
Abstract
Purpose
To evaluate the preoperative deterioration of an isolated meniscal tear in patients aged 40 years or older, and whether time from injury to surgery is associated with worsening of a meniscal tear.
Methods
Patients aged 40 years or older who underwent arthroscopic surgery for isolated meniscal tear between 2014 and 2019 were retrospectively reviewed. The diagnostic magnetic resonance imaging (MRI) findings and arthroscopic findings were compared to evaluate the deterioration of meniscal tears. Predictors of the development of meniscal tears; patient demographic factors, duration from injury to surgery (injury to MRI and MRI to surgery), and image findings were assessed.
Results
A total of 58 patients (58 knees) were included (mean age, 55.9 ± 8.5 years; male/female, 31/27). An isolated meniscal tear deteriorated in 28 (48.3%). Compared patients with and without deteriorated meniscal tear, significant differences were found in the MRI grade of meniscal tear (p = 0.03), duration from injury to MRI (164.2 ± 167.9 vs 45.2 ± 48.7 days, p < 0.001), and from MRI to surgery (148.8 ± 91.1 vs 67.6 ± 56.7 days, p < 0.001). A multivariate regression analysis showed that the duration from injury to MRI (odds ratio [OR], 1.03; p < 0.001) and from MRI to surgery (OR, 1.02; p < 0.001) were independent predictors.
Conclusion
Approximately 50% of isolated meniscal tears deteriorated preoperatively in patients aged 40 years or older. The duration from injury to surgery was an independent predictor of worsening of an isolated meniscal tear.
Introduction
A meniscal tear is the most common knee injury,1,2 with an incidence of 23.8/100,000 per year. 1 Meniscal injury is often associated with knee ligamentous injuries, such as anterior cruciate ligament (ACL) injury.3–5 Numerous studies have reported that there is a high risk of worsening or newly developing meniscal injuries in cases of ACL-deficient knee because of the anterior and rotational instability of the knee.5–8 Stone et al. 9 reported that delayed ACL reconstruction (ACLR) for more than 1 year was associated with an increased risk of medial meniscal injury (odds ratio, 3.47; p < 0.002). ACLR should be performed within 3 months to prevent subsequent meniscal injuries, according to a recent systematic review. 8 However, to the best of our knowledge, no studies have evaluated whether or not an isolated meniscal tear deteriorates when surgery is delayed. Evidence regarding the association between the duration from injury to surgery and worsening of the isolated meniscal tear, is scarce. To prevent deleterious effects of meniscectomy on the development of osteoarthritis (OA), the “meniscus preservation concept” has been mentioned.10,11 It was reported that 320% increase of the meniscal repair was found while 21.4% reduction of the meniscectomy, from 2005 to 2017 in France. 12 A similar trend in meniscal surgeries in the United States was also reported. 13 In the previous studies, less favorable outcomes of meniscal repair were reported in the older population.14,15 However, Poland et al. showed that an age >40 years old was not associated with an increased risk of meniscal repair failure at 5 years after surgery, 16 which was supported by a systematic review by Everhart et al. 17 Considering the increased number of aged populations all over the world, further studies are needed for this cohort.
