
Abstract
Background:
The effect of the double-incision technique on the supinator muscle is unclear.
Purpose:
The aim of this study was to quantify fatty atrophy of the supinator muscle and map the area of muscle damage.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 19 male patients (median age, 43 years) who underwent distal biceps tendon repair were included in the analysis. Patients with a minimum of 12 months of follow-up were included. The following variables were analyzed: range of motion; shortened version of Disabilities of the Arm, Shoulder and Hand (QuickDASH) score; Summary Outcome Determination (SOD) score; and isokinetic peak force and endurance in supination. Quantitative analysis and mapping of fatty infiltration of the supinator muscle were based on the calculation of proton density fat fraction on magnetic resonance imaging scans of both elbows using the IDEAL (Iterative Decomposition of Echoes of Asymmetrical Length) sequence.
Results:
At an average follow-up of 24 months (range, 12-64 months), the median SOD score was 9.0 (95% CI, 7.8-9.4), and the mean QuickDASH score was 6.7 (95% CI, 0.0-14.1). A difference of 17% in peak torque was measured between repaired and nonrepaired elbows (repaired elbow: 9.7 N·m; nonrepaired elbow: 11.7 N·m; P = .11). Endurance was better in the repaired elbow than the nonrepaired elbow (8.4% vs 14.9% work fatigue, respectively; P = .02). The average fat fraction of the supinator muscle was 19% (95% CI, 16%-21%) in repaired elbows and 14% (95% CI, 13%-16%) in contralateral elbows (P = .04). The increase in fat fraction was located in a limited area between the radius and ulna at the level of the bicipital tuberosity.
Conclusion:
The assessment of the supinator muscle showed a limited increase in fat fraction between the radius and ulna at the level of the bicipital tuberosity. No significant effect on supination strength was highlighted.
A distal biceps tendon rupture is not an uncommon event in patients performing manual work and participating in weight-lifting sports. 1 In active patients, surgical repair is usually indicated to avoid loss of strength in flexion of the elbow and supination of the forearm. 28
Several techniques have been described for distal biceps tendon repair and are broadly divided into single- 14,24,33 and double-incision techniques 8,21,32 based on the number of surgical incisions needed to reach the bicipital tuberosity and repair the tendon. With the single-incision technique, a single more extensive approach from the volar part of the elbow is used to repair the tendon, while with the double-incision technique, 2 separate incisions, one anteriorly to identify and prepare the biceps tendon and a second posterolaterally, are used to repair it to the bicipital tuberosity.
Good outcomes have been described for both techniques; however, there is some evidence that by using a single anterior approach, the anatomic insertion of the biceps tendon to the radial tuberosity is rarely achievable, with subsequent reduction in supination strength. 15,20,31 This is because of the anatomy of the bicipital tuberosity that, even in maximal supination, cannot be entirely approached from a single anterior incision. 15,16 On the other hand, the double-incision technique guarantees a more anatomic insertion of the biceps tendon through a split in the extensor carpi ulnaris and supinator muscles. By providing a more anatomic repair, this technique increases the chances of complete recovery of supination strength. 10 However, the posterolateral approach required to restore the anatomy of the biceps tendon involves violation of the integrity of the supinator muscle, jeopardizing the recovery of supination strength. This is a relevant concern because one of the main objectives of the surgical repair of the distal biceps tendon is the recovery of strength in supination.
The effect of the double-incision technique on supinator muscles has been reported by a single study that described worrisome fatty infiltration of the supinator muscle. 29 According to the authors, fatty infiltration was commonly observed after the double-incision technique, affecting supination strength. This new finding could clarify some unexplained cases of supination weakness after the double-incision technique. 9,11
Quantitative analysis of fatty atrophy and mapping of atrophy of the supinator muscle, both for the affected and healthy sides, have not been performed yet. Information from these analyses can help to reach a better understanding of the pathogenesis of fatty infiltration and suggest a method of prevention. Generalized atrophy of the supinator muscle could suggest a nerve-related abnormality or a pre-existing condition of the muscle-tendon unit. On the other hand, limited atrophy could suggest circumscribed damage of the muscle due to scar tissue around the area of the muscular split.
