and the Methodological Index for Non-Randomized Studies (MINORS). Mean citations and mean citation density (citations per year) were correlated with LOE, MCMS, and MINORS scores.
Results:
Most studies were cadaveric (n = 10; 20.0%), published in the American Journal of Sports Medicine (n = 13; 26.0%), published between 2000 and 2009 (n = 41; 82.0%), and conducted in the United States (n = 17; 34.0%). The mean number of citations and the citation density were 158.61 ± 59.53 (range, 95.5-400.5) and 12.74 ± 5.12, respectively. The mean MCMS and MINORS scores were 59.62 ± 12.58 and 16.24 ± 3.72, respectively. No correlation was seen between mean number of citations or citation density versus LOE. A significant difference was found in the mean LOE of articles published between 1990 and 1999 (5.0 ± 0) versus those published between 2000 and 2009 (3.12 ± 1.38; P = .03) and between 2010 and 2019 (3.00 ± 1.10; P = .01).
Conclusion:
There was a shift in research from anatomy toward outcomes in patellar instability; however, these articles demonstrated low LOE and methodological quality. Higher quality studies are necessary to establish informed standards of management of patellar instability.
Keywords
Patellar instability is a common cause of disability and pain, 42 affecting between 7 and 43 out of every 100,000 adolescents annually. 21 The cause of patellar instability is multifactorial; thus, the approach to treatment varies widely from nonoperative management to various surgical procedures. 65 Nonoperative treatment options include dynamic strengthening via physical therapy and bracing. In instances of failed nonoperative treatment or recurrent instability, surgery can improve stability and should be tailored toward individual anatomic features and injuries. The vast majority of patients with patellar instability are treated using soft tissue balancing procedures, such as medial patellofemoral ligament (MPFL) reconstruction and lateral lengthening. However, osseous procedures, such as tibial tubercle osteotomy (TTO), may be performed as an adjunctive procedure in cases of malalignment or patella alta. 65 Overall, operative intervention has been shown to result in adequate patient outcomes, satisfaction, and postoperative stability. 16,18,58,63,68,88 Improved knowledge about pathologies involving the patellofemoral joint has been a major driving force for tailored management. 90 With the increase in treatment approaches and research on patellar instability, it is imperative to analyze the types and quality of these investigations to determine the driving factors for current and future clinical practice. As changes in the health care system make physicians and health care systems more responsible for outcomes, the quality of the studies informing clinical decisions and management is critical for evidence-based medicine practice.
In the field of orthopaedics, bibliometric analyses have been conducted for the rotator cuff, 77 the elbow, 39 knee arthroplasty, 84 pediatrics, 8 the spine, 85 and the foot and ankle. 46 Collectively, these analyses have demonstrated that low-level studies are among the top cited research. However, no previous study has assessed the quality and methods of the highly cited literature on patellar instability.
The purpose of this study was to (1) identify the top 50 most cited articles related to patellar instability and (2) determine whether there was a correlation between these articles and the level of evidence (LOE) or their methodological quality. We hypothesized that there would be a weak or insignificant correlation between the top 50 most cited articles on patellar instability and LOE or methodological quality.
Methods
A search of the Scopus and Web of Science databases was performed on April 16, 2019, for articles in English published between 1985 and 2019, using the following Boolean operators and the advanced search function: “patellar instability OR lateral patellar dislocation OR medial patellofemoral ligament OR medial patellofemoral ligament repair OR medial patellofemoral ligament reconstruction OR TTO OR lateral retinacular release OR MPFL OR TTO OR proximal medial patellar restraints OR trochlear dysplasia OR trochleoplasty OR patellofemoral instability OR medial quadriceps tendon femoral ligament OR MPTFL OR medial patellofemoral complex OR Fulkerson osteotomy OR anteromedialization osteotomy OR Elmslie Trillat OR Hauser OR Maquet NOT osteoarthritis NOT arthroplasty NOT replacement.”
The search results were then filtered in descending order by number of citations. The number of citations was averaged from each database to determine the top 50 most cited articles on patellar instability according to both databases. All article titles that were relevant to the search criteria were included. Articles that were not present in both databases were excluded. Abstracts for each article were then evaluated for relevance to patellar instability and its related topics, and the top 50 relevant articles were selected.
Data Extraction
The following characteristics for each article were recorded: title, author(s), journal, publication information, country of origin, and study type. The citation density for each article was calculated by dividing the average number of citations by the number of years the article had been published to account for the possibility that older articles would have more citations simply based on years of publication. The LOE of each clinical article was recorded based on the guidelines established by the Journal of Bone and Joint Surgery (American Volume) (JBJS) 38 ; anatomic/cadaveric and basic science biomechanics research articles were assigned an LOE of 5 for the purposes of this investigation. It is important to note that LOE was designed for and is applicable to clinical studies despite the method of this investigation. 87 Additionally, the method of each article was evaluated based on 2 recent scoring systems for methodological quality: the Modified Coleman Methodology Score (MCMS) 64 and the Methodological Index for Non-Randomized Studies (MINORS). 75 Both the MCMS and the MINORS criteria were used, as both metrics were implemented in previous assessments of top papers in orthopaedics. 35,39,77 Furthermore, the MINORS questionnaire tends to favor nonrandomized controlled trials, whereas the MCMS questionnaire favors randomized controlled trials 39,77 ; therefore, both metrics were implemented in this investigation. Scores were calculated by 2 authors separately (A.A. and K.Y.), and consensus was reached when discrepancies arose. Scores were not calculated for cadaveric, review, or technique studies.