A recent systematic review reported that a short time from injury to surgery, Outerbridge scores below grade 3 were significant predictors of better patient-reported outcome measures (PROMs) after arthroscopic meniscal repair. 18 However, the majority of the included studies (78%) were level 4 case series, that were unable to draw a definitive conclusion regarding predictors for better results after arthroscopic meniscal repair. In order to achieve more favorable clinical results following meniscal repair for older patients as well as young patients, it may be valuable to clarify the preoperative factors associated with worsening of an isolated meniscal tear at the time of surgery. Some authors have reported that acutely repaired meniscus tears obtained superior results compared to chronically repaired tears.19–21 However, it remains unclear why acutely repaired tears result in better outcomes. It was hypothesized that delayed surgery may result in the deterioration of an isolated meniscal tear before surgery. Especially in the aged population, preoperative deterioration of meniscal tear would occur due to poor quality and vascularity of the meniscus.22,23 If an isolated meniscal tear develops before surgery, it may affect the surgical procedures and postoperative clinical outcomes. The present study was performed to answer the following two questions by comparing the findings of magnetic resonance imaging (MRI) that was performed as a diagnostic examination, and the arthroscopic findings at surgery: (1) “Does an isolated meniscal injury deteriorate between the injury and surgery in patients aged 40 years old or older ? ”, and (2) “If an isolated meniscal tear deteriorates preoperatively, is the duration from injury to surgery associated with worsening of the meniscal tear ? ”
Patients and methods
A single institutional retrospective analysis of prospectively collected data was performed. Institutional review board approval was obtained before the initiation of data collection (Approval No. O-0817). All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Declaration of Helsinki of 1975, as revised in 2013. From January 2014 to December 2019, patients
The evaluation of the MRI findings
The findings of MRI that were performed as a diagnostic examination of the meniscal tear were evaluated by two of the authors who are consultant orthopaedic surgeons, and have been involved in knee arthroscopic surgeries for more than 10 years. Both examiners were blinded to the patient information. The side (medial meniscus, MM vs. lateral meniscus, LM, or bilateral menisci), segment (anterior horn, middle horn, posterior horn, anterior or posterior roots), and grade of the affected meniscus were evaluated. The grade of the meniscal tear was documented according to the classification by Guenther et al. 27 Due to this classification system, meniscal injuries were graded on a scale from 1 to 4: grade 1, trivial tear, very short, peripheral; grade 2, substantial tear but undisplaced; grade 3, displaced portion or involvement of meniscal root; and grade 4, bucket handle meniscal tear. The two raters independently assessed the MRI findings. In the case of discrepancy in the assessment of the grade of meniscal injury between the examiners, a third senior orthopaedic surgeon resolved it.
The evaluation of the arthroscopic findings
All meniscal surgeries were arthroscopically performed with the patient in the supine position by one of four experienced arthroscopists who are specialized in knee arthroscopic surgeries. A tourniquet was applied over the operated thigh at an average of 250mmHg. The arthroscopic diagnosis was made using an 30° arthroscope via standard anterolateral and anteromedial portals. Information regarding the site, segment, and grade of the meniscal tear, as mentioned above in the section on the evaluation of MRI findings, was obtained from the operative records and arthroscopic videos.
Deterioration of the isolated meniscal tear
The MRI findings and arthroscopic findings at surgery were compared to evaluate the deterioration of the isolated meniscal tear. In addition to the grading system by Guenther et al., 27 enlargement of the meniscal tear was evaluated by comparing the involved segment of the tear between the MRI findings and arthroscopic findings. Patients were classified into two groups depending on the results: Group A, patients whose grade and segment of the meniscal tear had not change by surgery; Group B, patients whose meniscal tear had deteriorated by surgery. The deterioration of the meniscal tear was defined as (1) progressed grade of the meniscal tear at surgery, (2) enlargement of the meniscal tear at surgery and (3) newly identified tears at surgery in addition to the lesions on MRI.
Statistical analysis
All statistical analyses were performed using the SAS software program (JMP Pro ver. 15.2.0; SAS Institute, Cary, NC, USA). Descriptive statistics are presented for both group (subjects with and without worsening of the meniscal tear) in the form of the number of occurrences and percentage or as the mean, standard deviation (SD), and extrema. p values less than 0.05 were considered significant. The Shapiro-Wilk method was used to test whether or not the data were normally distributed. Student t tests were performed for continuous variables when the data showed a normal distribution, otherwise, the Mann-Whitney U test was performed. The categorial variables were compared using the Chi-square or Fisher’s exact test. All tests were two-tailed. Variables included in the bivariate analyses were the sex, age, BMI, injury mechanism, Tegner activity scale before the injury, side of the affected knee, duration from injury to MRI (days), duration from MRI to surgery (days), KL grade, and the side (MM vs. LM vs. bilateral menisci) and MRI grade of the meniscal tear. A logistic regression analysis was performed to assess the impact of potential predictors on the deterioration of the isolated meniscal tear. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Finally, Spearman’s rank correlation coefficient was used to assess the relationship between (1) the duration from injury to MRI and continuous variables, and (2) the duration from MRI to surgery and continuous variables. The strength of the correlation of the rank coefficients was defined as follows: strong, 0.70–1.0; moderate, 0.40–0.69; weak, 0.20–0.39. 28 The relationship between the duration from injury to surgery (injury to MRI and MRI to surgery) and categorial variables was evaluated using the Student t test or Mann-Whitney U test.
