
Abstract
Background:
Symptomatic, full-thickness chondral defects often are associated with meniscal deficiencies. These are difficult problems to manage in the young, high-demand patient population. A number of differing techniques have been published with no consensus. While more recent techniques have favored minimally invasive approaches, an open approach with tubercle osteotomy to maximize visualization of all knee compartments can still provide favorable outcomes when using a careful technique and postoperative protocol.
Indications:
Young, high-demand patients with long-standing meniscal deficiency and resultant chondral defects are indicated for cartilage restoration and preservation procedures. A meniscal allograft transplantation is indicated in symptomatic patients with prior total or subtotal meniscectomy. It is important to address other concomitant pathology such as instability, alignment, and chondral defects. Concomitant procedures are often performed with meniscal transplants, including osteochondral allograft transplantation for larger defects.
Technique Description:
This surgical technique video demonstrates a tibial tubercle osteotomy approach to gain access to both the medial and lateral tibiofemoral compartments. An arthroscopic-assisted bone slot technique was performed for meniscal allograft transplantation. Appropriately sized osteochondral allograft bone plugs were then transplanted onto the medial and femoral condyles with a press fit technique.
Results:
At 1-year follow-up, the presented patient has regained full motion and are back to full activities.
Discussion/Conclusion:
Full-thickness chondral defects associated with meniscal deficiency in a young, high-demand patient is a difficult problem to manage. Recent results using minimally invasive approaches have demonstrated favorable mid- and long-term outcomes. In patients with pathology that may preclude a minimally invasive approach, an open technique with osteotomy can still have a promising outcome.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.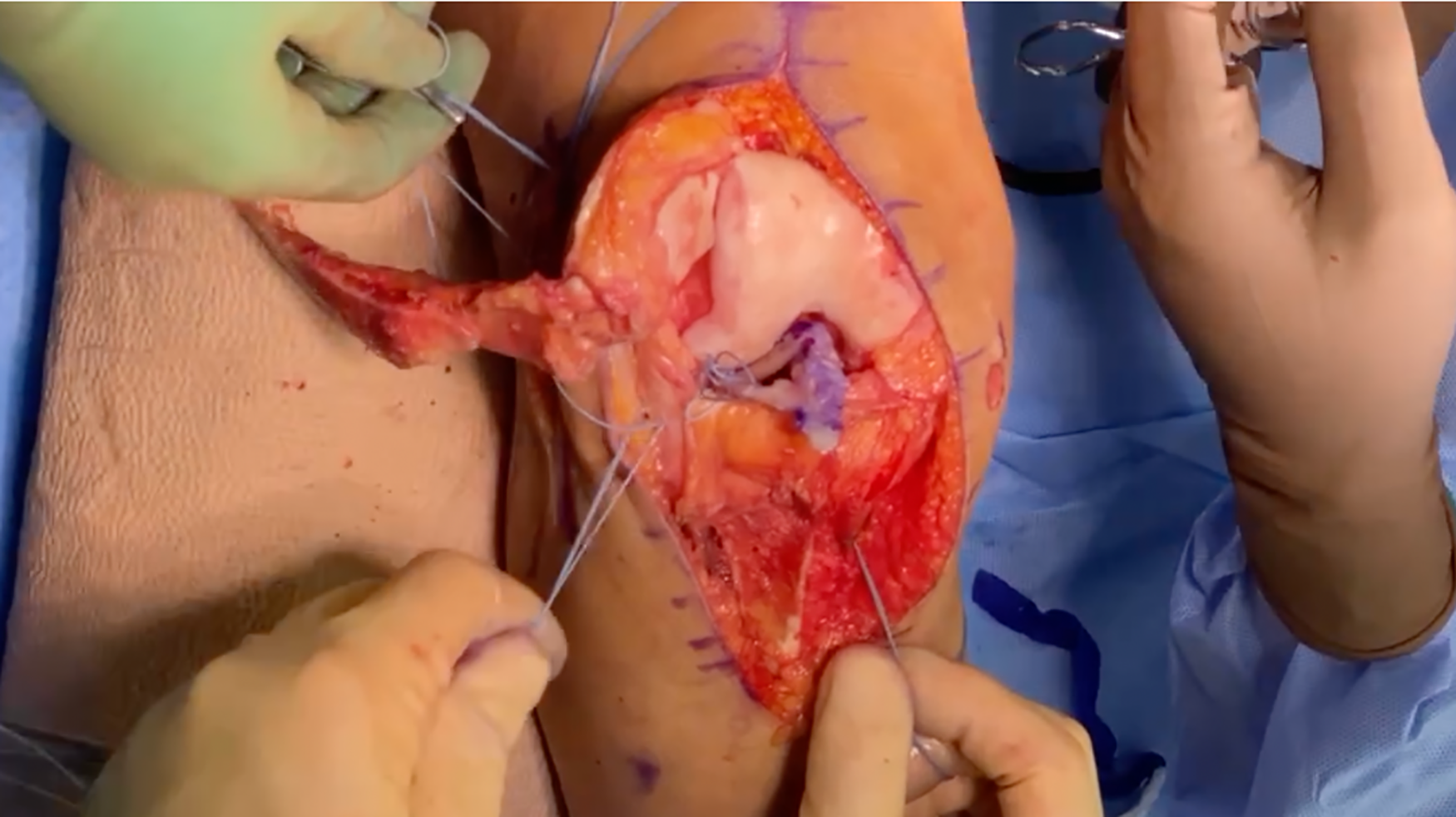
Video Transcript
This is Douglas Nestorovski, Hansel Ihn, Austin Cho, and George F. Rick Hatch from Keck School of Medicine at the University of Southern California, presenting our technique of osteochondral allograft (OCA) transplantation and concurrent lateral meniscus allograft transplantation (MAT). Our disclosures are listed here. Briefly, we will first introduce our patient and follow this with surgical planning and technique. We will close with our postoperative management and patient's outcome at latest follow-up.