Statistical Analysis
The data were assessed for a normal distribution using a Kolmogorov-Smirnov test. Based on the results, the Spearman rank coefficient (R S) was used to determine the degree of correlation if the data did not follow a normal distribution. Otherwise, the Pearson correlation coefficient (R) was used to determine the degree of correlation if the data were normally distributed. The strength of correlation for both tests was defined as shown in Table 1. Statistical analysis was performed using Microsoft Excel version 16.45 (Microsoft Corp). Two-group comparisons were analyzed using the Student t test. A value of P < .05 was defined for the level of significance.
Classification of Correlation Strength for the Pearson Correlation Coefficient (R) and Spearman Rank Coefficient (R S)

Results
The top 50 most cited articles on patellar instability between 1985 and 2019 are shown in Appendix Table A1. The mean ± SD number of citations was 158.61 ± 59.53 (range, 95.5-400.5) and the mean citation density was 12.74 ± 5.12. The distribution of citation density by publication year is provided in Figure 1. A total of 15 different journals were represented, with the top 3 most cited journals being the American Journal of Sports Medicine (n = 13; 26.0%), Arthroscopy (n = 8; 16.0%), and Knee Surgery, Sports Traumatology, Arthroscopy (n = 5; 10.0%) (Figure 2). In total, 13 different countries contributed to the top 50 articles, with the United States (n = 17; 34.0%), Japan (n = 8; 16.0%), Switzerland (n = 4; 8.0%), and Germany (n = 4; 8.0%) contributing the most articles (Figure 3). A significant difference (P = .01) was seen in the mean number of citations in articles from the United States (n = 17; 87.24 ± 79.37) compared with articles from outside of the United States (n = 33; 143.86 ± 40.23). As well, a significant difference (P = .03) was noted in the citation density in articles from the United States (n = 17; 14.88 ± 6.73) versus those outside of the United States (n = 33; 11.64 ± 3.69).
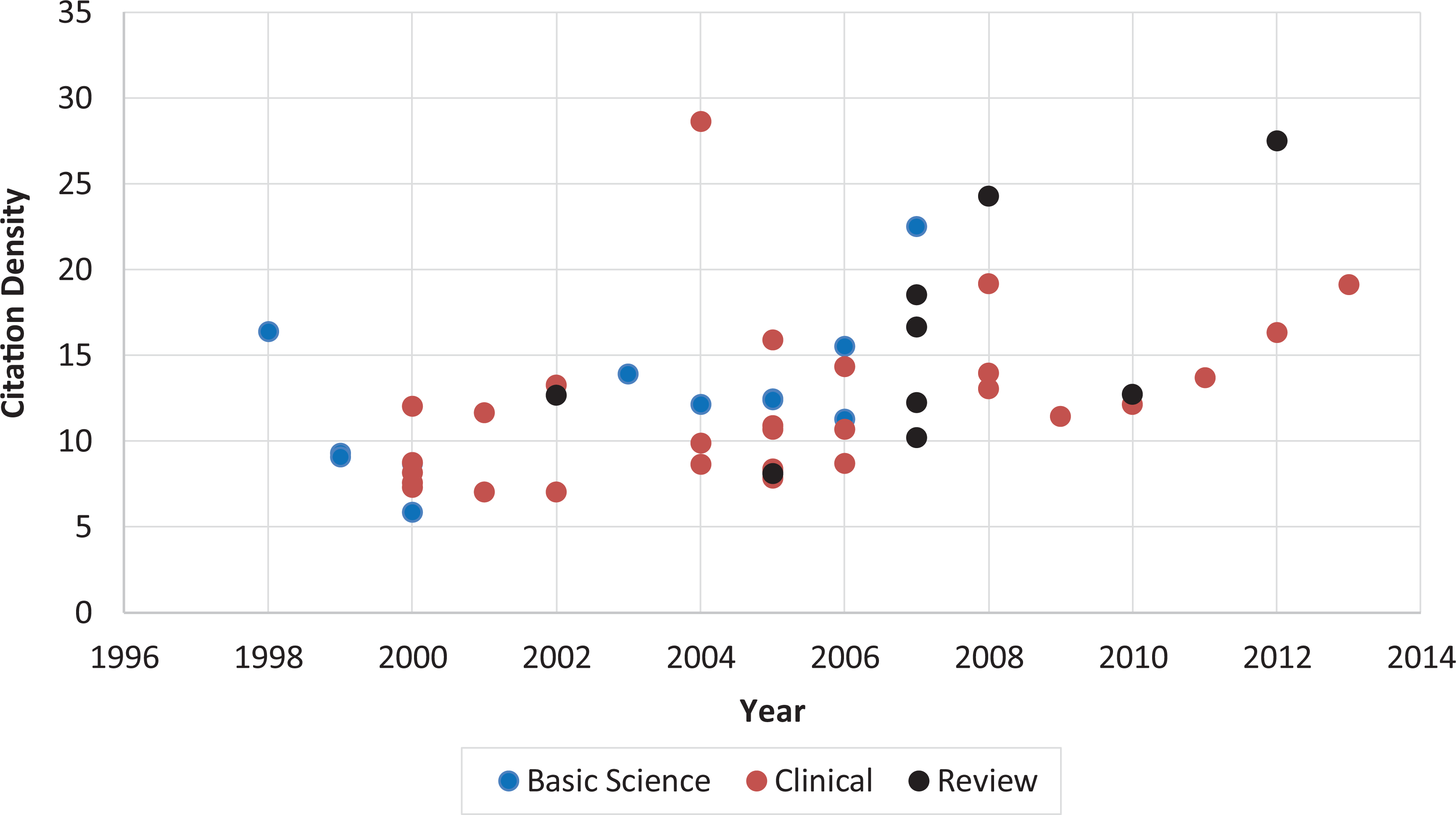
Distribution of citation density by year, stratified by study type.