Results
A total of 75 patients who underwent arthroscopic surgery for an isolated meniscal tear were identified in the study period. Of these patients, 17 were excluded for the following reasons: discoid meniscus (n = 5), history of the knee surgery (n = 10), and revision surgery of the meniscus tear (n = 2). As a result, a total of 58 patients (58 knees) were finally included and evaluated in this study. The arthroscopic evaluation did not identify any ligamentous injuries, such as ACL or posterior cruciate ligament (PCL) injuries. The mean age of the sample population was 55.9 ± 8.5 (range, 40–81) years old, and males were 31 (53.4%). The mean BMI was 25.5 ± 4.6 (range, 19.5–40.1) kg/m2. The side of the injured knee was right in 31 (53.4%), and no patient injured both sides. The KL grade were 1 in 23 (39.7%), and 2 in 35 (60.3%). The mean time from injury to MRI was 102.6 ± 134.8 (range, 1–727) days, and that from MRI to surgery was 106.8 ± 85.1 (range, 7–365) days.
Deterioration of the isolated meniscal tear
Details of the MRI findings and arthroscopic findings.
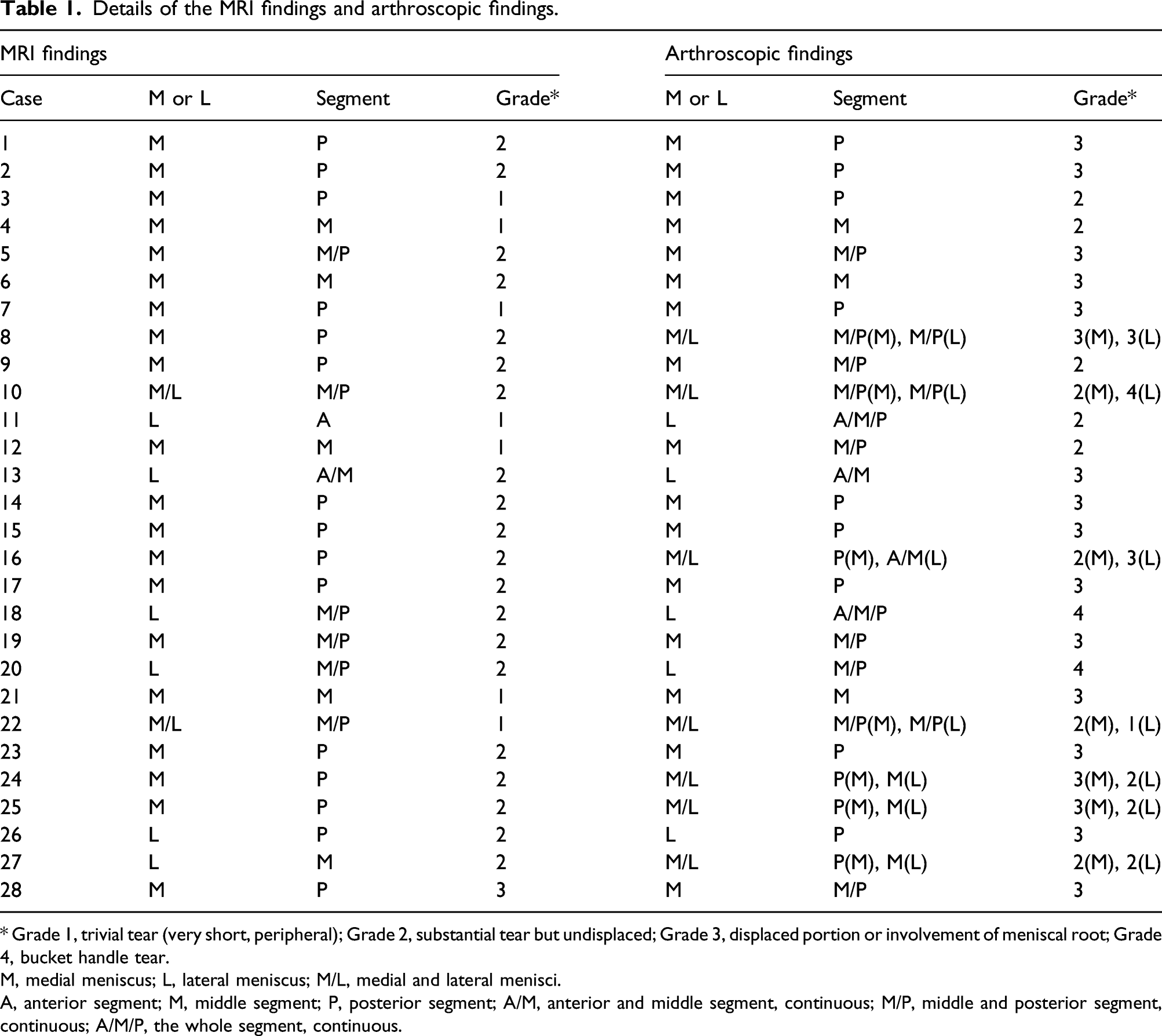
* Grade 1, trivial tear (very short, peripheral); Grade 2, substantial tear but undisplaced; Grade 3, displaced portion or involvement of meniscal root; Grade 4, bucket handle tear.
