
Abstract
Background:
Meniscal tears are a common knee injury. Isolated meniscal tears are less common; however, unaddressed tears can be troublesome, particularly for athletes. There is currently a lack of data in the literature on athletes returning to play after isolated meniscal repair.
Purpose:
To evaluate the return to play rate and time to return to play for athletes with isolated meniscal injuries.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A search of the PubMed, EMBASE, and Cochrane electronic databases was conducted to identify studies that reported the time and the rate of return to play in athletes after repair of isolated meniscal tears. Studies were excluded if there was a concomitant anterior cruciate ligament reconstruction, if there was a meniscectomy instead of a meniscal repair, or if the study was a systematic review. Quality assessment and data extraction were performed by 2 examiners.
Results:
Overall, 21 studies were included in this review. There were 355 athletes (358 knees) with a mean age of 22.5 years (range, 9-68 years). A sex breakdown was noted in 16 of the 21 (76.2%) studies with 224 men and 71 women. The specific repair technique was described in 259 (72.3%) knees. Of the total knees, 109 (30.4%) had an open repair, 128 (35.8%) had an inside-out arthroscopic technique repair, and 22 (6.1%) had an all-inside arthroscopic technique repair. Complications were addressed in 11 studies, with 13 out of 155 (8.4%) patients across the 11 articles having a postoperative complication. Of the total 355 patients, 295 (83.1%) returned to play, and 17 of these 21 (81.0%) articles reported the time it took for athletes to return to play, with a mean return of 8.7 months.
Conclusion:
The study results indicate that return to play rates after isolated meniscal repair are high, with an overall return to play rate of 83.1% and a mean return to play time of 8.7 months. However, the limited number of studies, particularly ones with larger patient numbers, highlights the need for further investigation regarding isolated meniscal repair in athletes.
Meniscal tears make up approximately 66% of all knee injuries and are more common in men than in women. 35 Intact menisci are crucial for preserving knee function since the menisci play a role in shock absorption, force distribution, and joint stability. In regard to athletes, the menisci provide proprioceptive feedback related to acceleration, deceleration, velocity, and direction. 4,14,24 Partial and especially total meniscectomies can put a patient at high risk for early cartilage degenerative changes, such as narrowing of the joint spaces or osteoarthritis. 6,8,16,18,20,23 Therefore, tears that are repairable slow or prevent the progression of arthritic changes. Furthermore, it is less common for athletes to have isolated meniscal repairs; Stein et al 33 reported that 70% to 80% of patients undergoing a meniscal repair also have a concomitant anterior cruciate ligament (ACL) reconstruction and that only 5% of patients receive isolated meniscal repairs.
Open meniscal repairs are rarely performed in the current management of meniscal tears. The advent of improved meniscal repair devices and arthroscopic techniques have relegated open meniscal repair procedures to more of a historical reference, in addition to other orthopaedic trauma surgeries requiring open exposure of the knee joint. 3 Meniscal repairs in athletes present a challenge with regard to treatment, rehabilitation, and return to sports. Eberbach et al, 8 in a study on 664 patients undergoing meniscal repair, reported that patients were allowed to bear partial weight at an average of 1.1 weeks (range, 0-4 weeks) and full weightbearing after 5.0 weeks (range, 3-10 weeks) postoperatively. Patients were allowed to perform full flexion motion at a mean of 5.7 weeks (range, 4-8 weeks). Patients were allowed to return to normal activity, including sports, at an average of 4.3 months (range, 1-6 months) postoperatively.
There are limited data in the literature regarding athletes returning to play after isolated meniscal repair. To our knowledge, there is only 1 previous systematic review that has reviewed the incidence, management, and return to play in this patient population. 8 However, the previous review was more limited in explicit return to play rates and focused more on subjective outcome measures to determine return to play rates. Therefore, the purpose of this study was to evaluate the management and outcomes, including return to play rates, of isolated meniscal repair in athletes by systematic review.
