
Abstract
Background:
Retear of a repaired rotator cuff tendon is a major issue for shoulder surgeons. It is possible that diabetes mellitus (DM) is associated with a greater risk of tendon retear after arthroscopic rotator cuff repair.
Purpose:
To determine whether patients with DM have a higher tendon retear risk after arthroscopic rotator cuff repair.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was conducted following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines using the Web of Science, PubMed, and Embase databases. Inclusion criteria were articles written in the English language that included patients undergoing arthroscopic rotator cuff repair surgeries, reported the numbers of patients with and those without DM, and reported the number of rotator cuff retears. Data relevant to this study were extracted and statistically analyzed. Random-effects models were used to generate pooled odds ratio estimates and CIs.
Results:
A total of 160 studies were identified from the initial search, and 5 of them met the inclusion criteria. A total of 1065 patients (207 patients with DM and 858 patients without DM) were included. The pooled results showed that the patients in the DM group had a significantly higher tendon retear risk than did those in the non-DM group (relative risk, 2.25; 95% CI, 1.14-4.45; P = .02).
Conclusion:
Patients with DM have a 2.25 times higher risk of tendon retear after arthroscopic rotator cuff repair compared with patients without DM.
Retear of a repaired rotator cuff tendon, a common complication after rotator cuff repair, has become a major concern of shoulder surgeons. 9 In addition to the patient age and the size of the tear, 12,17 several preoperative parameters have been proven to be associated with increased retear risk after rotator cuff repair, including a higher critical shoulder angle, 18,19 a higher acromion index, 18 a smaller acromion index, 18,20 a greater degree of tendon retraction, 11,20 the severity of fatty infiltration, 9,12 and the supraspinatus occupation ratio. 9,11
Diabetes mellitus (DM) is one of the most common and debilitating medical conditions. 5 It potentially impairs connective tissue healing and reduces tissue biomechanical properties. 1 Previous studies have shown the regenerative capability of tendons to be compromised in patients with diabetes because of less fibroblast proliferation and lymphocyte infiltration in healing tendons associated with tendon weakness. 1,3,6 An animal study indicated that DM impairs tendon-bone healing after rotator cuff repair. 2 Several clinical studies have further investigated the relationship between DM and retearing of the rotator cuff tendon. 5,9 –11,14 Some clinical studies have reported significantly higher retear rates of repaired rotator cuff tendon in patients with DM. 5,10 However, the findings of other studies have not supported DM as a risk factor for tendon retear after arthroscopic rotator cuff repair. 9,11,14
Owing to the inconclusive findings associating DM with tendon retear risk after arthroscopic rotator cuff repair, the purpose of this meta-analysis was to determine whether patients with DM have a higher risk of tendon retear after arthroscopic rotator cuff repair. We hypothesized that this would be the case according to the studies reviewed.
Methods
The current meta-analysis was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 15
Search Strategy and Study Selection
A systematic review of the literature was conducted using the Web of Science, PubMed, and Embase databases up to February 1, 2020. The keyword search consisted of the following terms: “diabetes mellitus,” “hyperglycemia,” “rotator cuff,” “tear,” and “retear.” Articles that met the following criteria were included: they were written in the English language, included patients undergoing arthroscopic rotator cuff repair surgeries, reported the number of patients with and those without DM, and reported the number of rotator cuff retears. Articles that did not meet these inclusion criteria or were animal studies or review articles were excluded. The search of articles was performed independently and manually by different authors (C.-K.H, C.-J.C.). After removing duplicates, all titles and abstracts of the remaining citations were screened carefully. The full text of studies that met the inclusion criteria was then reviewed. When discrepancies occurred, consensus was reached via discussion with the review team (F.-C.K., K.-L.H., Y.C.). The quality of each article was assessed by using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 23
Data Extraction
Two authors (C.-K.H., C.-J.C.) independently extracted the data from the articles. The following data were extracted from the included articles: (1) patient characteristics, (2) the timing for postoperative magnetic resonance imaging (MRI), (3) the number of patients with and those without DM, and (4) the number of rotator cuff retears (Sugaya type 4 or 5) 22 on postoperative MRI scans in each subgroup. If more data or missing data were needed for meta-analysis, the authors of these published articles were contacted.
Data Synthesis
The Mantel-Haenszel method was used for the purpose of analyzing the outcomes. The effect of heterogeneity was evaluated using I 2. 7 The I 2 value ranged from 0% to 100%. A fixed-effects model was used when I 2 < 50%, indicating low to moderate heterogeneity. In contrast, a random-effects model was used if the heterogeneity was high (I 2 > 50%). We calculated the heterogeneity and relative risk (RR) for the desired outcome in this meta-analysis. A forest plot was generated to illustrate the RR. Along with the RRs, 95% CIs were determined. The possibility of publication bias was assessed using Egger funnel plots. 21 This meta-analysis was conducted using Review Manager Version 5.3 software (The Nordic Cochrane Centre; The Cochrane Collaboration). A P value of .05 was considered statistically significant.