The patient is a 32-year-old woman who presented with a chief complaint of chronic right knee pain. At the age of 15, she sustained a tear of her lateral discoid meniscus and underwent an unspecified “debridement” procedure. She has had persistent pain since that time and has dealt with this conservatively. However, her pain was significantly worsened several months prior to presentation after starting a new training program. She had exhausted all conservative measures by the time she presented to us.
On examination, she was able to fully range her right knee but was noted to have a mild effusion along with tenderness to palpation along the lateral joint line. She had a negative McMurray test and stable ligamentous examination. She was also noted to have pain with deep knee flexion. The patient was neurovascularly intact distally.
On radiographic assessment, the patient's right knee was noted to have slight varus alignment with early degenerative changes noted in the medial and lateral compartments. She was also noted to have patella alta.
On magnetic resonance imaging, there was noted absence of a lateral meniscus along with degenerative changes of the cartilage in the lateral and medial compartments. Ligaments were noted to be intact.
A 2-stage surgical plan was initiated. A preliminary diagnostic arthroscopy was planned for diagnostic and surgical planning purposes. During this first stage, the patient was noted to have intact cartilage about the patellofemoral joint. The patella was noted to track centrally within the trochlear groove. The ligaments and medial meniscus were noted to be intact. The tibial surface in both the medial and lateral compartments was noted to have intact cartilage. The medial femoral condyle had a 1.5-cm grade IV lesion on the weightbearing surface. The lateral femoral condyle had a grade IV lesion that was larger than 2 cm × 2 cm. Finally, the patient's lateral meniscus was noted to be largely absent with only remnants of the posterior and anterior root remaining.
A few months after this diagnostic examination, the patient underwent lateral MAT and OCA transplantation of the medial and lateral femoral condyles. The patient was positioned supine with a thigh tourniquet and another diagnostic arthroscopy was performed. The lateral meniscal allograft was then prepared on the back table. A slot technique was planned with use of a 7-mm bone block from a donor. Six vertical mattress sutures were placed (2 for each third of the meniscus: posterior third, middle third, and anterior third). The recipient site was prepared arthroscopically by demarcation of the remnant anterior and posterior roots of the lateral meniscus using electrocautery. A recipient site bone slot was then prepared using the Arthrex system, which uses a combination of a bur and osteotome. Passing sutures were then placed.
We first obtained exposure of the posterior capsule by making a 7-cm incision on the lateral aspect of the knee in line with the iliotibial band. The iliotibial band was split and the lateral collateral ligament was identified. The lateral head of the gastrocnemius was then carefully elevated off the distal femur and proximal tibia to gain access to the posterior capsule. A curved suture lasso was used to pass 4 passing sutures through the capsule. These 4 sutures corresponded to the 4 vertical mattress sutures on the lateral meniscal allograft in the posterior and middle third regions. Passing sutures for the anterior third meniscal sutures were placed percutaneously using a spinal needle. Hemostats were used to organize the sutures.
A medial parapatellar arthrotomy was then performed. The medial and lateral aspects of the patellar tendon were clearly identified. Then, a tibial tubercle osteotomy was performed to gain complete access to both knee compartments. The tubercle osteotomy allowed complete exposure of the both the medial and lateral condyles for fresh osteoarticular allograft placement as well as allowed for ease of concomitant placement of a lateral allograft meniscus transplant, all through a single midline incision. The Arthrex AMZ guide system was used to make a wafer osteotomy which tapered distally. The tubercle was reflected laterally after careful separation of the underlying fat pad and protection of the medial meniscus.
We began with passage of the lateral meniscal allograft. An ACL guide was used to drill a path for another passing suture from the medial tibial metaphysis into the bone block slot for the graft. As opposed to screw fixation, with this slot technique a FiberTape suture is looped through the donor bone block and is passed through a bone tunnel and the block is further secured with a button over the anterior medial tibial metaphysis. The knee was then flexed to 30° and followed by sequential passage and tying of the vertical mattress sutures from posterior to anterior. These were secured down to the capsule.