Methods
Search Strategy
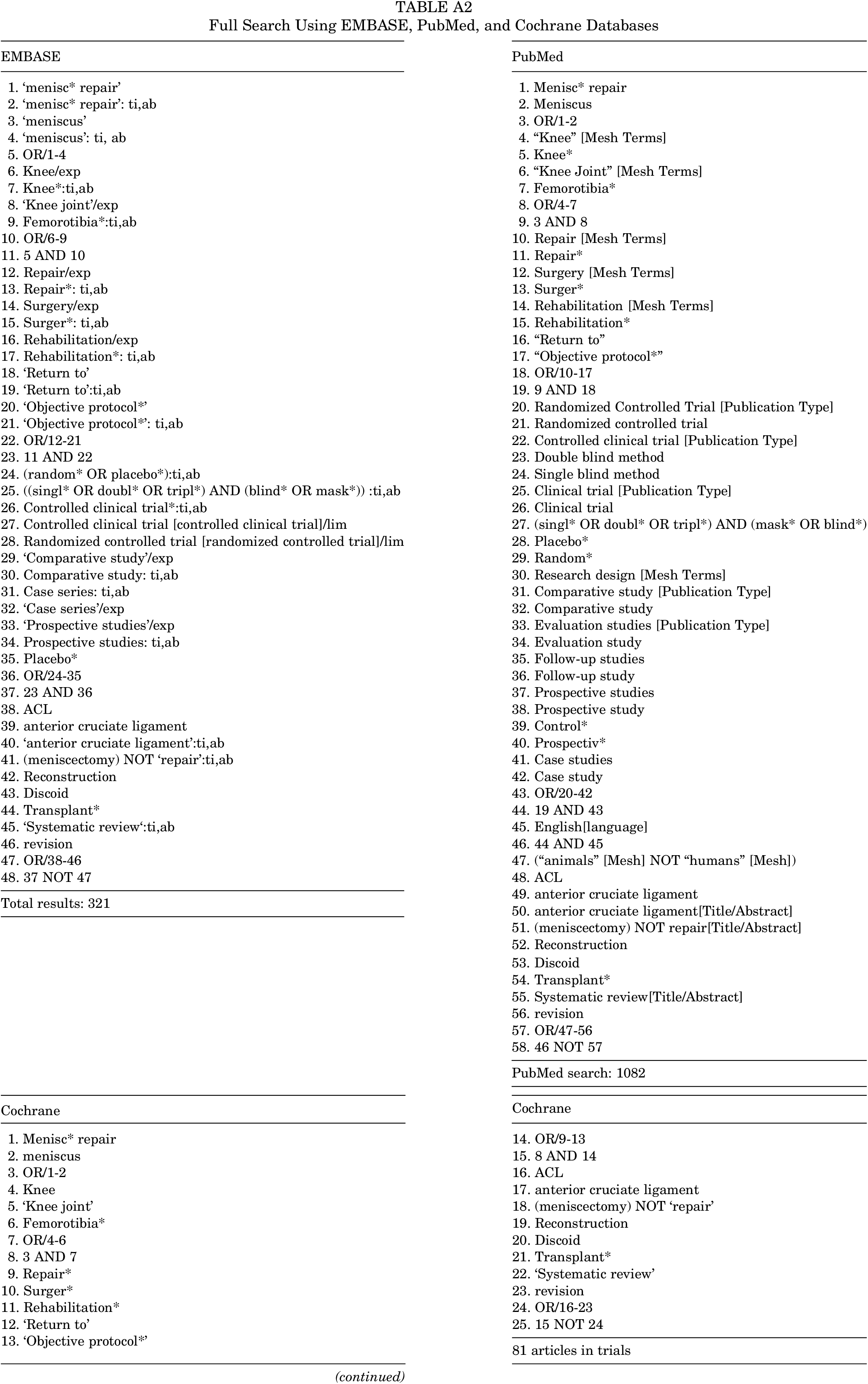
The literature search was completed using the PubMed, EMBASE, and Cochrane databases with a search from inception until June 7, 2019. Search terms included several combinations of keywords such as “knee joint,” “meniscus repair,” and “return to.” The search was limited to the English language and human participants. The full search is available in the appendix. Two reviewers (E.R.B., C.J.H.) independently screened titles and abstracts to determine eligibility of inclusion. Potential full-text articles were then obtained and thoroughly reviewed for inclusion. In addition, the references of all the selected full-text articles were screened to see if any possible papers were overlooked. After removing ineligible articles and duplicates, the search resulted in 21 articles (Figure 1).
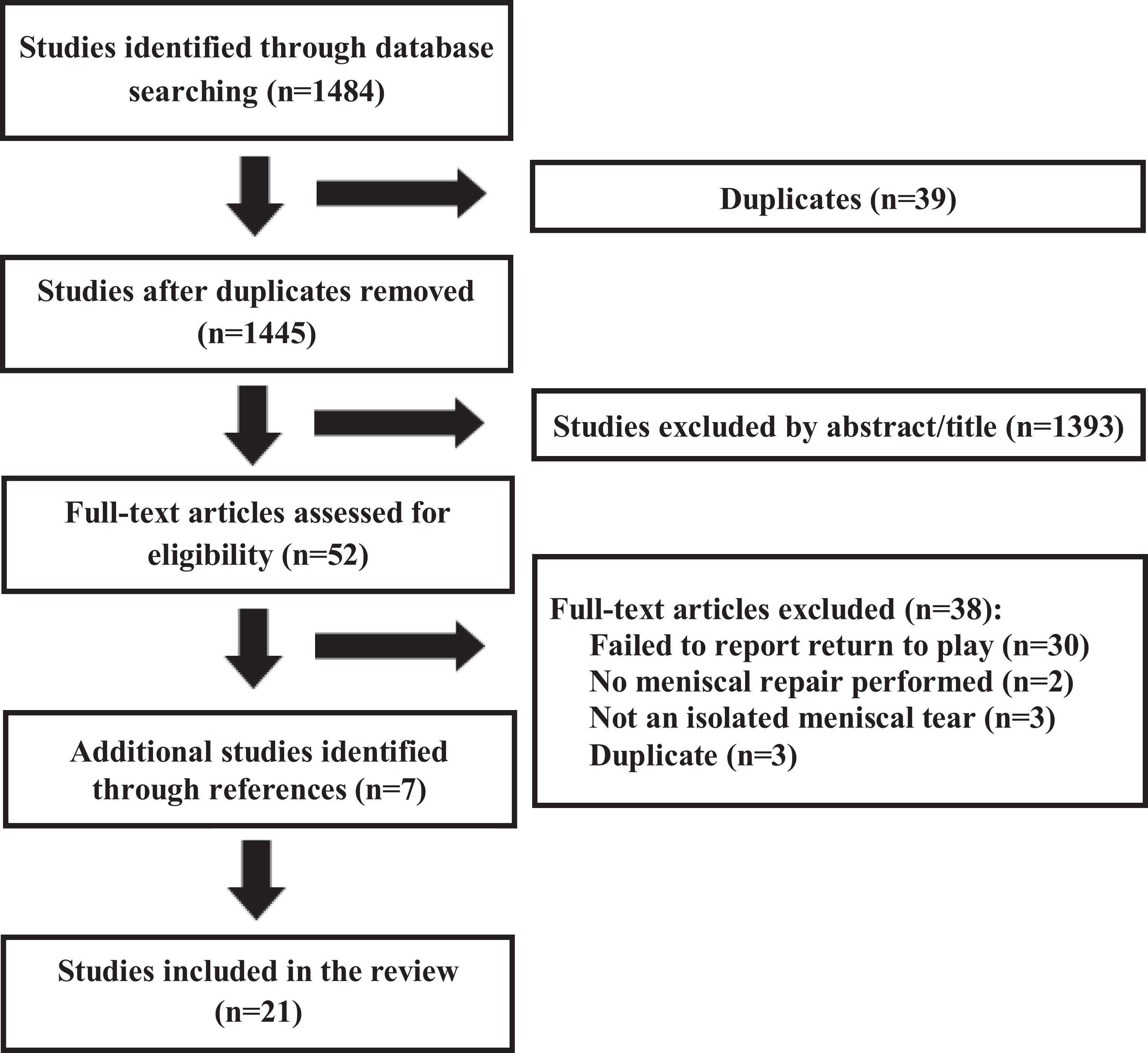
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) chart outlining the review of articles from the search.
The inclusion criteria for this study were as follows: (1) isolated meniscal repair without concomitant ACL repair, (2) indication of the number of athletes and when the athletes returned to play, (3) and level of evidence 1 to 4. This systematic review was not limited by the surgical technique performed, characteristics such as age or sex of the patients, or the type of sport that the athletes played. Return to play was determined by explicit mention in the text of whether athletes returned to their preinjury level of play. Exclusion criteria included patients undergoing concomitant ACL reconstruction and patients undergoing either meniscectomy or meniscal transplant. In this study, many of the papers (n = 1393) were removed based on the title and abstract of the paper. For many of these papers, athletes also underwent concomitant ACL reconstruction at the time of their meniscal repair or underwent partial meniscectomy and not meniscal repair.
Data Extraction
The following data points were recorded when available: number of patients with isolated meniscal repairs, patient characteristics (age and sex), sport played, surgical technique used, number of patients who returned to play, time to return to play, number of revision surgeries, complications, and subjective outcome scores. The data collected were used to evaluate return to play time and rate for athletes with isolated meniscal repairs.