The aim of our study was to quantify fatty atrophy of the supinator muscle and map the area of atrophy, comparing the affected elbow with the contralateral healthy elbow. The hypothesis was that damage of the supinator muscle would be limited to the area of the surgical approach.
Methods
The study was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and was carried out in accordance with relevant regulations of the Italian National Health Service. With respect to Italian laws, institutional review board approval was not mandatory.
Patients
A total of 28 patients underwent surgical repair of the distal biceps tendon between 2010 and 2017. A double-incision technique with transosseous sutures, as modified by Kelly et al 21 and Morrey et al, 25 was used in all the cases. Patients with a minimum follow-up of 12 months were included. Exclusion criteria were a partial rupture, a history of contralateral distal biceps tendon ruptures, delayed surgical repair of the tendon (≥6 weeks from trauma), and any relative contraindication to undergoing bilateral magnetic resonance imaging (MRI) (ie, claustrophobia, metallic devices, pacemaker).
Among the 28 patients, 4 were not traceable because of erroneous telephone numbers, 3 declined to participate in the study, and 1 underwent contralateral distal biceps tendon repair. Another patient was further excluded for the presence of a metallic foreign body in the bicipital tuberosity (the tip of a broken drill). The remaining 19 male patients (68% of original cohort; median age: 43 years) were included in the study.
Surgical Technique
All the surgical procedures were performed by the same 2 experienced shoulder and elbow surgeons (F.C., D.B.). The patient was placed in the supine position, and a tourniquet, set at 250 mm Hg, was used. First, a 2- to 3-cm transverse incision was made 1 cm distal to the elbow crease. Blunt dissection, preserving the lateral antebrachial cutaneous nerve, was performed to identify the distal biceps tendon. The tendon was prepared using 2 No. 2 nonabsorbable Ti-Cron braided polyester sutures (Medtronic) after removing 3 to 5 mm of degenerated tendon. The original pathway of the biceps tendon was found or re-created carefully, avoiding unnecessary bleeding and traction on the lateral antebrachial cutaneous nerve and radial nerve. A blunt curved instrument was then used to penetrate the space between the proximal radius and ulna at the level of the bicipital tuberosity or more proximally. Gentle pronosupination of the forearm simplified this step, which usually is the most concerning. Once the blunt instrument was palpated in the posterolateral aspect of the forearm, the surgeon performed a second longitudinal skin incision. The use of the blunt instrument was important to center the second incision. Careful blunt dissection, through a split of the extensor carpi ulnaris and supinator muscles, was then performed to reach the bicipital tuberosity of the radius while the forearm was held in maximum pronation. An anterior retractor was placed with careful attention to avoid damaging the posterior interosseous nerve. A high-speed bur was then used to create a half bone tunnel in the radius big enough to accommodate the distal biceps tendon. Usually, a tunnel 12 to 15 mm in length and 10 mm deep was required. Extensive lavage was performed to avoid deposits of bone fragments that could predispose the patient to heterotopic bone formation. During drilling, the use of sterile lubricant gels further reduced the formation of bone dust.
The 2 No. 2 Ti-Cron sutures were then shuttled from anterior to posterolateral, and the tendon was securely repaired using bone sutures after creating three 2-mm holes in the anterior part of the radius. Then, 10 mL of tranexamic acid was inserted in the 2 approaches, and drainage was left in the posterolateral approach for 24 hours.
After surgery, the patient wore a soft bandage for 10 days, and active and passive motion were allowed immediately after surgery. Carrying heavy weights was forbidden for 30 days. Also, 50 mg of indometacin twice a day was prescribed for 3 weeks after surgery to minimize the risk of heterotopic ossification.
Clinical Evaluation
At the time of final follow-up, range of motion (ROM) was assessed in both elbows using a manual goniometer. 7 Patient-reported outcomes were collected using the shortened version of Disabilities of the Arm, Shoulder and Hand (QuickDASH) score 3 and the Summary Outcome Determination (SOD) score. 6 A subjective evaluation of the repaired elbow was also performed by asking patients the following (Subjective Elbow Value [SEV]): “What is the overall percentage value of your elbow if a completely normal elbow represents 100%?”