Results
Search Results
In total, 160 studies were identified using our search strategy in 3 databases. After removing duplicates, 85 studies remained, and 8 of them were deemed appropriate for full-text screening after initial screening of the title and abstract. The full texts of 8 articles were reviewed, and 5 articles were identified and included in the meta-analysis after applying the inclusion and exclusion criteria. The results of the literature search are displayed in Figure 1. The included articles fit 19 to 21 out of 22 items in the STROBE statement.

Flow diagram for study selection following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Five studies 5,9 –11,14 met the inclusion criteria, and a total of 1065 patients (559 men [52.5%] and 506 women [47.5%]) were included. The DM group had 207 patients, among whom 70 patients (33.8%) had a tendon retear after rotator cuff repair surgeries. The non-DM group had 858 patients, among whom 134 patients (15.6%) had a rotator cuff tendon retear. The timing for postoperative MRI ranged from 3 months to 2 years. All included patients had full-thickness rotator cuff tears preoperatively, and the majority of patients had medium- to large-sized tears (Table 1).
Meta-analysis Results for Individual Studies a
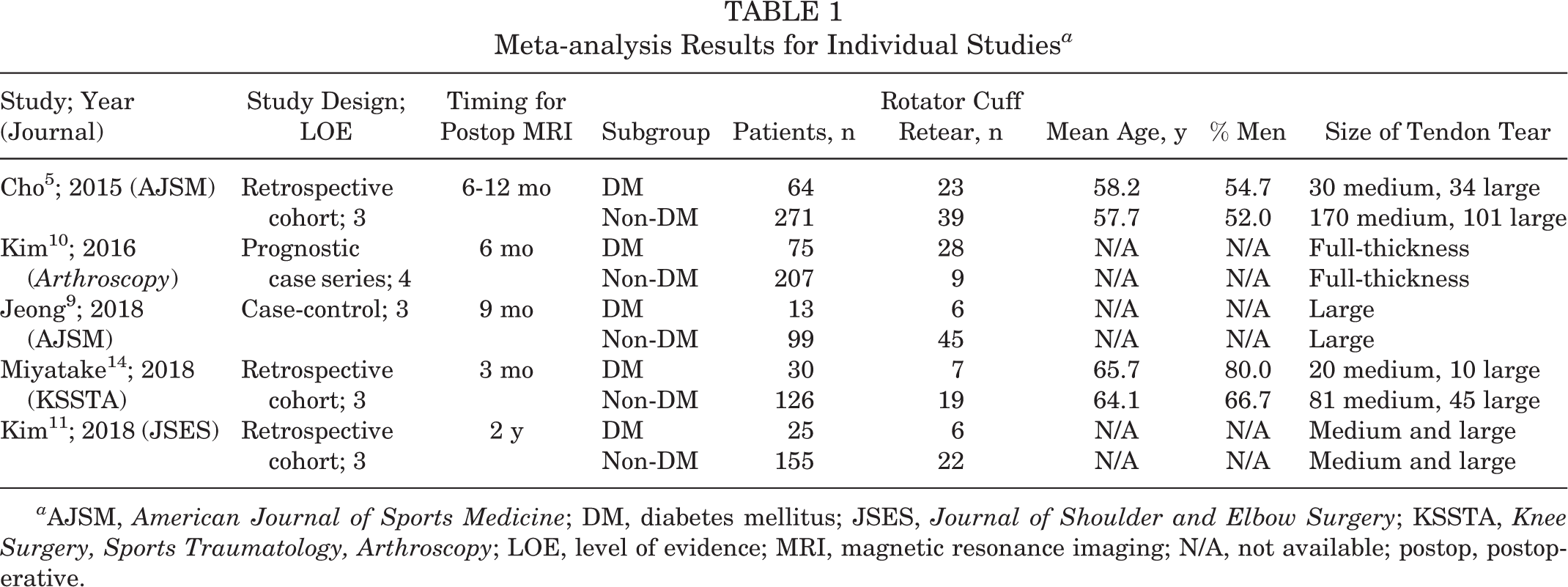
a AJSM, American Journal of Sports Medicine; DM, diabetes mellitus; JSES, Journal of Shoulder and Elbow Surgery; KSSTA, Knee Surgery, Sports Traumatology, Arthroscopy; LOE, level of evidence; MRI, magnetic resonance imaging; N/A, not available; postop, postoperative.