Distribution of the top 50 most cited articles by journal of publication.
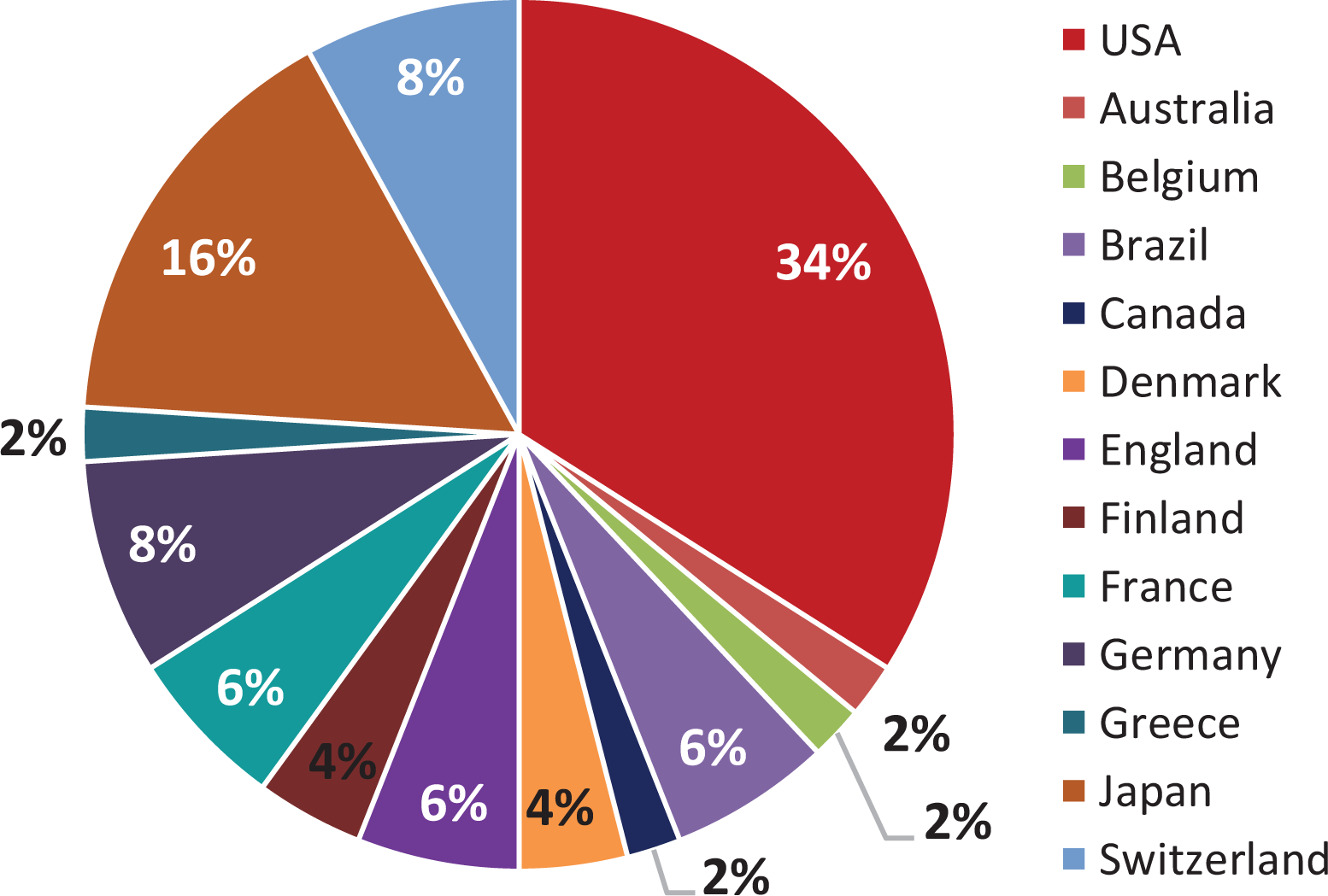
Distribution of the top 50 most cited articles by country of origin.
The most common types of article were cadaveric studies (n = 10; 20.0%), followed by review articles (n = 9; 18.0%) and prospective cohort studies (n = 8; 16.0%) (Figure 4). The overall mean LOE for all 50 articles was 3.28 ± 1.37, with investigations assigned an LOE of 5 being the most prevalent (n = 13; 26.0%) (Figure 5). After exclusion of anatomic studies and review articles, the average LOE was 2.6 ± 1.1. The majority of articles were published between 2000 and 2009 (n = 41; 82.0%) (Figure 6), with the most articles being published in 2005 (n = 9; 18.0%). The most prevalent topics were related to MPFL reconstruction (n = 19; 38%) and anatomic studies of the MPFL and surrounding structures (n = 13; 26%). A breakdown of topic by decade is shown in Table 2.

Distribution of the top 50 most cited articles by study design. RCT, randomized controlled trial.

Distribution of the top 50 most cited articles by level of evidence (LOE) for clinical studies (according to the guidelines established in the Journal of Bone and Joint Surgery [American Volume] 38 ); anatomic/cadaveric and basic science biomechanics research articles were assigned an LOE of 5 for the purposes of this investigation. LOE was initially designed for clinical studies, as described by Wright et al 87 ; however, in this investigation, cadaveric and biomechanical studies were assigned an LOE of 5.