Quality of Literature Methodology
The quality of the methodology for each study was assessed by 2 reviewers (E.R.B., C.J.H.) using the Modified Coleman Methodology Score (MCMS).
Statistical Analysis
Statistical analysis was performed with a Student t test using Microsoft Excel to determine the significance between return to play rates. Throughout the systematic review process, PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) criteria were followed (Figure 1).
Results
Study and Patient Characteristics
Of the 21 articles included in this review, 4 were prospective, 6 were retrospective, 4 were case reviews, and 7 were case studies (evidence level 4). A summary of the selected articles is listed in Table 1. There was a total of 355 athletes (358 knees) included in our study, with participation in a variety of sports. The specific sports were listed in 12 of the 21 (57.1%) articles (with the number of articles mentioning the sport) and included football (n = 5), soccer (n = 4), basketball (n = 3), volleyball (n = 2), baseball (n = 1), track (n = 1), wrestling (n = 1), water skiing (n = 1), rugby (n = 1), softball (n = 1), handball (n = 1), running (n = 1), tae kwon do (n = 1), ice hockey (n = 1), gymnastics (n = 1), lacrosse (n = 1), and mud wrestling (n = 1). ∥ The mean patient age was 22.5 years (range, 9.0-68.0 years), with 16 of the 21 (76.2%) studies reporting a sex breakdown of 224 men and 71 women. The repair technique was reported in 259 (72.3%) knees: 109 (30.4%) knees had an open repair, 128 (35.8%) had an inside-out arthroscopic technique repair, and 22 (6.1%) had an all-inside arthroscopic technique repair. Patients had their final follow-up at a mean of 40.5 months (range, 2.5-165.5 months) after surgery.
Study Characteristics a

a CR, case report; CS, case series; NR, not reported. Dash implies where the average cannot be calculated.
Return to Play
Of the 355 patients, 295 (83.1%) athletes were able to return to play. Seventeen of the 21 (81.0%) articles reported the time it took for athletes to return to play with a mean return of 8.7 months (range, 3.4-30.0 months) (Table 2).
