
Abstract
Background:
Return to sport (RTS) after osteochondral allograft (OCA) transplantation for large unipolar femoral condyle defects has been consistent, but many athletes are affected by more severe lesions.
Purpose:
To examine outcomes for athletes who have undergone large single-surface, multisurface, or bipolar shell OCA transplantation in the knee.
Study Design:
Case series; Level of evidence, 4.
Methods:
Data from a prospective OCA transplantation registry were assessed for athletes who underwent knee transplantation for the first time (primary transplant) between June 2015 and March 2018 for injury or overuse-related articular defects. Inclusion criteria were preinjury Tegner level ≥5 and documented type and level of sport (or elite unit active military duty); in addition, patients were required to have a minimum of 1-year follow-up outcomes, including RTS data. Patient characteristics, surgery type, Tegner level, RTS, patient-reported outcome measures (PROMs), compliance with rehabilitation, revisions, and failures were assessed and compared for statistically significant differences.
Results:
There were 37 included athletes (mean age, 34 years; range, 15-69 years; mean body mass index, 26.2 kg/m2; range, 18-35 kg/m2) who underwent large single-surface (n = 17), multisurface (n = 4), or bipolar (n = 16) OCA transplantation. The highest preinjury median Tegner level was 9 (mean, 7.9 ± 1.7; range, 5-10). At the final follow-up, 25 patients (68%) had returned to sport; 17 (68%) returned to the same or higher level of sport compared with the highest preinjury level. The median time to RTS was 16 months (range, 7-26 months). Elite unit military, competitive collegiate, and competitive high school athletes returned at a significantly higher proportion (P < .046) than did recreational athletes. For all patients, the Tegner level at the final follow-up (median, 6; mean, 6.1 ± 2.7; range, 1-10) was significantly lower than that at the highest preinjury level (P = .007). PROMs were significantly improved at the final follow-up compared with preoperative levels and reached or exceeded clinically meaningful differences. OCA revisions were performed in 2 patients (5%), and failures requiring total knee arthroplasty occurred in 2 patients (5%), all of whom were recreational athletes. Noncompliance was documented in 4 athletes (11%) and was 15.5 times more likely (P = .049) to be associated with failure or a need for revision than for compliant patients.
Conclusion:
Large single-surface, multisurface, or bipolar shell OCA knee transplantations in athletes resulted in two-thirds of these patients returning to sport at 16 to 24 months after transplantation. Combined, the revision and failure rates were 10%; thus, 90% of patients were considered to have successful 2- to 4-year outcomes with significant improvements in pain and function, even when patients did not RTS.
Osteochondral allograft (OCA) transplantation in the knee has been reported to enable between 75% and 88% of athletes to return to sport (RTS), including between 75% and 82% who returned to preinjury levels. 4,8 However, rates of RTS after OCA transplantation in the knee have been critically examined for only unipolar focal cylindrical, or “plug,” grafts for femoral condylar lesions. While outcomes for these articular defects in athletes are important to examine and the results compare favorably with those for other treatment options, 3,8 many athletes are affected by more severe lesions that are not amenable to unipolar plug grafts. 4,13 The athletes with more severe lesions have not had consistently successful RTS outcomes after other cartilage repair or restoration treatments, such as debridement, abrasion arthroplasty, marrow stimulation procedures, or cell-based therapies. 3,4,8,11,18 Furthermore, patients in this cohort who desire to RTS are not considered suitable candidates for unicompartmental knee arthroplasty (UKA) or total knee arthroplasty (TKA). 1,6,7,10,16,17
OCA transplantation is a treatment option for active patients with large chondral and osteochondral defects in the knee with survival rates as high as 84% to 93% at 10 to 15 years postsurgically. 5 However, historically, OCA transplantation for the treatment of multisurface and bipolar defects in the knee has not been associated with consistently high success rates. 2,5,12,13 Risk factors for poor outcomes in this cohort include patient age, tobacco use, body mass index (BMI), OCA chondrocyte viability at the time of transplantation, allograft bone pretreatment, and surgical techniques. 2,9,12 –14 Recently, the use of a novel allograft preservation method that significantly improved chondrocyte viability and advancements in treatment protocols—including the use of custom-cut “shell” grafts; fresh meniscal allografts; behavioral screening, counseling, and education; and patient-specific rehabilitation protocols—has been reported to be associated with consistently successful 1- to 4-year outcomes for patients with unipolar, multisurface, and bipolar lesions treated by OCA transplantation in the knee. 12 –15 Concurrently, a large volume of patients, including athletes across a wide variety of sports and levels with complex articular cartilage pathology, have been treated at our institution. As such, a prospective registry was established to collect, analyze, and report data regarding outcomes of all cases of OCA transplantation performed in patients who opted for this treatment and consented to inclusion. The purpose of the present study was to examine outcomes for athletes who underwent either large (>4 cm2) single-surface, multisurface, or bipolar OCA transplantation in the knee using shell grafts. This study was designed to test the hypothesis that for patients undergoing large single-surface, multisurface, or bipolar OCA transplantation in the knee, elite and competitive athletes would return to their preinjury level of sport at a significantly higher proportion when compared to recreational athletes.