MRI Examination
To conduct a quantitative analysis of fatty infiltration of the supinator muscle, we developed an experimental protocol derived from a validated method used to quantify fatty atrophy in patients with hepatic steatosis called the IDEAL (Iterative Decomposition of Echoes of Asymmetrical Length) sequence. 12,19 This technique has been previously used in the measurement of fatty infiltration in the rotator cuff. 22,23,26 The IDEAL sequence is an MRI-based technique for fat quantification based on the calculation of proton density fat fraction. Different from other methods based on MRI, it corrects for multiple confounding factors including T1 bias, T2 decay, and noise bias. Previous studies have shown that this MRI analysis has a high diagnostic accuracy for quantifying steatosis compared with liver biopsy results. 2,17 A high correlation was observed between fat fraction measured using the IDEAL sequence and that measured using liver biopsy. A 3% difference between biopsy and the IDEAL sequence was highlighted in patients with a low level of fat fraction. 19
Each patient underwent MRI at final follow-up. Patients were placed in the supine position with the examined arm in a neutral position (palm of the hand facing the body and elbow extended in the middle of the bore). For each patient, the contralateral arm was also examined using the same MRI protocol to make a comparison. MRI was performed on a 1.5-T scanner (450W; GE Healthcare). We used a flex medium coil or a small coil when possible. The following MRI parameters were used:
IDEAL sequence: repetition time (TR), 25.8 milliseconds; echo time (TE), 6 to 7 milliseconds; field of view (FOV), 22 × 22 cm; matrix, 128 × 128; slice thickness, 1.2 mm; flip angle, 10°; bandwidth, 100 Hz.
Axial T1 sequence: TR, 380 to 750 milliseconds; TE, 9 milliseconds; FOV, 160 × 160; slice thickness, 5 mm; gap between slices, 0.5 mm; number of slices, 28.
Axial T2 sequence: TR, 5000 to 6500 milliseconds; TE, 70 milliseconds; FOV, 160 × 160; slice thickness, 5 mm; gap between slices, 0.5 mm; number of slices, 28.
Imaging Postprocessing
Postprocessing software provided by the manufacturer (Advantage Workstation 4.7 GE Healthcare) was used to generate a fat fraction map of the supinator muscle. For each elbow, the examiner placed 4 circular regions of interest (ROIs) in the supinator muscle for each slice as determined on T1-weighted axial images. The fat fraction for each ROI was then calculated.
To provide reliable positioning of the ROIs, the supinator muscle was mapped using 2 perpendicular lines in each slice. The reference line was drawn between the supinator crest of the ulna and the center of the radial shaft (Figure 1). The second perpendicular line was placed in the center of the radial shaft. There were 4 circular ROIs plotted according to these lines (ROI-A, ROI-B, ROI-C, ROI-D) so that they occupied the maximum possible areas of the supinator muscle. ROI-A and ROI-C were centered with the reference line, and ROI-B and ROI-D were placed perpendicular to the reference line. All the ROIs were plotted clockwise on the right elbow and counterclockwise on the left elbow so that ROI-B was always in the anterolateral position.

Mapping of the fat fraction of the supinator muscle in the (A) nonrepaired elbow and (B) repaired elbow. The white circles represent the different regions of interest of the supinator muscle used to quantify the fat fraction.
The bicipital tuberosity was used as the main landmark to establish MRI slices to pick for measurements; it was located between slices 3 and 5. In these slices, because of the physiological absence of the supinator muscle, ROI-A and ROI-D were shifted laterally and medially with respect to the other 2 reference lines drawn between the medial and lateral borders of the ulna and radius (Figure 2). Figure 3 shows the relationship between the bicipital tuberosity and the ROIs in a nonrepaired elbow at the level of slice 4.

Mapping of the fat fraction of the supinator muscle in the (A) nonrepaired elbow and (B) repaired elbow. The white circles represent the different regions of interest (ROIs) of the supinator muscle used to quantify the fat fraction. ROI-A and ROI-D are shifted laterally and medially with respect to 2 reference lines (dotted lines) drawn between the medial and lateral borders of the ulna and radius.

A schematic drawing of a magnetic resonance imaging scan at the level of slice 4 in a nonrepaired elbow.