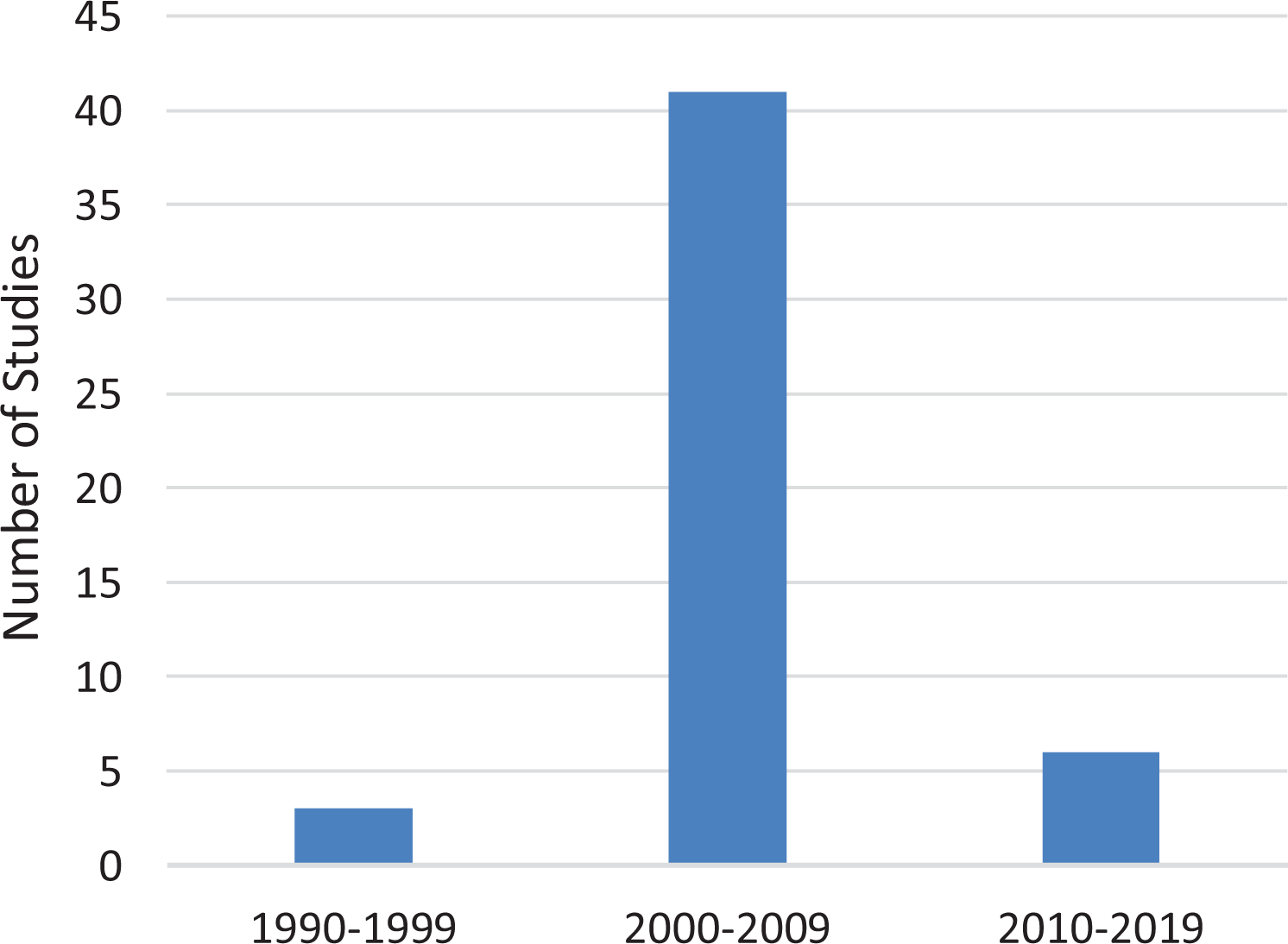
Distribution of the top 50 most cited articles by decade of publication.
Distribution of Patellar Instability Research Topics a

a Values are expressed as n (%). MPFL, medial patellofemoral ligament.
When analyzing methodological quality, we excluded 10 cadaveric studies, 9 review articles, 1 anatomic study, and 1 controlled laboratory study (n = 21; 42% excluded). From the remaining articles (n = 29), the overall mean MCMS and MINORS scores were 59.62 ± 12.58 and 16.24 ± 3.72, respectively. We found no significant difference between articles published in the United States versus outside the United States with regard to MCMS (57.57 ± 7.93 vs 60.27 ± 13.82, respectively; P = .63) and MINORS scores (15.15 ± 2.97 vs 16.59 ± 3.92, respectively; P = .38).
We found no correlation between mean number of citations or citation density versus LOE (R S = –0.035; P = .855 and R S = –0.117; P = .546, respectively) or MCMS scores (R S = –0.058; P = .763 and R S = 0.171; P = .375, respectively). A weak negative correlation existed for mean citations versus MINORS scores (R S = –0.385; P = .039). However, no correlation was noted between citation density and MINORS scores (R S = 0.020; P = .920).