Methods
With institutional review board approval and documented informed consent, patients were prospectively enrolled into a dedicated prospective registry designed to follow outcomes after OCA transplantation. For inclusion in the present study, a search of the registry identified persons with a documented preinjury Tegner level ≥5 with type and level of sport or elite unit active military duty documented. Additional criteria for inclusion required patients to have undergone osteochondral and/or meniscal transplantation for the first time (primary transplant) between June 2015 and March 2018 and have at least 1-year follow-up outcomes, including RTS data, documented in the electronic medical record (EMR) and/or registry. Patients in the registry who did not meet all inclusion criteria were excluded from the present study. All grafts were stored using the Missouri Osteochondral Preservation System (MOPS) for 56 days or less after recovery.
This patient registry is based on the senior author (J.P.S.), a fellowship-trained orthopaedic traumatologist and team physician at an academic referral institution, who evaluated a large population of patients pursuing evaluation for their complex knee problems (eg, 1 or more large [≥4 cm2] focal full-thickness articular cartilage defect[s] and/or functional deficiency of 1 meniscus) at a center dedicated to biologic joint restoration. A significant number of these patients either participate or previously participated in athletic activities, including elite, competitive, and recreational sports. As such, review of preinjury activities and expectations for return to activities were components of the patient assessment and education process. Patients underwent a comprehensive diagnostic workup including review of patient history, physical examination, diagnostic imaging including radiographic and magnetic resonance imaging, and diagnostic arthroscopy to determine eligibility for OCA transplantation. When patients chose this treatment over nonsurgical or surgical options and preoperative approval for coverage by their insurance provider was provided, surgeries were performed as indicated (Figure 1).

Intraoperative images of (A) a large single-surface medial femoral condyle shell osteochondral allograft (OCA) transplant and (B) a bipolar medial femoral condyle OCA and medial tibial plateau OCA with attached medial meniscal allograft from patients included in the present study.
OCA transplantation surgeries were performed by 1 or 2 surgeons together using custom-cut patient-specific tab-in-slot shell (∼7 mm thick) grafts stabilized with either 2.4-mm or 2.0-mm cortical screws (DePuy Synthes) placed in lag fashion, bioabsorbable pins (Arthrex), or bioabsorbable nails (ConMed Linvatec). OCA bone was saturated with autogenous bone marrow aspirate concentrate (BMC) (Angel System; Arthrex) immediately before implantation after 3.2-mm subchondral drill holes were created, and the donor bone was thoroughly lavaged to remove marrow elements. Fresh meniscal allograft transplants were performed using a bone plug technique with suspensory fixation or included as part of the tibial OCA transplant. 13
Procedure-specific postoperative management protocols were prescribed to each patient undergoing allograft transplantation in the knee. 12 All patients received verbal and written instructions regarding postoperative rehabilitation. These instructions were also directly communicated to the outpatient physical therapist identified by the patient to be involved in the patient’s postoperative care. Dedicated physical therapists at our center attended all pre- and postoperative outpatient physician visits, provided all inpatient therapy, and either provided outpatient physical therapy or personally communicated with each patient’s outpatient physical therapist throughout the rehabilitation process. During the postoperative period, patient compliance with the prescribed protocol was monitored and documented through patient communication and outpatient physical therapy reports. RTS criteria were specific to the physician, patient, procedure, and sport in assessing the degree of healing, stability, and function deemed appropriate for safe participation in athletic activities. RTS timing and level decisions were made by physicians in conjunction with the athletes, their parents (when applicable), physical therapists, and athletic trainers based on physical examination, diagnostic imaging, and functional performance data. Patients were considered noncompliant if there was documented evidence for definitive breaks in the prescribed protocol during the first year after surgery.