Mapping of the supinator muscle started 1.5 cm below the joint line between the radial head and capitulum humeri and continued distally for a total of 10 slices, each every 5 mm. A total of 40 ROIs (4 ROIs for each slice for a total of 10 slices) were thus determined for each elbow with the aim of mapping 5 cm of the supinator muscle.
Moreover, for each slice, another ROI that included the entire surface of the supinator muscle belly was plotted to calculate the fat fraction of the entire supinator muscle (ROI-T). The surface cross-sectional area of the entire supinator muscle belly was also measured for each slice. An additional ROI was placed in the pronator muscle as a control (ROI-P). Analysis was conducted on the right elbow and then on the contralateral one. The examiner (A.O.) was unaware of the elbow that had undergone surgery.
Validation
To validate the study protocol, intraobserver analysis was performed. A total of 10 repaired elbows were randomly selected, and the examiner measured the fat fraction by plotting the ROIs in each elbow as described. The examiner was a radiologist with more than 15 years of practice using MRI to evaluate musculoskeletal disorders. The decision to test the validity of the measurements using the repaired elbow was made considering that the worst reliability was expected in the repaired elbow because of potential confounding factors, such as scar tissue and sutures. The measurements were repeated after 2 weeks. Intraclass reliability was calculated using the Bland-Altman method. 4,5 The Bland-Altman method defines the limits of agreement. This system is based on the mean and SD of differences between ratings. The Bland-Altman method measures reliability as the potential error between measures, defining the smallest detectable difference (SDD). ROIs that showed differences in fat fraction between nonrepaired and repaired elbows, inferior to the SDDs, were considered unreliable. In such conditions, we could not exclude the possibility that the difference between nonrepaired and repaired elbows was caused by potential errors of measurements instead of true differences. The SDD was calculated using intraobserver reliability only because the protocol of the study was based on searching differences between repaired and nonrepaired elbows in the same patients evaluated by the same observer.
Isokinetic Evaluation of Strength and Endurance
Supination strength and endurance were measured using a Humac Norm isokinetic machine (CSMi Solutions). Each patient performed the test first using the right arm. The patient sat with the elbow flexed to 90° and belts placed around the forearm, trunk, and shoulders. A trial test was performed for both elbows. Strength was measured by using 3 maximal repetitions at 30 deg/s with ROM of 60°-0°-60° of the forearm. Endurance was measured by using 15 maximal repetitions at 120 deg/s with ROM of 60°-0°-60°.
The parameter used to assess strength was the mean peak torque (N·m), and work fatigue was used to assess endurance. Work fatigue was the ratio of the difference, expressed as a percentage between work performed in the first third of the test and that performed during the last third of the test, using the following formula:

Statistical Analysis
For analysis of demographic and clinical data of the patients, the mean and 95% CI were considered. The D’Agostino-Pearson test was used to examine the normal distribution of the collected data; thus, a parametric statistical analysis was performed except for the SOD score, for which a nonparametric analysis was used. The fat fraction for each ROI was compared between the nonrepaired and repaired sides using the paired Student t test. The paired Student t test was also used to compare data obtained via isokinetic evaluations. Significance for all tests was set at P < .05. A multiple linear regression analysis was performed to determine the effect of the fat fraction, average cross-sectional area, and dominant arm on supination strength (peak and fatigue).
A post hoc analysis was performed to exclude type II errors. A previous study has shown a difference of 3% between biopsy and the IDEAL sequence in patients with a low level of fat fraction. 19 We considered a minimum difference of 4% to be relevant. In our cohort of patients, the SD of the total fat fraction in the repaired elbow was 4.9 and in the nonrepaired elbow was 3.3. Sample size analysis suggested that a minimum of 18 patients should be included (α = .05; β = 0.2). MedCalc statistical software (MedCalc Software) was used to perform statistical analyses of the data.
Results
For the 19 male patients, the average follow-up was 24 months (range, 12-64 months). Surgery involved the dominant arm in 68% (13/19). The dominant arm was defined by asking the patient which was the arm that he/she chose to write and handle things.
The limits of agreement (SDDs) for the variables are reported in Table 1. The best agreement (lower limit of agreement) was measured for variables ROI-P, ROI-T, ROI-B, and ROI-C. The worst agreement was reported for cross-sectional area, ROI-A, and ROI-D.