When analyzing the trends in methodological quality over time, we noted a significant difference in the mean LOE of articles published between 1990 and 1999 (5 ± 0) versus those published between 2000 and 2009 (3.12 ± 1.38) (P = .03). There was a statistical significant difference between level of evidence between 1990 and 1999 versus 2010 and 2019 (P = .01). However, no significant difference (P = .74) was found in the mean LOE in articles published between 2000 and 2009 (3.20 ± 1.38) and between 2010 and 2019 (3.00 ± 1.10). In articles published between 2000 and 2009 and between 2010 and 2019, no significant difference was seen in the MCMS (60.24 ± 12.88 vs 55.5 ± 11.21, respectively; P = .52) or MINORS scores (15.76 ± 3.70 vs 19.25 ± 2.36, respectively; P = .81). No methodological scores were available for analysis for articles published between 1990 and 1999 due to study type.
Discussion
This investigation identified the top 50 most cited articles on patellar instability and found no significant relationship between the number of citations and the quality of the study based on 2 separate indices for assessing study method. The top 50 most cited articles on patellar instability were of low-level evidence and had low methodological assessment scores based on 2 different scoring methods. The most cited article among the list, that by Fithian et al, 34 was published in 2004 and had an average citation number of 400.5. This high citation number likely is attributable to the importance of this article in the history of knowledge about epidemiology and risk factors associated with patellar instability. The most common studies were cadaveric (LOE, 5), were published in the American Journal of Sports Medicine between 2000 and 2009, and were conducted in the United States. The most frequently discussed topics were MPFL reconstruction and anatomic analyses of the patellar stabilizers. Furthermore, between 2000 and 2009, there was a shift in study topics from the complex anatomic characteristic of the major patellar stabilizers toward outcomes from management of patellar instability. As the number of publications on patellar instability continues to proliferate, it is imperative to assess the quality of investigations that guide diagnosis and management of patellar instability.
Researchers and journals are consistently assessed based upon their level of effect. The journal impact factor (JIF) is often used as a marker of the quality of a journal. The JIF is calculated by the total number of citations for articles in a given journal divided by the number of articles published in that journal over the 2 years before the calculation 13 and, therefore, does not account for information, such as mean citation of individual articles and the possibility of a few articles with a large number of citations. As a result, the JIF can be significantly affected by a skewed citation distribution and by the variability in citation rates across research fields. 13 This is a significant consideration for orthopaedic surgeons, as the JIF is a key marker for finding research that influences their clinical decision making. 27 Similar to the JIF, citation counts are often used to evaluate articles but may not be an accurate marker of study quality. Although an alternative tool for screening research quality has yet to be elucidated, researchers should take into account study methods when referencing other studies to increase the effect of their findings.
Although no previous bibliometric reviews exist for patellofemoral injuries, the results of this investigation are comparable with previous bibliometric analyses in subspecialties of orthopaedics. Similar to trends found in research of anterior cruciate ligament, knee arthroplasty, and ulnar collateral ligament surgery, the most represented country among the top 50 most cited papers on patellar instability was the United States (34%). 37,39,84 This trend supports the fact that the United States continues to be a global leader in research output. 43 However, this finding may be subject to bias, as many journals are written in the English language and are based in the United States. Furthermore, Okike et al 56,57 demonstrated that investigations performed in the United States or Canada, studies that accurately reported conflict of interests, or studies that were authored by an individual with >10 publications in frequently cited orthopaedic journals were more likely to be published in JBJS. Furthermore, author details, such as country of origin, rather than study quality or details were prognostic of eventual publication in a journal after rejection from JBJS. 57 Cadaveric studies were the most prevalent type of study in this report, differing from previous bibliometric analyses in orthopaedic surgery, which tend to have more case series and outcome studies. 2,37,43,77,84 It is possible that cadaveric studies may have been more prevalent in this study due to the relative infancy of patellar instability research and management in comparison with other orthopaedic procedures. Hence, initial interest in this area is expected to begin with cadaveric and anatomic studies before proceeding to live participants and case studies. Furthermore, the statistical difference in LOE from 1990-1999 to 2000-2009 and 2010-2019 was likely due to the preponderance of anatomic and cadaveric studies that were initially performed, which we included as investigations with an LOE of 5 for this study.
The field of patellofemoral instability has changed tremendously over the past 2 decades. Before 2000, the standard of care for treatment of recurrent instability was either medial imbrication or TTO with medial imbrication. Since its inception, MPFL reconstruction has become the gold standard in the treatment of recurrent instability. Research has evolved over time from defining anatomic structures to using biomechanical studies to evaluate MPFL surgical techniques. Elias and Cosgarea 31 identified the importance of appropriate graft tensioning and lengthening to reduce contact pressure on patellofemoral cartilage. Furthermore, Schöttle et al 71 aided in the establishment of radiographic landmarks for controlled intraoperative femoral MPFL insertion, commonly known as the Schöttle point. As the anatomic and biomechanical characteristics have become well-described, research on patellar instability has shifted toward clinical outcomes. Early clinical investigations had small sample sizes and were retrospective in nature, which contributed to the low LOE. Eventually, Fithian et al 34 published a large clinical series that helped define surgical indications and descriptive epidemiological characteristics of patients who were at risk for patellar dislocation. However, this investigation was limited by including all patients with acute patellar dislocation and was unable to stratify specific populations who were at risk. Eventually, predictive models of recurrent instability identified that young patients with trochlear dysplasia were at the highest risk for recurrent instability. 40,44 As research into patellofemoral instability has continued to evolve, there has been a statistically significant increase in the number of patients who have undergone operative treatment for patellar instability between 2005 and 2016. 71 Furthermore, Stupay et al 82 demonstrated that many more medical centers and physicians were performing MPFL reconstruction after 2010 with good functional outcomes and a lower rate of complications and failures than when the procedure was introduced.