Data were collected preoperatively and at 3 months, 6 months, and yearly after surgery for each case. Patient and operative data were collected from the EMR. The preinjury Tegner level was determined for each patient based on documentation of the highest level of activities, sport, and/or work before the definitive injury or period of time that led to pursuit of surgical treatment for the affected knee. Patient-reported outcome measures (PROMs), including visual analog scale pain scores, International Knee Documentation Committee, Single Assessment Numeric Evaluation, Patient-Reported Outcomes Measurement Information System (PROMIS)–Physical Function, and PROMIS–Mobility, were collected at each time point. All reported complications and reoperations were documented in the EMR and recorded in the registry in order to manage these data for calculating proportions. Revision was defined as a second operation to revise the osteochondral and/or meniscal allograft in at least 1 part of the patient’s knee, and failure was defined as conversion to TKA or UKA. The decision to pursue revision surgery, TKA, or UKA was based on the attending surgeon’s discussion of joint pathology, treatment options, and related prognosis in conjunction with patient preference. Successful outcomes were defined as patients reporting return to functional activities with no need for revision or conversion to TKA or UKA at the last recorded follow-up.
Descriptive statistics were calculated to report medians, means, ranges, and percentages. Paired t tests were used to assess for significant differences between preoperative and final follow-up time points for outcome measures based on continuous data. Fisher exact tests were used to determine significant differences in proportions between or among cohorts and categories of patients. When significant differences in proportions were noted, odds ratios were calculated. Significance was set at P < .05.
Results
Study inclusion criteria were met by 37 patients with large (>4 cm2) single-surface (n = 17; femoral condyle, 14; patella, 3), multisurface (n = 4; condyle-trochlea, 2; condyles, 2), or bipolar (n = 16; femorotibial, 12; patellofemoral, 4) OCA transplantation in the knee using shell grafts for the treatment of injury- or overuse-related articular defects (Table 1). Eleven of the bipolar cases included meniscal transplants. Concomitant procedures were performed in 5 patients and included distal femoral osteotomy (n = 1), high tibial osteotomy (n = 2), anterior cruciate ligament (ACL) reconstruction (n = 1), and ACL and posterior cruciate ligament reconstructions (n = 1). The mean age was 34 years (range, 15-69 years), the mean BMI was 26.2 kg/m2 (range, 18-35 kg/m2), 16 (43%) were female athletes, and none used tobacco. The median final follow-up with all documented RTS data was 24 months (range, 12-50 months).
Patient Characteristics and Surgery Type Based on Level of Sport a

a BMI, body mass index.
The highest preinjury median Tegner level was 9 (mean, 7.9 ± 1.7; range, 5-10). With respect to the general category of sport in which patients participated before injury, 22 patients (59%) were involved in cutting sports while 15 patients (41%) were involved in noncutting sports. Level of sport before injury was categorized as elite unit (airborne or special ops) active duty military (n = 2), competitive collegiate (n = 4), competitive high school (n = 10), or recreational (n = 21).
In total, 25 patients (68%) returned to sport after large (>4 cm2) single-surface, multisurface, or bipolar OCA transplantation in the knee using shell grafts. For those who returned to sport, 17 (68%) returned to the same or higher level of sport compared with the highest preinjury level, while 8 (32%) had returned to a lower level of sport at the final follow-up (Table 2). The median time to RTS was 16 months (range, 7-26 months). No statistically significant differences were noted for RTS proportions between male and female athletes, between patients <40 versus ≥40 years of age, or among single-surface, multisurface, and bipolar OCA transplantations. However, elite unit military, competitive collegiate, and competitive high school athletes returned to sport at a significantly higher proportion (P = .004) than recreational athletes (Table 3).
RTS for Athletes Based on Level of Sport a

a RTS, return to sport.
Comparison of RTS Rate Based on Patient Sex, Age, Type of Surgery, and Level of Sport a

a The boldface P value indicates a statistically significant between-group difference (P < .05). RTS, return to sport.
For all patients, the median Tegner level at the final follow-up was 6 (mean, 6.1 ± 2.7; range, 1-10), which was significantly lower (P = .007) than that at the highest preinjury level. Seventeen patients (46%) had the same or higher Tegner level at the final follow-up compared with their highest preinjury Tegner level.
For PROMs, all scores were significantly higher at the final follow-up when compared with preoperative levels, and all improvements reached or exceeded clinically meaningful differences for pain and function. PROMIS measures reached levels considered normal for the healthy adult population (Table 4).