Smallest Detectable Differences Allowed by Study Protocol a

a ROI, region of interest.
MRI scans showed that the distal biceps tendon was attached at the level of the bicipital tuberosity in all the elbows. No significant partial tears were observed in the nonrepaired elbows, and no recurrent lesions were observed in the repaired elbows. The bicipital tuberosity was located between slices 3 and 5, starting approximately 25 mm from the proximal portion of the radial head.
The average fat fraction of the supinator muscle was 19% (95% CI, 16%-21%; range, 12%-30%) in the repaired elbows and 14% in the nonrepaired elbows (95% CI, 13%-16%; range, 9%-21%) (P = .04). The biggest differences in fat fraction were observed between slices 3 and 6, with a peak in slice 4. In slices 3 to 6, the difference was greater than the corresponding SDD.
Mapping of the supinator muscle’s fat fraction according to ROIs is reported in Figure 4. The biggest difference in fat fraction was measured at the level of the bicipital tuberosity in ROI-A (slices 3-5). ROI-B, ROI-C, and ROI-D did not show an increase in fat fraction bigger than the SDD. ROI-T was significantly higher in the repaired elbows than in the contralateral elbows between slices 3 and 5 (Table 2).
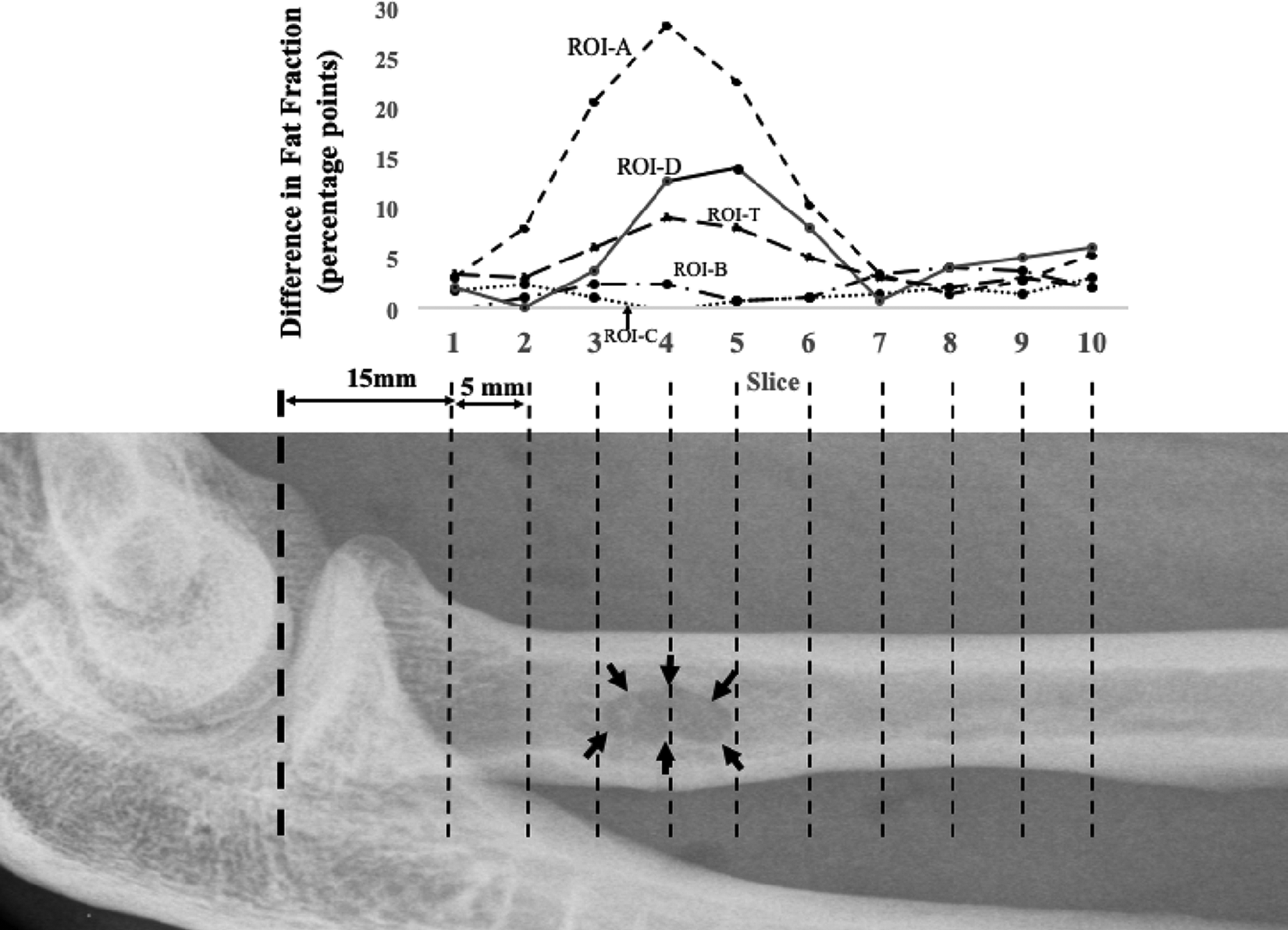
The differences in fat fraction for every slice. Every region of interest (ROI) has a curve and shows the trend of fat fraction. Black arrows show the area of insertion of the repaired biceps tendon. ROI-A shows a statistically significant difference in fat fraction at the level of the bicipital tuberosity (P < .05).