The localized grade IV lesions on the lateral and medial femoral condyles were then addressed. Both lesions were addressed in a similar fashion starting with the lateral femoral condyle. An appropriately sized guide was chosen. A guide pin was placed in the center of the lesion. The reaming system was used to remove less than 7 mm of subchondral bone. Appropriately sized donor grafts were harvested from a whole distal femur allograft. Pulse irrigation was used to remove marrow elements and each graft was press fit into the defect. The lateral femoral condyle defect required a 22.5-mm plug, and the medial femoral condyle defect required a 15-mm plug. Both were press fit such that the graft sat flush with no prominence. After thorough irrigation of the joint, the tibial tubercle was fixed with 3 lag screws under fluoroscopic guidance. We then checked the knee's range of motion to ensure full flexion and hyperextension could be obtained. The wound was then irrigated once more and closed in layered fashion.
The surgeon needs to be cognizant of several possible complications. Neurovascular injury is of particular concern, especially with passage of sutures for lateral meniscal allograft passage. Other complications that can be associated with meniscal allograft transplantation with the bone slot technique include iatrogenic injury to the cruciate ligaments and violation of the posterior tibial cortex. Complications particular to the OCAs include inappropriate sizing of the graft, which can be avoided by careful measurements at the 3, 6, 9, and 12’o clock positions. It is always better to slightly oversize than it is to undersize. In addition, excessive force during impaction may lead to poor integration secondary to compromised chondrocytes. Finally, both techniques are potentially vulnerable to immunologic allograft rejection.
This slide lists the main pearls of the technique we presented. Our patient had full-thickness lesions on both femoral condyles. Performing her surgical care in 2 stages allowed us to appropriately plan for her management. A remnant of the recipient meniscus should be kept in place to be used as landmarks for proper anatomic placement of donor meniscus and to help prevent radial displacement. While a number of different suture techniques have been described, we have found that spreading out the vertical mattress sutures with an equivalent number of sutures in each third helps with a more anatomic reconstruction. Care should also be taken during the posterolateral approach to visualize the capsule. Repair of the posterior aspect of the meniscus under direct visualization helps avoid iatrogenic injury to the common peroneal nerve. Finally, stiffness is of particular concern in an extensive reconstruction. We prefer the use of a continuous passive motion (CPM) machine immediately on postoperative day 0 to allow range of motion while still protecting the osteotomy and reconstruction.
The patient was instructed to maintain non-weightbearing precautions using a hinged knee brace for the first 8 weeks after operation. After the 8-week time point, the patient was allowed to partially advance weightbearing each week until she was weightbearing as tolerated at 12 weeks postoperatively. The patient was started on a CPM machine immediately postoperatively with motion restricted to 0° to 90° for the first 2 weeks. The patient was instructed to avoid extremes of knee flexion for at least 12 weeks postoperatively.
OCA transplantation with concomitant MAT has become more frequent, with recent evidence demonstrating favorable outcomes. Frank et al 2 used Kaplan-Meier survival analysis to predict probability of survival of grafts and found no significant differences in survival between isolated OCA and OCA with concomitant MAT groups. Furthermore, another study by the same group demonstrated no functional differences between the 2 treatment groups. 1 In addition, no statistical difference between groups was shown for reoperations, graft failures, or time to failure. 1 This study displayed that OCA with concomitant MAT is associated with favorable outcomes and sustainability. Another prospective study from Rue et al 4 further exhibited improved patient outcome scores (P < .001) and additionally reported no complications in 30 patients undergoing combined MAT and articular cartilage repair, 15 of which included OCAs. Some studies have not demonstrated as favorable outcomes. The study by Getgood et al 3 demonstrated that 11 out of 48 patients failed (23%) and had a reoperation rate of 54%; however, this group of failures largely included patients with severe osteoarthritis, infection, and trauma. The previously mentioned study by Frank et al 1 showed that reoperation rates between MAT with OCA and without OCA had no significant difference, along with a failure rate of 12% (excluding patients with severe osteoarthritis). Although the current research on OCA with concomitant MAT is limited, initial studies show that the procedure has improved outcomes with few disadvantages.
Here is our patient at her 5-month follow-up visit demonstrating return of full range of motion, symmetrical gait, and double-leg squat.
Footnotes
Submitted January 11, 2023; accepted June 7, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.N. has received a grant from Arthrex; support for education from Arthrex and Empire Medical; and hospitality payments from Stryker Corporation. G.F.H. is a consultant for Arthrex and NewClips Surgical; received funding from Arthrex for research; fellowship support for the University of Southern California Sports Medicine Fellowship; received support for education from Saxum Surgical; and received honoraria from Fidia Pharma USA. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.