Patient-Reported Outcomes for Pain, Function, and Mobility a
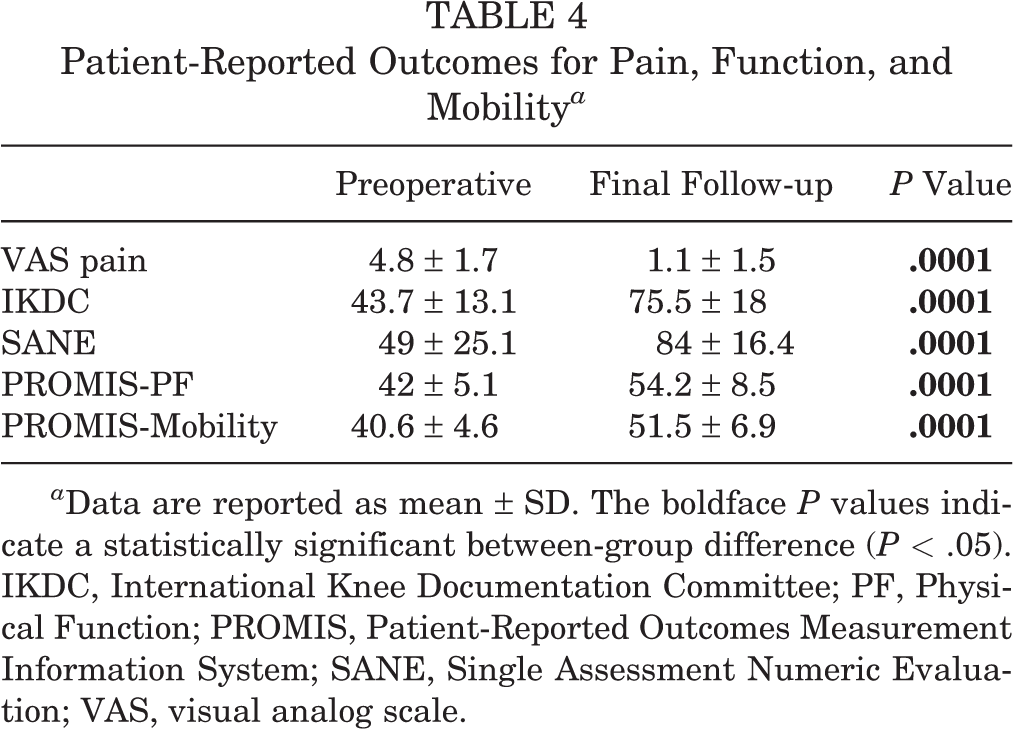
a Data are reported as mean ± SD. The boldface P values indicate a statistically significant between-group difference (P < .05). IKDC, International Knee Documentation Committee; PF, Physical Function; PROMIS, Patient-Reported Outcomes Measurement Information System; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
OCA revisions were performed in 2 patients (5%) and failures requiring TKA occurred in 2 patients (5%), all of whom were recreational athletes. One revision was performed for meniscal allograft transplant tear in a bipolar case and 1 for incomplete OCA bone healing in a multisurface case. Both TKAs were performed in bipolar cases because of incomplete resolution of knee pain and dysfunction and progression of knee pathology. At the time of the final follow-up, OCA revisions were considered successful in both patients in terms of functional outcomes such that the overall OCA survival rate for the patients included in the present study was 95% at 2 to 4 years after transplantation. However, no patient undergoing OCA revision or TKA returned to sport during the time frame of the present study. Noncompliance was documented in 4 athletes (11%), one of whom underwent OCA revision and one of whom underwent TKA. Based on these data, noncompliance with the prescribed postoperative rehabilitation protocol was 15.5 times more likely (P = .049) to be associated with failure or a need for revision than for compliant patients.