Summary of Outcomes a

a NR, not reported.
b Of the 28 patients, 21 were contacted on follow-up.
c Of the 24 patients, 18 were contacted on follow-up.
d Of the 10 patients, 9 were contacted on follow-up.
Surgical Technique
The surgical techniques performed varied across the studies. Three of the 21 (14.3%) 1,6,27 articles utilized an open surgical technique. The open meniscal repair is rarely used today and is reserved for patients in whom a meniscal cyst cannot be removed arthroscopically. 27 The open technique has some subtle variances, but these differences share a common base technique. Initial investigation of the knee joint is performed by arthroscopic evaluation of all intra-articular structures. Meniscal injuries are confirmed, and the morphology and extent of the tear are classified. 1,6,27 An incision is made posterior or anterior to the collateral ligament with respect to the location of the meniscal tear. 1,6,27 Most commonly, the technique was utilized for repair of horizontal posterior horn tears of the medial meniscus. An incision posterior to the medial collateral ligament is described in these cases. 6,27 The incision is taken down to the level of the joint capsule. The capsular incision for an arthrotomy is centered on the meniscal tear. The meniscus is then exposed, and the edges of the tear are debrided with a scalpel, rasp, or curette. A vertical suturing technique through the meniscus has been described with absorbable polydioxamone, 27 chromic catgut, 1 and permanent (Tycron) 6 suture. If only a meniscal tear gap repair was performed without incorporating the capsule into the repair, the meniscocapsular junction was then closed independently. 1,6,27 In all techniques, the arthrotomy was repaired and layered closure of subcutaneous tissue and skin was completed. 1,6,27 Open repairs are rarely employed in the current management of meniscal tears, as they pose a higher risk of neurovascular injury and less invasive techniques have proven effective.
Sixteen of the 21 (76.2%) reports described an arthroscopic technique, and the 2 remaining articles reported a combination of open and arthroscopic techniques 25,29 but did not specify which surgical technique was utilized for the patients with isolated meniscal repairs. Therefore, some of the data from these 2 studies were not included in the below calculations. This systematic review found that the open surgical technique was performed in 109 of the total 358 (30.4%) knees. For athletes receiving an open repair, 75 of the 107 (70.1%) patients returned to play. An arthroscopic technique was used in 206 (57.5%) knees. In the 16 articles that described the utilization of any type of arthroscopic technique, 197 of the 205 (96.1%) patients returned to play, resulting in a significantly higher (P < .001) return to play rate compared with the open technique. The arthroscopic technique was able to be further subclassified as either an all-inside or inside-out technique depending on the approach. The inside-out technique was utilized in 7 of the 21 (33.3%) articles in a total of 128 (35.8%) knees. 4,11,14,23,32,33,36 For patients undergoing the inside-out technique, 117 of the 128 (91.4%) patients returned to play. The all-inside technique was performed in 5 (23.8%) articles in a total of 22 (6.1%) knees. 2,15,20,26,31 For the 22 patients undergoing the all-inside technique, 21 (95.5%) athletes returned to play. The remaining 4 (19.0%) articles 13,16,21,24 either used a combination of different surgical techniques or did not specify which arthroscopic technique was used.
For the athletes returning to play, the mean time of return after the open technique was 12.0 months. When examining the return to play time for patients undergoing arthroscopic repair, this included 128 patients with an inside-out repair, 22 with an all-inside repair, and 55 patients with an unspecified type of arthroscopic repair. Together, when examining the 205 patients who had an arthroscopic repair, the mean return to play time was 8.0 months. Regarding the subtypes of arthroscopic repair, the mean return to play time was 8.8 months for the 22 athletes with an all-inside arthroscopic technique and 8.9 months for the 128 patients who underwent inside-out arthroscopic repair.