Differences in Fat Fraction and Supinator Muscle Cross-sectional Area Between Repaired and Nonrepaired Elbows a

a Bold values indicate a difference between repaired and nonrepaired elbows that was statistically significant (P < .05) and that was greater than the smallest detectable difference. ROI, region of interest.).
An overall increase in the area of the supinator muscle was observed in the repaired elbow compared with the nonrepaired elbow (Table 2). The increase was, however, not statistically different and was inferior to the SDDs for such variables.
Clinical Outcomes and Isokinetic Evaluation
The median SOD score was 9.0 (95% CI, 7.8-9.4; range, 5-10), and the mean QuickDASH score was 6.7 (95% CI, 0.0-14.1; range, 0-59). The mean SEV was 89.7 (95% CI, 83.4-96.1; range, 50-100). The ROM was normal in extension and flexion (0°-140°) in all patients. Pronation and supination were normal in all patients except 1, who had a loss of 20° of pronation. Radiography in this patient showed heterotopic ossification around the bicipital tuberosity. Another 3 patients had some evidence of heterotopic ossification but normal ROM.
A difference of 17% in peak torque was measured between repaired and nonrepaired elbows (repaired elbow: 9.7 N·m; nonrepaired elbow: 11.7 N·m; P = .11). The endurance test, however, showed a reduction in work fatigue in the repaired elbow (repaired elbow: 8.4%; nonrepaired elbow: 14.9%; P = .02).
Multiple regression analysis revealed a significant correlation between the fat fraction in ROI-B and ROI-C and strength in supination for both the repaired and nonrepaired elbows (fat fraction for ROI-B: t = –2.6; P = .013; fat fraction for ROI-C: t = –19.0; P = .045). The increase in fat fraction was not related significantly to changes in peak force and work fatigue.
Discussion
Surgical repair of the distal biceps tendon has the purpose of restoring strength in flexion and supination. Use of the double-incision technique has been promoted in the past for its ability to restore the anatomy of the biceps tendon, hence allowing complete functional restoration. More recently, use of the double-incision technique has been questioned because it damages the supinator muscle, thus jeopardizing supination strength. 29 This study, based on an MRI quantification of fat fraction, has partially confirmed this hypothesis. An overall increase in fat fraction from 14% to 19% was observed in our cohort of patients. This increase of 5% was caused by an increase in fat fraction of the supinator muscle at the level of the bicipital tuberosity for approximately 1 cm (slices 3-5), confirming our hypothesis that the increase in fat fraction was directly related to the surgical incision for the lateral approach.
A general increase in fat fraction of the supinator muscle was not observed, excluding neurological damage or other causes of diffuse fatty atrophy of the supinator muscle. The circumscribed increase in fat fraction did not have a significant effect on supination strength in our cohort of patients. This could be related to the fact that the increase in fat fraction was observed in ROI-A at the level of the bicipital tuberosity, which is a small area where few fibers of the supinator muscle cross the area between the radius and ulna. The much larger ROI-C and ROI-B, which represent most of the supinator muscle, were not significantly affected. The importance of the supinator fibers at the level of ROI-B and ROI-C was also confirmed by the relationship between the fat fraction in ROI-B and ROI-C and the peak of supination strength. This study showed that for the high fat fraction in ROI-B and ROI-C, the peak of supination strength was reduced in both repaired and nonrepaired elbows. On the contrary, fat fraction in ROI-A and ROI-D did not seem to affect supination strength. This could explain why the increasing fat fraction in ROI-A observed between repaired and nonrepaired elbows had no effect on supination strength.