Pooled Risk for Rotator Cuff Retear
All included studies 5,9 –11,14 reported the number of patients with and those without DM, as well as the number of patients with tendon retear after arthroscopic rotator cuff repair surgeries. The data were pooled, and the RR was calculated for tendon retear between the DM and non-DM groups. The random-effects model was applied because evidence of heterogeneity was found among studies (τ2 = 0.49; I 2 = 82%; P = .0002). The pooled results showed that patients in the DM group had a significantly higher tendon retear risk than those in the non-DM group (RR, 2.25; 95% CI, 1.14-4.45; P = .02). A forest plot of patients with DM versus those without DM is illustrated in Figure 2. Egger funnel plots in this meta-analysis showed symmetrical distribution (Figure 3), indicating low publication bias.
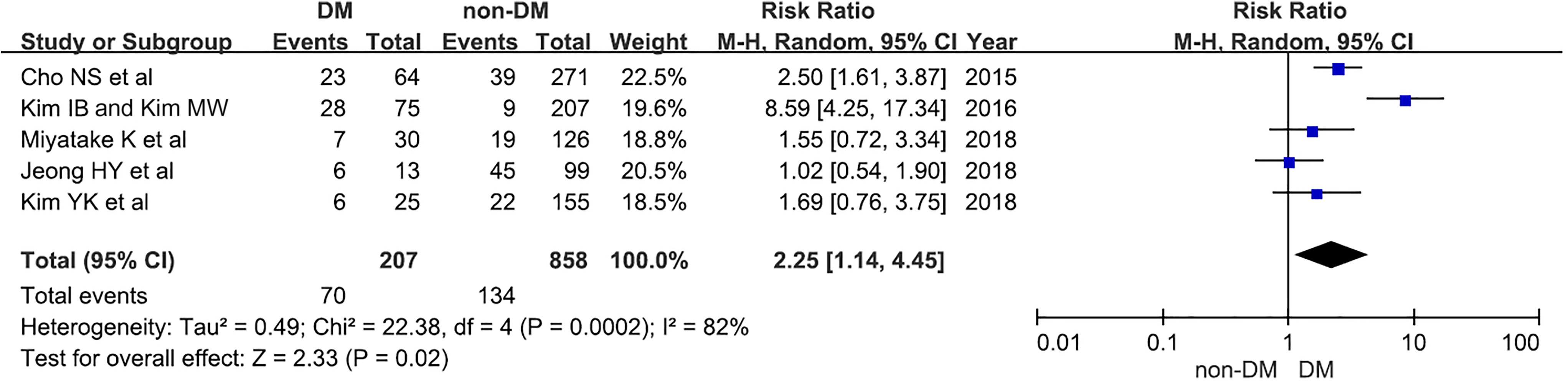
Forest plot for the relative risks when comparing tendon retear risk in patients with and those without DM. DM, diabetes mellitus; M-H, Mantel-Haenszel.

Egger funnel plots used in this meta-analysis. SE was used for the vertical axis, whereas relative risk (RR; log scale) was used for the horizontal axis.
Two included studies 5,14 reported the number of patients with controlled DM and those with uncontrolled DM, as well as the number of patients with tendon retear after arthroscopic rotator cuff repair surgeries. Both studies assigned patients with diabetes with ≥7% preoperative serum glycosylated hemoglobin to the uncontrolled DM group, whereas those with <7% preoperative serum glycosylated hemoglobin were assigned to the controlled DM group. 1,5 The fixed-effects model was utilized because no evidence of heterogeneity was found among studies (χ2 = 0.00; I 2 = 0%; P = .95). The pooled results showed that the patients with uncontrolled DM had a higher tendon retear risk than did the patients with controlled DM (RR, 1.69; 95% CI, 0.89-3.21; P = .11), but the result did not reach a significant difference. A forest plot of patients with controlled DM versus those with uncontrolled DM is illustrated in Figure 4.

Forest plot for the relative risks when comparing tendon retear risk in patients with controlled diabetes mellitus (DM) and those with uncontrolled DM. M-H, Mantel-Haenszel.
Two included studies 5,14 that reported the number of patients with controlled DM and those with uncontrolled DM, as well as the number of patients with tendon retear after arthroscopic rotator cuff repair surgeries, were further analyzed. The fixed-effects model was utilized because no evidence of heterogeneity was found among studies (χ2 = 0.42; I 2 = 0%; P = .52). The pooled results showed that the patients with controlled DM had a higher tendon retear risk than did the patients without DM (RR, 1.56; 95% CI, 0.86-2.81; P = .14), but the result did not reach a significant difference. A forest plot of patients with controlled DM versus those with uncontrolled DM is illustrated in Figure 5.

Forest plot for the relative risks when comparing tendon retear risk in patients with uncontrolled diabetes mellitus (DM) and those with controlled DM. M-H, Mantel-Haenszel.