Subjective Outcome Scores
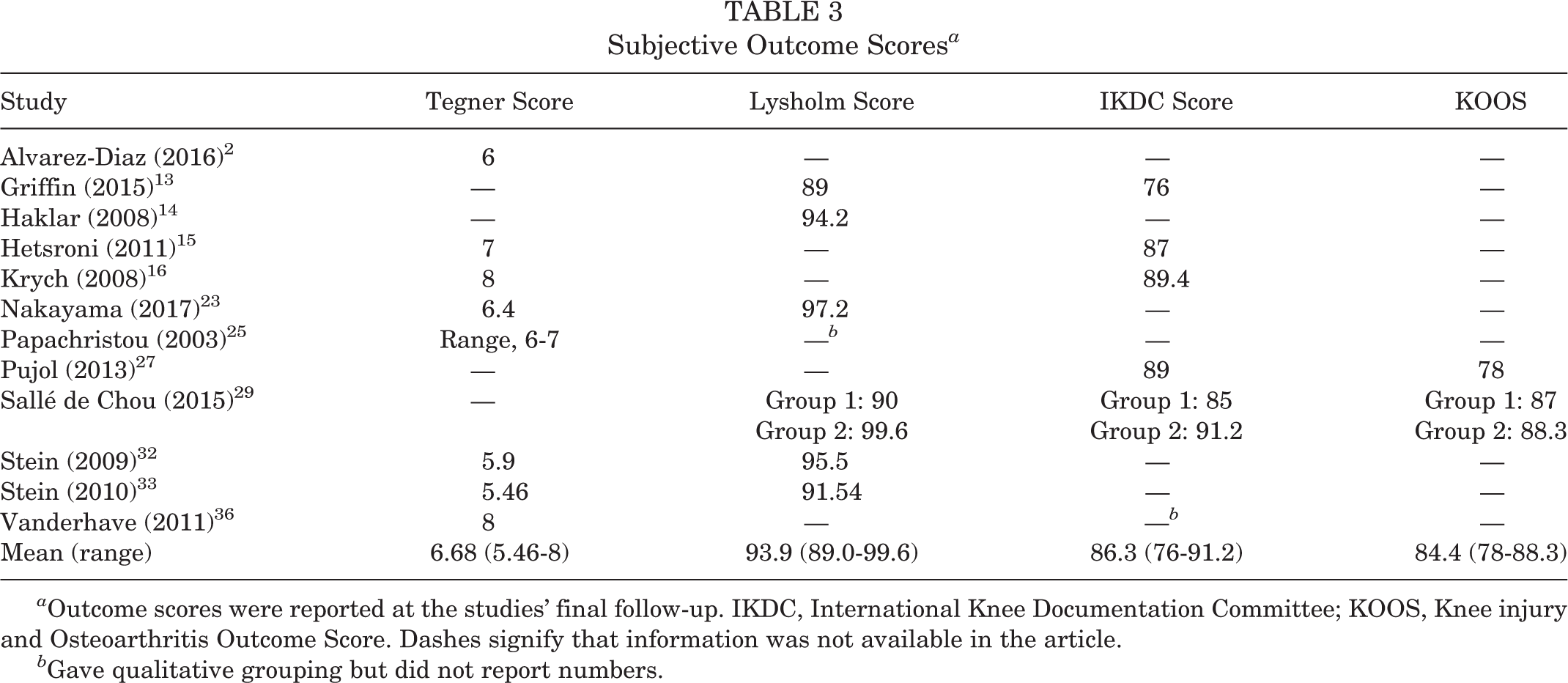
Subjective outcome scores were reported in 12 (57.1%) studies using 1 or more of the following (with the number of times that each test was utilized): Tegner score (n = 8), Lysholm score (n = 7), International Knee Documentation Committee (IKDC) score (n = 6), and Knee injury and Osteoarthritis Outcome Score (KOOS) (n = 2) (Table 3). ¶
Subjective Outcome Scores a
a Outcome scores were reported at the studies’ final follow-up. IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score. Dashes signify that information was not available in the article.
b Gave qualitative grouping but did not report numbers.
Complications
Complications were reported in 11 of the 21 (52.4%) articles, resulting in a total of 13 out of 155 (8.4%) patients who had complications after their surgery. Pujol et al 27 reported 7 total complications. One patient had a superficial cutaneous burn from the knee brace. One patient had a deep infection that was treated with antibiotics, wound lavage, and arthroscopic synovectomy; this patient had full function at follow-up. Four patients had transitory dysesthesias of the infrapatellar and sartorial branch of the saphenous nerve, and all 4 fully recovered between 9 and 12 months. The last complication was not described. 27 There were 3 separate complications reported by Sallé de Chou et al. 29 One patient had septic arthritis that required arthroscopic joint lavage and a 6-week antibiotic treatment, another patient had a deep vein thrombosis, and the third patient had persistent pain that was treated with a partial meniscectomy for retear. Stein et al 33 also reported 3 complications that occurred in patients who underwent revision surgeries, where 2 of the 3 patients’ menisci had never healed and the last patient had persistent dysesthesias in the region of the saphenous nerve.
Revision Surgery
A total of 44 (12.4%) patients required revision surgeries. # Alpar and Bilsel 1 reported that 2 menisci failed to heal after surgery, and both patients underwent subsequent partial meniscectomy. Papachristou et al 25 reported 4 patients who had a meniscal tear recurrence between 9 and 14 months after the initial surgical procedure. In all 4 patients, a partial meniscectomy was performed, and complete healing was achieved in 3 patients, with partial healing in the fourth patient. Pujol et al 27 reported 4 revision surgeries after 4 patients experienced clinical failure and had recurrent symptoms. These patients underwent a secondary meniscectomy with 3 subtotal medial meniscectomies at 18, 24, and 36 months, and the fourth patient had a partial lateral meniscectomy at 11 months with partial healing. Stein et al 33 reported 6 revision surgeries within 13 months of surgery. Three revisions were because of a new trauma, and the other 3 did not have an identifiable cause. Two of the revision surgeries were a new meniscal repair at another part of the meniscus, and the other 4 revisions were partial meniscectomies. Vanderhave et al 36 reported 1 revision surgery because of retear, and that patient underwent subsequent meniscal debridement. Nakayama et al 23 reported that 4 retears occurred between 8 and 30 months after surgery, and that 3 of the 4 patients underwent a meniscectomy, while the other patient had a second repair. Griffin et al 13 reported 5 revision surgeries. Two patients underwent partial meniscectomy because of recurrent pain, and the other 3 revision surgeries were not specified for the patients with isolated meniscal repair. Krych et al 16 reported 17 revision surgeries; 12 patients experienced failure while performing the same sport as the initial injury, 3 reinjuries happened during activities of daily living, 1 was noncompliant with postoperative restrictions, and 1 mechanism of failure was unknown. Two patients received a re-repair surgery, and the other 15 underwent partial meniscectomy. Hetsroni et al 15 reported 1 surgical failure with the all-inside arthroscopic technique when a suture pulled through the meniscus. This patient then had a revision repair with an outside-in technique.