Another potential explanation of the lack of supination impairment between repaired and nonrepaired elbows is that most of the patients had undergone surgery on the dominant arm. A postoperative reduction of supination strength could have been hidden by greater pretrauma strength in supination in the dominant arm. 13 The fact that the cross-sectional area of the supinator muscle was generally bigger in the repaired elbow than in the contralateral elbow could corroborate this hypothesis. An intense postoperative rehabilitation program focused mostly on the repaired elbow could be another potential explanation. However, we cannot exclude that the increase in the cross-sectional area of the supinator muscle might be a direct consequence of surgical trauma due to edema or scar tissue.
The isokinetic assessment of supination strength also showed that endurance was better for the repaired than the nonrepaired elbow. The mean percentage of work fatigue for supination was 8.4% in the repaired elbows and 14.9% in the nonrepaired elbows. Similar outcomes have been previously reported 27 and justified with the predominance of distal biceps tendon repair on the dominant arm.
Although the difference in supination strength between repaired and nonrepaired elbows measured in our study was not statistically different, it is important to note that a difference of 17% in peak torque was measured between repaired and nonrepaired elbows. This is in accordance with other reports. 18,29 The reason for this difference is probably multifactorial, and limited damage of the supinator muscle secondary to the posterolateral approach is, according to our study, a marginal factor. Other variables could have played a more relevant role. A deficit in neuromuscular control and loss of cam effect due to reduction of the radial tuberosity and damage to the anterior protuberance can reduce the supination moment while the arm is at 60° of supination. 30 Future studies should investigate if different positioning of the tendon, preserving the anterior protuberance, and modifying the double-incision technique to diminish supinator muscle damage could improve outcomes including supination strength.
The small sample size is a limitation of the study, potentially affecting the statistical significance among differences in supination strength. Overall, 32% of the patients were lost to follow-up. This is quite a high number and probably results from a combination of factors including the nature of the distal biceps tendon rupture, which affects young active patients. These patients are reluctant to miss days of work for studies that, by their nature, require longer times for follow-up examinations.
We accepted the limitation related to the small sample size because the main purpose of our study was to map the damage of the supinator muscle. For this reason, we based our study on bilateral MRI using a method of quantification of the fat fraction that is considered to be the gold standard. 12 Quantitative analysis of the fat fraction has been investigated in several fields of medicine. In orthopaedics, several studies have been carried out on fat fraction of the rotator cuff in which the IDEAL water-fat separation method has shown high reliability. Compared with semiquantitative analysis of fatty infiltration of the rotator cuff, the IDEAL technique has shown better correlation with clinical scores. 26 Considering the ability of the IDEAL technique to compensate for several confounding factors, it is now considered an accurate and valid tool to quantify fat in soft tissue either in vitro or in vivo. Despite the fact that it has never been used previously in the elbow, good results in the shoulder are promising for its use in the elbow. 22,23 To limit the drawbacks of the absence of studies of the IDEAL sequence in the elbow, we tested the reliability of our study protocol. However, future studies are needed to test the validity of the IDEAL sequence in the elbow including interobserver reliability, which was not assessed in this study.
Conclusion
A bilateral MRI assessment of the supinator muscle revealed a limited increase in fat fraction in a small area between the radius and ulna, with minimal differences seen in supination strength. The fat fraction of the supinator muscle in regions that were not violated during the posterolateral surgical approach seemed to be more relevant for supination strength.
Footnotes
Final revision submitted May 13, 2020; accepted June 3, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.B. is a teaching consultant for Orthofix and Zimmer Biomet. F.C. is a teaching consultant for Zimmer Biomet. R.R. is a teaching consultant for Mitek, DePuy, Lima, Zimmer Biomet, Medacta, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.