Discussion
The results of this study suggest that competitive and recreational athletes can expect a 68% chance to return to some level of sport after large single-surface, multisurface, or bipolar OCA transplantation in the knee using MOPS-preserved allografts, autogenous BMC pretreatment of OCA bone, custom-cut shell grafts, and fresh meniscal allografts in conjunction with patient compliance with behavioral screening, counseling, and education as well as patient-specific rehabilitation protocols. For the two-thirds of athletes who returned to sport, 68% returned to a level that was the same as or higher than the highest level achieved before injury. This included both (100%) of the elite unit active duty soldiers and 3 of 4 (75%) of the competitive NCAA Division I collegiate athletes included in the study. Importantly, RTS cannot be expected before 16 months after OCA transplantation and may take as long as 2 years postoperatively. In addition, based on the results of this study, competitive high school athletes can expect only a 60% chance and recreational athletes only a 29% chance of return to the same or higher level of sport achieved before injury. While these realistic expectations regarding RTS must be communicated to competitive high school and recreational athletic patients before pursuing OCA transplantation, it is important to note that these athletes consistently experienced significant and clinically meaningful improvements in pain, function, physical health, and mobility, such that they were able to return to work, school, and recreation. In addition, RTS for these latter 2 cohorts was often based on choice or opportunity regarding level and type of sport. It is also important to communicate the combined revision and failure rates, which totaled 10% of the patients included in our study. Compliance with the prescribed postoperative rehabilitation protocol significantly influenced the likelihood for revision or failure after OCA transplantation in the knee in our cohort.
Based on differences in patient population, severity of pathology, and treatment techniques, direct comparisons with other studies examining RTS outcomes after OCA transplantation in the knee cannot be made. 4 However, in the authors’ opinion, the 68% rate for RTS noted in the present study for patients undergoing large single-surface, multisurface, or bipolar shell OCA transplantation in the knee compares favorably with the RTS rates (75%-88%) reported for isolated femoral condyle plug grafts. 4 In addition, outcomes for patients in the present study compare favorably with those in previous studies reporting outcomes after large single-surface, multisurface, and bipolar shell OCA transplantation in the knee in the general population. 5 Historically, these more complex OCA transplantation cases have been associated with revision rates of between 39% and 100% and failure rates of between 29% and 46% across patient cohorts. 5 In the present study, 90% of cases were considered successful in returning patients to function without need for revision, and 95% of cases were associated with 2- to 4-year functional survival when including successful revisions, which also compares favorably with previous studies. 3 –5
The primary limitations to consider when interpreting and applying the data from the present study consist of the number and spectrum of athletes included in terms of age, sex, and level and type of sport; the spectrum of pathology included; the single-center study design; and the duration of follow-up. While no statistically significant differences were noted for RTS proportions between male and female athletes, between patients <40 versus ≥40 years of age, or among single-surface, multisurface, and bipolar OCA transplantations, the limitations do not allow for universal applicability of the results to all athletes across all geographical locations, nor can they be considered anything more than initial short-term outcomes. However, the data suggest that OCA transplantation with shell grafts can be considered as an option for athletic patients with complex articular defects in the knee based on RTS outcomes associated with other cartilage repair or restoration treatments and their lack of suitability for TKA or UKA based on age or activity level. 1,6,7,10,16,17
Conclusion
Taken together, the results of this study suggest that OCA transplantation is a valid option for the surgical treatment of large single-surface, multisurface, or bipolar chondral, osteochondral, and meniscal defects in the knee. The combination of high-viability allografts, autogenous BMC pretreatment, and custom-cut patient-specific surgical techniques—as well as patient compliance with preoperative education and postoperative rehabilitation protocols—resulted in two-thirds of athletes returning to sport 16 to 24 months after transplantation. Importantly, revision and failure rates combined were 10%, such that 90% of patients were considered to have successful 2- to 4-year outcomes with significant improvements in pain and function, even when they did not RTS.
Footnotes
Final revision submitted May 19, 2020; accepted June 11, 2020
One or more of the authors has declared the following potential conflict of interest or source of funding: J.L.C. is a member of the medical board of trustees of the Musculoskeletal Transplant Foundation (MTF), which licenses the Missouri Osteochondral Preservation System (MOPS) used in the allograft procedures described in this study. J.L.C. and J.P.S. have received funding from the US Department of Defense and MTF related to this line of research conducted at the University of Missouri. J.L.C. has also received research support from Arthrex, the Coulter Foundation, DePuy Synthes, GE Healthcare, Merial, the MTF, Purina, and Zimmer Biomet; consulting fees from Arthrex and Trupanion; and speaking fees and royalties from Arthrex; and is a board member for the Midwest Transplant Network and MTF. J.P.S. has received research support from the Coulter Foundation; consulting fees from Acelity, Arthrex, DePuy Synthes, NuVasive, Orthopedic Designs North America, and Smith & Nephew; nonconsulting fees from Arthrex and Smtih & Nephew; faculty/speaker fees from DePuy; and royalties from Thieme. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Missouri–Columbia.