Study Methodology Scores
The quality of the methodology/risk bias for each study was assessed using the MCMS. The overall MCMS mean was 48.64 ± 15.95 (see the Appendix). The results of our review were limited to mainly retrospective studies, as well as case reports, accounting for a lower mean MCMS.
Discussion
Isolated meniscal repairs are less common in athletes. This systematic review found that the return to play rate was high for athletes after isolated meniscal repairs. For this study, 295 out of the total 355 patients returned to sports, giving a return to play rate of 83.1%.
Eberbach et al 8 conducted a similar systematic review looking at return to play with isolated meniscal repairs and reported a comparable return to play rate of 89%. However, those authors reported on 6 articles with a total population of only 92 athletes for the specific return to play rate. In the remaining 22 articles analyzed, sports participation was evaluated via the Tegner activity scale. Our systematic review aimed to evaluate a larger patient population and only reported return to play rates based on explicit statements regarding patients returning to sport, as compared with subjective outcome scores. It should also be noted that many of the included articles did not specify if their patients returned to the preinjury level of sport or if they experienced a decrease in sport level.
As noted above, a large difference was observed in return to play rates between the different surgical techniques. The mean return to play rate was much higher for the arthroscopic technique than for the open technique. For the open technique, 69.2% of the patients returned to play, while with the arthroscopic technique, 96.1% of patients returned to play across the 16 articles. The 2 subtypes of arthroscopic techniques had very similar return to play rates of 95.5% for the all-inside technique and 91.4% for the inside-out approach. The open surgical technique is an older technique, and the 3 studies that used all open surgical techniques reported the procedures being used in 1978-1980, 6 1991, 1 and 1998-2006. 27 Although the article written by Pujol et al 27 was published more recently (in 2013), the data reported regarding the open surgical technique were from procedures performed between 1998 and 2006. Advancements in surgical techniques could help explain why the return to play rate was much higher in the patients who received arthroscopic surgery. Papachristou et al 25 reported similar results when they looked at 2 groups of patients with isolated meniscal repairs; 1 group had open repairs while the other group had arthroscopic repairs. There were 3 recurrences in the group of 15 patients who had an open repair, and there was only 1 recurrence in the group of 10 patients who had an arthroscopic repair. The difference in outcome and return to play could be explained in the study by DeHaven. 7 This study was on meniscal repairs using the open versus arthroscopic technique and found that arthroscopic surgeries were associated with reduced morbidity and earlier return to function as compared with the same surgeries performed with the open technique. Two other studies 12,38 also reported that the arthroscopic technique was initially used to decrease morbidity, and Grant et al 12 stated that arthroscopic repair can be applied to more types of meniscal tear locations, while the open technique has a more limited access to the meniscus. In addition, Grant et al 12 found clinical failure rates of 17% and 19% to be similar between inside-out and all-inside repair techniques, respectively. This article ultimately concluded that there were no significant differences in clinical failure rate or subjective outcomes between the inside-out and all-inside arthroscopic repairs. The overall decreased morbidity, increased application, and earlier return to function that patients experienced with the arthroscopic versus open technique may help explain the difference in the return to play rates that this systematic review found between these 2 surgical techniques.
Measuring the return to play rate is important for athletes, but it is also important to analyze the reasons why some athletes were not able to return to play after their surgery. Two studies provided explanations as to why select patients did not return to their preinjury level of sport. Papachristou et al 25 reported that 2 patients dropped to a lower level of sports because of pain, and an additional 4 patients were symptom-free, but at their final follow-up had abandoned soccer, handball, and running because of increased age, only participating in jogging 4 times a week. Sallé de Chou et al 29 reported that 2 patients continued to play sports, but after their surgery had to drop from their preinjury sport level for unstated reasons. Alvarez-Diaz et al 2 listed pain, personal life, and job-related reasons for why athletes stopped or reduced sport participation. However, this study did not specify whether these reasons were applicable to the patients with isolated meniscal injuries. Stein et al 32 reported that all athletes returned to their preinjury level of sport. However, Stein et al 32 also theorized that incomplete neuromuscular recovery in the quadriceps may explain why some athletes do not return to their preinjury level.
In addition to looking at reasons for why athletes were not able to return to play, we also analyzed the reason for revision surgeries. Revision surgeries were necessary in 44 of the 358 (12.3%) knees. Of these 44 revision surgeries, 35 were meniscectomies, 6 were secondary meniscal repairs, and 3 were not specified. Alvarez-Diaz et al 2 found that subsequent meniscectomies were required in 7.6% to 24% of meniscal repairs. Sallé de Chou et al 29 reported a lower failure rate of 3.7%, Eberbach et al 8 reported a failure rate of 21%, and Tucciarone et al 35 reported a 27% failure rate. This systematic review reports data that are consistent with these values. However, only 15 of the 21 (71.4%) articles discussed surgical revision. A more accurate surgical revision rate of 15.3% is generated when looking at the surgical revisions only across the surgeries in these 15 studies.