M, medial meniscus; L, lateral meniscus; M/L, medial and lateral menisci.
A, anterior segment; M, middle segment; P, posterior segment; A/M, anterior and middle segment, continuous; M/P, middle and posterior segment, continuous; A/M/P, the whole segment, continuous.
Comparison of patients with and without the deterioration of the isolated meniscal tear.

Age, BMI, Tegner activity scale, duration from injury to MRI and that from MRI to surgery are shown as mean ± standard deviation.
Other variables are shown as a number and percentage in the parenthesis.
BMI, body mass index; MRI, magnetic resonance imaging.
Bold shows statistically significant (p < 0.05).
Multivariate analysis of the predictors for deterioration of the isolated meniscal tear.

B, regression coefficient; SE, standard error; OR, odds ratio; 95% CI, 95% confidence interval.
MRI, magnetic resonance imaging.
Correlation between the duration from injury to surgery and included variables
Correlations between the duration from injury to surgery (injury to MRI and MRI to surgery) and variables.

BMI, body mass index; MRI, magnetic resonance imaging; N/A, not applicable.
Values are shown as mean ± standard deviation.
MRI, magnetic resonance imaging.
There were no significant associations between the duration from injury to surgery (injury to MRI and MRI to surgery) and evaluated categorial variables (Table 4-B).
Discussion
The most important findings of the present study were that an isolated meniscal tear deteriorated from the injury to surgery in 48.3% (28/58) of patients
Many previous studies have demonstrated an increased incidence of meniscal tears with delayed ACLR in pediatric and adult patients.5–9,27,29,30 Recurrent episodes of instability in the ACL-deficient knee could cause displacement or enlargement of the already-torn meniscus.
31
However, in the present study the deterioration of the meniscal tear was confirmed in nearly one-third of the patients with ACL-intact knees. Many authors have demonstrated the role of the meniscus, especially the medial meniscus, as an important restraint for anterior tibial translation in the ACL-deficient knee.32,33 However, the influence of isolated meniscal tear on knee stability still remains controversial, because few studies have investigated this issue. It was reported that a meniscal tear developed during screw-home mechanism (0–30° flexion) and ascent from a squatting position (120-60° flexion).
34
Kedgley et al.
35
showed that the stress distribution on the meniscal tear surface under weight-bearing differed depending on the tear pattern and tear location, according to a finite element analysis. They showed that differences in the stresses across the tear surfaces were greater for the LM than for the MM in longitudinal tear samples. In addition, they found that only the posterior segment of the LM was compressed throughout the range of knee flexion (0–30°). In the present study, there was not significant difference in the rate of worsening of the tear of the MM or LM between the Group A and Group B (p = 0.22). The deterioration of the meniscal tear in our study was assessed using the grading system reported by Guenther et al.