Several randomized controlled trials have compared nonoperative treatment versus surgical intervention in patients with first-time dislocations. 10,59,74 Despite being of high-level evidence, these investigations were limited because they assessed patients as a collective group and did not specifically assess patients who are at the highest risk of patellar dislocations. Prospective randomized controlled trials that assess modern, standard of care treatments (MPFL reconstruction) in the highest risk population (young patients with trochlear dysplasia) will have clinical effect by elucidating the optimal treatment plan in patients with patellar dislocations. Nonetheless, there are limitations to performing randomized clinical trials due to strict regulations and high costs. 12,48,89 However, patellar instability further compounds this issue with its increased variability in indications, concomitant procedures, and postoperative rehabilitation. It becomes increasingly difficult and onerous to adequately perform a high-level investigation with many confounding variables.
In an effort to standardize the approach to the diagnosis and management of patellar instability, the Orthopaedic Journal of Sports Medicine and the Patellofemoral Foundation released a consensus statement on the approach to patellar instability; these recommendations were based on the experience of 16 recognized experts and their understanding of the medical literature and principles of biomechanics, anatomy, and patient care. 62 Although these guidelines help standardize a treatment algorithm, these recommendations should be further substantiated by evidence from high-level investigations. The establishment of new guidelines must also take into consideration cost and efficiency, as these factors are important to maintain adherence to such changes. 28 Although the consensus statement was a strong start to a more standardized approach to patellar instability, further high-level research is required to substantiate these recommendations and implement them in clinical practice. In an effort to provide higher level evidence, systematic reviews and meta-analyses are commonly performed to increase sample sizes and provide a summary of clinical outcomes. However, systematic reviews and meta-analyses can only be as effective as the quality of investigations they include. In order to improve the quality of these investigations, we should aim to have a minimum criterion of data required for a field. Justifying Patellar Instability Treatment by Early Results is a multicenter registry that was founded in 2017 with the purpose of establishing clinical guidelines in the management of patellar instability. 41,73
Limitations
The results of this investigation must be interpreted within the context of its limitations. Our sample size was arbitrarily selected at 50 articles, and this investigation could have been repeated using a larger sample size. Basic science and cadaveric studies were assigned an LOE of 5 in this investigation, which decreased the overall LOE. This may inhibit interpretation of the trend of study type and quality over time. This investigation may have benefited from assessing only clinical investigations or increasing the number of studies in this analysis to understand the change in patellofemoral research over time. Furthermore, inclusion of anatomic studies biased the finding that there was no correlation between LOE and the top 50 papers due to the number of anatomic investigations (n = 21) and their low LOE. Therefore, this finding must be interpreted with caution. Because of the high number of cadaveric and review articles that were included in the final group, only 29 studies could be assessed for methodological quality. Additionally, our study took into consideration only the search results from Scopus and Web of Science. Scopus is the largest database in the world, and many of our articles that were in the top 50 from Scopus were not listed in Web of Science and therefore were not included in this analysis. Another limitation to our study is the subjectivity of some of the items on the methodological grading scales. Phrases, such as “well-described” rehabilitation protocol versus “described without complete detail,” in the MCMS scoring rubric left room for subjective variability. 64 This was also evident in the MINORS scale, where criteria, such as “a clearly stated aim,” were used to assess techniques. 75 This could result in the quality of a publication’s being interpreted differently by various investigators. To minimize this bias, 2 investigators were responsible for independently scoring all of the articles using both scales, and a consensus was achieved when discrepancies in scoring were discovered.
Conclusion
There was a shift in research from anatomy toward outcomes in patellar instability; however, these articles demonstrated low LOE and methodological quality. Higher quality studies are necessary to establish informed standards of management of patellar instability.
Footnotes