Discussion
The major finding of this meta-analysis is that patients with DM had a 2.25 times increased risk of tendon retear after arthroscopic rotator cuff repair compared with patients without DM. Retear of a repaired rotator cuff tendon is an important concern for shoulder surgeons. 9 Many factors contribute to the healing rate of repaired rotator cuff tendons, 9,11 –13,16 –18,20 and DM is one of them. However, the effect of DM on tendon retear after rotator cuff repair has been a subject of debate. 5,9 –11,14 Because of the inconclusive findings in previous studies, 5,9 –11,14 this meta-analysis was aimed toward determining whether patients with DM have higher risk of tendon retear after arthroscopic rotator cuff repair.
DM, a disorder characterized by persistent hyperglycemia, may adversely influence tendon quality and delay the tendon healing process by affecting a variety of intrinsic factors. 1 Compared with the healing process in normal tissues, DM is often associated with reduced collagen synthesis, abnormal cytokine production, and compromised angiogenic and growth factor production. 3,6 Thus, the healing process of damaged tissues in patients with DM is impeded. 3,6 In addition to the obstruction of the tendon healing process, DM also alters the quality of tendons, 4 possibly leading to an increased risk of rotator cuff tears. 8 Given that both the quality of the tendon and the process of tendon healing are affected by hyperglycemia, we hypothesized that patients with DM would have a higher risk of tendon retear after arthroscopic rotator cuff repair. The current meta-analysis reported a significant retear risk in patients with DM and supported our hypothesis.
Well-controlled glycemic status seems to be beneficial for patients with DM in regard to tendon retear after arthroscopic rotator cuff repair. Cho et al 5 compared the retear rate after rotator cuff repair for patients with DM with poor glycemic control with the rate in those with controlled DM. They reported that the patients with uncontrolled DM had significantly greater tendon retear rates than did the patients with controlled DM. 5 However, Miyatake et al 14 found opposing results, which showed no significant between-group differences in tendon retear rate for the patients with uncontrolled DM (30.8%) and those with controlled DM (17.6%). Despite this, they still suggested intensive perioperative glycemic control and patient education for patients with uncontrolled DM. 14 In the present meta-analysis, we pooled the results and found a higher risk of tendon retear in patients with uncontrolled DM as compared with patients with controlled DM, although the result did not reach a significant difference. Furthermore, the patients with controlled DM still had a higher tendon retear risk than did the patients without DM, although it did not reach statistical significance. In order to achieve better clinical treatment outcomes in patients with DM after rotator cuff repair surgeries, further studies regarding the effect of preoperative, perioperative, and postoperative glycemic control on tendon retear risk are required in the future.
Rotator cuff tendon retear is usually associated with poorer clinical outcome scores. 24 Despite patients with DM having a higher risk of tendon retear after rotator cuff repair, the clinical outcome between patients with and those without DM seemed to be comparable. Cho et al 5 reported that the patients with DM and those without DM have equal postoperative clinical results, such as postoperative pain, range of motion, Constant score, and University of California Los Angeles score. Miyatake et al 14 also revealed that the Japanese Orthopaedic Association and University of California Los Angeles scores as well as the shoulder range of motion except internal rotation were not different between the patients with DM and those without DM at the final follow-up. However, the subgroup analysis between intact and retear rotator cuff in patients with DM was not available in the current literature.
This study has some limitations. First, the number of included studies was relatively small (n = 5), and all of them were conducted retrospectively. Therefore, additional prospective clinical studies will be needed in the future. Second, some recall bias possibly existed in the reported results because only the retrospective cohort studies or case-control studies were included in this meta-analysis. In spite of this, the sample size in this meta-analysis may have been large enough that the recall bias did not significantly influence the outcome of the study. Third, only 2 of the included studies classified the patients with DM into controlled and uncontrolled groups. Therefore, the effect of glycemic control could not be illustrated in the current study. Fourth, all included patients underwent arthroscopic rotator cuff repair surgeries. However, some of them underwent double-row suture bridge techniques, whereas the rest underwent single-row rotator cuff repairs. The selection for double-row or single-row repair was based on the surgeons’ decision and could not be controlled in this meta-analysis. Fifth, results in patients with DM undergoing open rotator cuff repair were not addressed in this study. Sixth, the different types of studies (case-control and cohort studies) included in this review could have led to clinical heterogeneity. In response to this concern, a random-effects model was used in this meta-analysis.
Conclusion
According to the results of this review, patients with DM had a 2.25 times higher risk of tendon retear after arthroscopic rotator cuff repair compared with patients without DM.
Footnotes
Acknowledgment
The authors thank the Skeleton Materials and Bio-compatibility Core Lab, Research Center of Clinical Medicine, National Cheng Kung University Hospital, Tainan, Taiwan, for assistance with this project.
Final revision submitted May 6, 2020 accepted May 26, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.