27
This grading method did not consider the morphology of the meniscal tear. Furthermore, the majority of tear locations in this study population were in the middle to posterior segments of the meniscus. Therefore, the influence of the morphology and/or location of the tear on the development of isolated meniscal tear was not evaluated in this study. However, the present study was the first, to the best of our knowledge, to evaluate the development of an isolated meniscal tear from injury to surgery in the clinical setting, demonstrating the worsening of the tear in a half of patients
In the treatment for an isolated meniscal tear, conservative or surgical treatment is selected depending on the clinical setting. Many factors, such as tear stability, length, morphology, segment and vascularity were reported to be considered for the suitability of conservative treatment. 37 If conservative treatments fail, preservation of the meniscus, by meniscal repair or left in situ, is recommended as the clinical and radiological outcomes are worse after partial meniscectomy.10,11,38 Based on the 2019 European Society for Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA) meniscus consensus, preservation of the meniscus should be the first line of treatment whenever possible, regardless of the age, BMI, tear size, or tear location. 38 Several authors demonstrated favorable clinical results of meniscal repair performed in patients who were 40 years and older.16,17,21 However, patient’s age and radiographic findings (KL grade) could become a bias to clinicians when evaluating the cause of knee pain, which may result in a delayed decision to perform MRI to evaluate meniscal tears in middle-aged or elderly patients with radiographically OA knee. However, Englund et al. 39 reported that meniscal tears on knee MRI were detected in 35% of persons >50 years old, and two-thirds of those tears were asymptomatic. Therefore, it is not appropriate to make a diagnosis of a meniscal tear in aged patients using only MRI findings.24,25 All patients in the present study had a history of the sudden onset of knee pain, and individuals whose onset of meniscal tear could not be identified were not included in order to exclude cases of incidental meniscal tears detected on MRI. With increased age, the vascular supply to the meniscus is decreased. 22 Furthermore, the meniscus of patients with OA knee is more degenerative and sensitive to minor injury than in patients without OA knee, implying more easily worsening of the tear after an injury in OA knee patients. In order to prevent the development of meniscal tear after the injury, it is recommended to consider performing MRI at an early stage in middle-aged or elderly patients suspected of having a traumatic meniscal tear. This will decrease the rate of worsening of the meniscal tear, which may lead to better clinical results after meniscal repair in such populations. The avoidance of preoperative deterioration of the meniscal tear may result in performing meniscal repair rather than meniscectomy. However, the purpose of the present study was to evaluate whether or not an isolated meniscal tear deteriorates before surgery, and it was beyond the scope of this study to assess the differences in surgical outcomes or procedures between subjects with and without worsening of the meniscal tear at surgery. Further prospective studies will be required to investigate the influence of preoperative deterioration of the meniscal tear on surgical procedures and surgical results.
The current study has several limitations. First, patients who did not undergo surgery were not evaluated in this study. Therefore, the presence or absence of worsening of an isolated meniscal tear in patients treated conservatively could not be described. Second, MRI is the most commonly performed diagnostic imaging modality in the diagnosis of meniscal tear. 40 However, the sensitivity and specificity of MRI for medial meniscal tear are 89% (95% CI, 83%–94%) and 88% (95% CI, 82%–93%), respectively, and those for the lateral meniscal are 78% (95% CI, 66%–87%) and 95% (95% CI, 91%–97%), respectively. 41 Therefore, the accuracy of the evaluation of meniscal tear by MRI could affect the results of the present study. Third, as mentioned in the discussion, the grading system of the meniscal tear used in this study was unable to evaluate the morphology of the tear. Furthermore, the length of the meniscal tear was not evaluated using a probe at surgery. Therefore, the detailed measurement of the tear length was not performed. Fourth, due to the retrospective study design, the patient activities from the injury to surgery were not completely evaluated. However, all subjects had knee pain that limited their preoperative activity level, therefore the activity level was not high. Fifth, this study evaluated risk factors for preoperative worsening of isolated meniscal tears in patients aged 40 years or older. Therefore, an different cutoff age of the older group (>50 years or >60 years) may show different results. Finally, young patients and patients with severe OA-knee (KL 3 or KL 4) were not identified in the study population. Therefore, preoperative worsening of meniscal tears in these cohorts was not evaluated.
Conclusions
Approximately 50% of isolated meniscal tears deteriorated preoperatively in patients aged 40 years and older. The durations from injury to MRI and from MRI to surgery were independent predictors of the worsening of isolated meniscal tear at surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Miyazaki University Hospital (A research grant in 2021).