Final revision submitted May 30, 2020; accepted June 23, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.L.S. has received research support from Arthrex; grant support from DJO; educational support from Elite Orthopedics and Vericel; consulting fees from Arthrex, Ceterix, Conmed Linvatec, Flexion Therapeutics, GLG Consulting, JRF Ortho, Moximed, Olympus, RTI Surgical, and Vericel; and royalties from RTI Surgical. J.F. has received research support from Active Implants, Arthrex, Episurf, Fidia, JRF Ortho, Novartis, Organogenesis, Samumed, Vericel, and Zimmer Biomet; educational support from Crossroads Orthopedics and Vericel; consulting fees from Aesculap/B.Braun, Arthrex, Cartiheal, Cook Biotech, DePuy, Exactech, Moximed, Organogenesis, Regentis, RTI Surgical, Samumed, Zimmer Biomet, and ZKR Orthopedics; speaking fees from Arthrex, DePuy, Organogenesis, and Vericel; and royalties from Biopoly, Organogenesis, Springer, and Thieme and has stock or stock options in MedShape and Ortho Regenerative Tech. B.E.S.S. has received consulting fees, speaking fees, and royalties from Arthrex. N.H.A. has received research support from Arthrex, Pacira, Stryker, Trice Medical, and Zimmer; educational support from Arthrex; consulting fees from DePuy/Medical Device Business Services, Flexion, Pacira, Smith & Nephew, and Trice Medical; speaking fees from DePuy, Flexion, Pacira, Smith & Nephew, Trice Medical, and Zimmer; honoraria from Fidia Pharma; hospitality payments from Novadaq; and royalties from Smith & Nephew. J.N.L. has received educational support from Arthrex and Smith & Nephew, speaking fees from Smith & Nephew, and hospitality payments from Exactech. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Appendix
The Top 50 Most Cited Articles on Patellar Instability, 1985-2019 a

| Rank | Title | Lead Author | Year | Study Design | Average Citations | Citation Density | LOE | MCMS | MINORS |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Epidemiology and natural history of acute patellar dislocation | Fithian 34 | 2004 | Prosp cohort | 400.5 | 28.61 | 2 | 63 | 16 |
| 2 | Medial soft tissue restraints in lateral patellar instability and repair | Hautamaa 36 | 1998 | Cadaveric | 328 | 16.40 | 5 | NA | NA |
| 3 | Radiographic landmarks for femoral tunnel placement in medial patellofemoral ligament reconstruction | Schöttle 71 | 2007 | Cadaveric | 247.5 | 22.50 | 5 | NA | NA |
| 4 | Patellar instability | Colvin 22 | 2008 | Review | 243 | 24.3 | 3 | NA | NA |
| 5 | Characteristics of patients with primary acute lateral patellar dislocation and their recovery within the first 6 months of injury | Atkin 5 | 2000 | Prosp cohort | 216.5 | 12.03 | 1 | 61 | 16 |
| 6 | Acute lateral patellar dislocation at MR imaging: injury patterns of medial patellar soft tissue restraints and osteochondral injuries of the inferomedial patella | Elias 30 | 2002 | Case-control | 212.5 | 13.28 | 3 | 57 | 15 |
| 7 | Osteotomies in patellofemoral instabilities | Dejour 25 | 2007 | Review | 204 | 18.55 | 4 | NA | NA |
| 8 | Clinical and radiological outcome of medial patellofemoral ligament reconstruction with a semitendinosus autograft for patellar instability | Schöttle 70 | 2005 | Retrosp cohort | 206.5 | 15.88 | 2 | 60 | 14 |
| 9 | The anatomy and reconstruction of the medial patellofemoral ligament | Smirk 76 | 2003 | Cadaveric | 208.5 | 13.90 | 5 | NA | NA |
| 10 | Current concepts of lateral patellar dislocation | Arendt 4 | 2002 | Review | 203 | 12.69 | 4 | NA | NA |
| 11 | Results of medial patellofemoral ligament reconstruction in the treatment of patellar dislocation | Drez 29 | 2001 | Case series | 198 | 11.65 | 4 | 67 | 11 |
| 12 | Quantitative study of the quadriceps muscles and trochlear groove geometry related to instability of the patellofemoral joint | Farahmand 33 | 1998 | Cadaveric | 186 | 9.30 | 5 | NA | NA |
| 13 | Acute patellar dislocation in children and adolescents: a randomized clinical trial | Palmu 59 | 2008 | RCT | 191.5 | 19.15 | 1 | 63 | 18 |
| 14 | Technical errors during medial patellofemoral ligament reconstruction could overload medial patellofemoral cartilage—a computational analysis | Elias 31 | 2006 | Lab | 186.5 | 15.54 | 2 | NA | NA |
| 15 | Medial patellofemoral ligament reconstruction in patients with lateral patellar instability and trochlear dysplasia | Steiner 81 | 2006 | Case series | 172 | 14.33 | 4 | 58 | 18 |
| 16 | The anatomy and isometry of the medial patellofemoral ligament—implications for reconstruction | Steensen 79 | 2004 | Cadaveric | 170 | 12.14 | 5 | NA | NA |
| 17 | First-time traumatic patellar dislocation—a systematic review | Stefancin 80 | 2007 | Review | 183 | 16.64 | 2 | NA | NA |
| 18 | Classification of lesions of the medial patellofemoral ligament in patellar dislocation | Nomura 50 | 1999 | Anatomic | 172.5 | 9.08 | 5 | NA | NA |
| 19 | Medial patellofemoral ligament restraint in lateral patellar translation and reconstruction | Nomura 53 | 2000 | Cadaveric | 156.5 | 8.69 | 5 | NA | NA |
| 20 | Tensile strength of the medial patellofemoral ligament before and after repair or reconstruction | Mountney 47 | 2005 | Cadaveric | 162 | 12.46 | 5 | NA | NA |
| 21 | Anatomical analysis of the medial patellofemoral ligament of the knee, especially the femoral attachment | Nomura 55 | 2005 | Cadaveric | 161.5 | 12.42 | 5 | NA | NA |
| 22 | Immediate surgical repair of the medial patellar stabilizers for acute patellar dislocation—a review of eight cases | Ahmad 1 | 2000 | Case series | 157.5 | 8.75 | 4 | 60 | 11 |
| 23 | Femoral trochlear dysplasia: MR findings | Pfirrmann 61 | 2000 | Case-control | 147 | 8.17 | 3 | 45 | 20 |