Furthermore, many studies have also concluded that isolated meniscal repairs have a higher failure rate than meniscal repairs with concomitant ACL reconstructions. 5,13,16,17,35 Krych et al 17 reported an isolated meniscal tear failure rate of 38%, while their combined meniscal repair and ACL reconstruction cohort had a 26% failure rate. Griffin et al 13 stated that the lack of meniscal vasculature providing intrinsic nutrition could help explain this discrepancy. Other studies stated that hemarthrosis generated during concomitant ACL surgery generally helped healing. 13,18,35 The lower surgical revision rate of 15.3% observed in our analysis may be attributed to a younger average patient age of 22.5 years. It has previously been reported that patients younger than 30 years of age have improved healing rates and may therefore require less surgical revisions. 9,34 As an exception to this trend, Alvarez-Diaz et al 2 found a similar return to play rate between athletes with isolated meniscal injuries and those with concomitant ACL reconstruction. Clearly, there are some conflicting results regarding these 2 groups and further investigation is needed to more accurately analyze the failure rate with isolated meniscal injuries.
This systematic review found an overall complication rate of 3.7%, which is relatively low compared with previous literature. However, only 11 of the 21 (52.4%) studies discussed complications. A more accurate complication rate of 8.4% is generated when looking at the complications across only the patients in these 11 studies. Austin and Sherman 3 found that the complication rate was 14% for isolated meniscal repairs and also reported a 20% complication rate after a meniscal repair with a concomitant ACL reconstruction. They also found that there was an 18% complication risk in patients with isolated medial meniscal repair, and zero complications were found with isolated lateral meniscal repair. These results demonstrate that the type and location of the isolated meniscal repair may affect complication rates. In this review, 17 (81.0%) articles reported whether the meniscal repairs were medial or lateral. Across these 17 studies, there were 212 (59.2%) medial meniscal repairs and 95 (26.5%) lateral meniscal repairs; however, the complication rate for medial and lateral repairs could not be individually extrapolated from the studies.
Subjective outcome scores were examined, when available, to better understand postoperative patient function (see Table 1). The mean postoperative Tegner score was 6.7 (range, 5.46-8); Lysholm score, 93.9 (range, 89.0-99.6); IKDC score, 86.3 (range, 76-91.2); and KOOS, 84.4 (range, 78-88.3). For patients with meniscal repair and simultaneous ACL reconstruction, studies have reported a mean postoperative Tegner score of 5.47, 19 Lysholm score of 93.1, 10 IKDC score of 84.2, 22 and KOOS of 45.0. 37 These values can be compared with subjective outcome scores of athletes who underwent isolated ACL reconstruction. Shervegar et al 30 did a study looking at ACL reconstructions and reported a post–ACL reconstruction Tegner score of 4.26, a mean postoperative Lysholm score of 84.4, and a mean postoperative IKDC score of 75.6. A similar study on ACL reconstructions reported a KOOS value of 51.4. 28 Vanderhave et al 36 stated that patients with ACL reconstruction had lower Tegner scores of 6.8 compared with patients with isolated meniscal tears who had a higher mean Tegner score of 8. Other studies looked at isolated meniscal repairs and reported a mean Tegner score of 6.4, 8,23 a mean Lysholm score of 97.2, 8,23 and a mean IKDC score of 81.2 at 12 months postoperatively. 35 Our values are consistent with the current literature and show that isolated meniscal repairs generally have similar or higher subjective outcome scores than meniscal repairs with concomitant ACL reconstruction or isolated ACL reconstruction. However, further research is necessary as there are exceptions to this trend. Martin-Fuentes et al 19 found that the Lysholm and Tegner scores were 88.6 and 4.53 for patients with isolated meniscal repairs, respectively, and 88.0 and 5.47 for patients with meniscal repair and ACL reconstruction, respectively.
The evidence in this systematic review should be interpreted with caution because of several limitations. First, a smaller number of studies and patients could affect the strength and application of the results. However, because the literature on isolated meniscal repairs is so sparse, a systematic review is the best way to present significant data and draw conclusions. Another potential limitation of this study is the overall poor quality of the studies as measured by the MCMS score, which was a mean of 48.64. The overall average was heavily influenced by the lower number of case studies that were included, as 7 of the total 21 (33.3%) 4,11,20,21,24,26,31 articles included are case studies. Because of the limited number of studies reporting, 12 (57.1%) on the specific sport played, and the large number of sports reported, we were not able to draw associations between sports type and the return to sports rate. This is an important area that needs to be addressed and should be a focus of future studies on this topic. This further highlights the limited literature related to isolated meniscal repairs. Regardless of the limited research, the included studies are diverse with varying sports and patient characteristics, which helped to improve the generalizability of these findings.
Conclusion
Patients with an arthroscopic meniscal repair had a higher chance of and faster return to play than those with an open repair. Isolated meniscal repairs may result in more surgical revisions, decreased complications, and higher subjective outcome scores than meniscal repairs with concomitant ACL reconstruction. However, the limited number of studies, particularly higher-level studies with larger patient numbers, highlights the need for further investigation regarding isolated meniscal repair in athletes.