| 24 | Operative treatment of primary patellar dislocation does not improve medium-term outcome—a 7-year follow-up report and risk analysis of 127 randomized patients | Nikku 49 | 2005 | RCT | 141.5 | 10.88 | 1 | 68 | 19 |
| 25 | Patellar instability: assessment on MR images by measuring the lateral trochlear inclination---initial experience | Carrillon 17 | 2000 | Case-control | 136 | 7.56 | 3 | 35 | 19 |
| 26 | Reconstruction of the medial patellofemoral ligament with gracilis tendon autograft in transverse patellar drill holes | Christiansen 19 | 2008 | Case series | 139.5 | 13.95 | 4 | 43 | 6 |
| 27 | A long-term follow-up study after medial patellofemoral ligament reconstruction using the transferred semitendinosus tendon for patellar dislocation | Deie 23 | 2005 | Prosp cohort | 139 | 10.69 | 2 | 76 | 13 |
| 28 | Isolated repair of the medial patellofemoral ligament in primary dislocation of the patella: a prospective randomized study | Christiansen 20 | 2008 | RCT | 130.5 | 13.05 | 1 | 76 | 21 |
| 29 | Cadaveric study on static medial patellar stabilizers: the dynamizing role of the vastus medialis obliquus on medial patellofemoral ligament | Panagiotopoulos 60 | 2006 | Cadaveric | 135 | 11.25 | 5 | NA | NA |
| 30 | Medial patellofemoral ligament reconstruction with semitendinosus autograft for chronic patellar instability: a follow-up study | Ellera Gomes 32 | 2004 | Prosp cohort | 138.5 | 9.89 | 4 | 56 | 10 |
| 31 | Current concepts review—the medial patellofemoral ligament | Bicos 9 | 2007 | Review | 134.5 | 12.23 | 3 | NA | NA |
| 32 | A mid-term follow-up of medial patellofemoral ligament reconstruction using an artificial ligament for recurrent patellar dislocation | Nomura 52 | 2000 | Prosp cohort | 131.5 | 7.31 | 2 | 40 | 15 |
| 33 | Trochleaplasty for recurrent patellar dislocation in association with trochlear dysplasia—a 4- to 14-year follow-up study | von Knoch 86 | 2006 | Retrosp cohort | 128 | 10.67 | 2 | 66 | 17 |
| 34 | Reconstruction of the medial patellofemoral ligament for the treatment of habitual or recurrent dislocation of the patella in children | Deie 24 | 2003 | Retrosp cohort | 129.5 | 8.63 | 2 | 48 | 13 |
| 35 | Medial patellofemoral ligament injury following acute transient dislocation of the patella: MR findings with surgical correlation in 14 patients | Sanders 66 | 2001 | Retrosp cohort | 119.5 | 7.03 | 3 | 50 | 18 |
| 36 | Acute traumatic primary patellar dislocation—long-term results comparing conservative and surgical treatment | Buchner 14 | 2005 | Retrosp cohort | 109 | 8.38 | 3 | 75 | 20 |
| 37 | Correlation of MR imaging findings and open exploration of medial patellofemoral ligament injuries in acute patellar dislocations | Nomura 51 | 2002 | Retrosp cohort | 112.5 | 7.03 | 3 | 43 | 18 |
| 38 | Current concepts on anatomy and biomechanics of patellar stability | Amis 3 | 2007 | Review | 112 | 10.18 | 5 | NA | NA |
| 39 | Trochleaplasty for patellar instability due to trochlear dysplasia—a minimum 2-year clinical and radiological follow-up of 19 knees | Schöttle 69 | 2005 | Prosp cohort | 107 | 8.23 | 1 | 78 | 18 |
| 40 | Conservative versus surgical treatment for repair of the medial patellofemoral ligament in acute dislocations of the patella | Camanho 15 | 2009 | RCT | 103 | 11.44 | 2 | 83 | 20 |
| 41 | The effect of reconstruction of the medial patellofemoral ligament on patellar tracking | Sandmeier 67 | 2000 | Cadaveric | 105 | 5.83 | 5 | NA | NA |
| 42 | The sulcus deepening trochleoplasty—the Lyon’s procedure | Dejour 26 | 2010 | Review | 102 | 12.75 | 4 | NA | NA |
| 43 | Trochleoplasty in dysplastic knee trochlea | Verdonk 83 | 2005 | Prosp cohort | 102 | 7.85 | 2 | 70 | 14 |
| 44 | Magnetic resonance imaging characteristics of the medial patellofemoral ligament lesion in acute lateral patellar dislocations considering trochlear dysplasia, patella alta, and tibial tuberosity-trochlear groove distance | Balcarek 6 | 2010 | Case-control | 97 | 12.13 | 4 | 54 | 21 |
| 45 | Hybrid MPFL reconstruction using the semitendinous tendon for recurrent patellar dislocation: minimum 3 years’ follow-up | Nomura 54 | 2006 | Case series | 104 | 8.67 | 4 | 65 | 14 |
| 46 | A simple technique for reconstruction of the medial patellofemoral ligament using a quadriceps tendon graft | Steensen 78 | 2005 | Review | 105.5 | 8.12 | 5 | NA | NA |
| 47 | Value of the tibial tuberosity |
Balcarek 7 | 2011 | Case-control | 96 | 13.71 | 3 | 54 | 21 |
| 48 | A systematic review of complications and failures associated with medial patellofemoral ligament reconstruction for recurrent patellar dislocation | Shah 72 | 2012 | Review | 165 | 27.50 | 3 | NA | NA |
| 49 | Traumatic patellar dislocation nonoperative treatment compared with MPFL reconstruction using patellar tendon | Bitar 11 | 2012 | RCT | 98 | 16.33 | 1 | 71 | 19 |
| 50 | Predictors of recurrent instability after acute patellofemoral dislocation in pediatric and adolescent patients | Lewallen 45 | 2013 | Case-control | 95.5 | 19.10 | 3 | 44 | 16 |
a Prosp, prospective; Retrosp, retrospective; Lab, controlled laboratory study; LOE, level of evidence; MCMS, Modified Coleman Methodology Score; MINORS, Methodological Index for Non-Randomized Studies; MPFL, medial patellofemoral ligament; MR, magnetic resonance; NA, not applicable; RCT, randomized controlled trial.