Footnotes
Notes
Final revision submitted April 14, 2020; accepted May 7, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.D.W. has received educational support from Liberty Surgical, Smith & Nephew, Arthrex, and Medical Device Business Services. W.E. has received educational support from Liberty Surgical. S.B.C. has received speaking fees and consulting fees from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Appendix
Full Search Using EMBASE, PubMed, and Cochrane Databases
| EMBASE | PubMed |
| 1. ‘menisc* repair’ | 1. Menisc* repair |
| 2. ‘menisc* repair’: ti,ab | 2. Meniscus |
| 3. ‘meniscus’ | 3. OR/1-2 |
| 4. ‘meniscus’: ti, ab | 4. “Knee” [Mesh Terms] |
| 5. OR/1-4 | 5. Knee* |
| 6. Knee/exp | 6. “Knee Joint” [Mesh Terms] |
| 7. Knee*:ti,ab | 7. Femorotibia* |
| 8. ‘Knee joint’/exp | 8. OR/4-7 |
| 9. Femorotibia*:ti,ab | 9. 3 AND 8 |
| 10. OR/6-9 | 10. Repair [Mesh Terms] |
| 11. 5 AND 10 | 11. Repair* |
| 12. Repair/exp | 12. Surgery [Mesh Terms] |
| 13. Repair*: ti,ab | 13. Surger* |
| 14. Surgery/exp | 14. Rehabilitation [Mesh Terms] |
| 15. Surger*: ti,ab | 15. Rehabilitation* |
| 16. Rehabilitation/exp | 16. “Return to” |
| 17. Rehabilitation*: ti,ab | 17. “Objective protocol*” |
| 18. ‘Return to’ | 18. OR/10-17 |
| 19. ‘Return to’:ti,ab | 19. 9 AND 18 |
| 20. ‘Objective protocol*’ | 20. Randomized Controlled Trial [Publication Type] |
| 21. ‘Objective protocol*’: ti,ab | 21. Randomized controlled trial |
| 22. OR/12-21 | 22. Controlled clinical trial [Publication Type] |
| 23. 11 AND 22 | 23. Double blind method |
| 24. (random* OR placebo*):ti,ab | 24. Single blind method |
| 25. ((singl* OR doubl* OR tripl*) AND (blind* OR mask*)) :ti,ab | 25. Clinical trial [Publication Type] |
| 26. Controlled clinical trial*:ti,ab | 26. Clinical trial |
| 27. Controlled clinical trial [controlled clinical trial]/lim | 27. (singl* OR doubl* OR tripl*) AND (mask* OR blind*) |
| 28. Randomized controlled trial [randomized controlled trial]/lim | 28. Placebo* |
| 29. ‘Comparative study’/exp | 29. Random* |
| 30. Comparative study: ti,ab | 30. Research design [Mesh Terms] |
| 31. Case series: ti,ab | 31. Comparative study [Publication Type] |
| 32. ‘Case series’/exp | 32. Comparative study |
| 33. ‘Prospective studies’/exp | 33. Evaluation studies [Publication Type] |
| 34. Prospective studies: ti,ab | 34. Evaluation study |
| 35. Placebo* | 35. Follow-up studies |
| 36. OR/24-35 | 36. Follow-up study |
| 37. 23 AND 36 | 37. Prospective studies |
| 38. ACL | 38. Prospective study |
| 39. anterior cruciate ligament | 39. Control* |
| 40. ‘anterior cruciate ligament’:ti,ab | 40. Prospectiv* |
| 41. (meniscectomy) NOT ‘repair’:ti,ab | 41. Case studies |
| 42. Reconstruction | 42. Case study |
| 43. Discoid | 43. OR/20-42 |
| 44. Transplant* | 44. 19 AND 43 |
| 45. ‘Systematic review‘:ti,ab | 45. English[language] |
| 46. revision | 46. 44 AND 45 |
| 47. OR/38-46 | 47. (“animals” [Mesh] NOT “humans” [Mesh]) |
| 48. 37 NOT 47 | 48. ACL |
| Total results: 321 | 49. anterior cruciate ligament |
| 50. anterior cruciate ligament[Title/Abstract] | |
| 51. (meniscectomy) NOT repair[Title/Abstract] | |
| 52. Reconstruction |
|
| PubMed search: 1082 | |
| Cochrane | Cochrane |
| 1. Menisc* repair | 14. OR/9-13 |
| 2. meniscus | 15. 8 AND 14 |
| 3. OR/1-2 | 16. ACL |
| 4. Knee | 17. anterior cruciate ligament |
| 5. ‘Knee joint’ | 18. (meniscectomy) NOT ‘repair’ |
| 6. Femorotibia* | 19. Reconstruction |
| 7. OR/4-6 | 20. Discoid |
| 8. 3 AND 7 | 21. Transplant* |
| 9. Repair* | 22. ‘Systematic review’ |
| 10. Surger* | 23. revision |
| 11. Rehabilitation* | 24. OR/16-23 |
| 12. ‘Return to’ | 25. 15 NOT 24 |
| 13. ‘Objective protocol*’ | 81 articles in trials |