
Abstract
Background:
In patients with type 2 diabetes mellitus (DM), preoperative glycosylated hemoglobin (HbA1c) is associated with outcomes after arthroscopic rotator cuff repair (ARCR); however, the relationship between outcomes and postoperative serum glycosylated hemoglobin (HbA1c) after ARCR has not been investigated.
Purpose:
To evaluate outcomes after ARCR in patients (1) with and without DM and (2) with DM according to their pre- and postoperative HbA1c levels.
Study Design:
Cohort study; Level of evidence, 3.
Method:
Included in this study were 148 patients without DM and 35 patients with type 2 DM who underwent ARCR between January 1, 2017, and December 31, 2019. Clinical and radiological outcomes were evaluated preoperatively and at the latest clinical follow-up. Postoperative magnetic resonance imaging was performed after 12 months. In patients with type 2 DM, HbA1c levels were evaluated preoperatively as well as 6 and 12 months postoperatively; patients with an HbA1c level of ≥7% were defined as having uncontrolled DM. Multivariate logistic regression analyses were performed to determine the factors for retears after ARCR.
Results:
The retear rates after ARCR were 22.9% (8/35) and 16.9% (25/148) in patients with and without DM, respectively. The retear rates were significantly higher in the 6-month postoperative uncontrolled DM group than in the controlled DM and non-DM groups (50% vs 8.7% and 16.8%; P < .05). The odds ratio for retears in the postoperative uncontrolled DM group was 5.555 (P =0.01) compared with the non-DM group. Among the patients with DM, in the uncontrolled DM group, 6-month postoperative hyperglycemia was superior in accuracy, sensitivity, and specificity for predicting retears after ARCR than preoperative hyperglycemia (77.1% vs 62.9%, 75% vs 37.5%, and 77.8% vs 70.4%, respectively).
Conclusion:
This study demonstrated the association between uncontrolled postoperative DM and an increased risk of retears compared with no DM or controlled DM. Furthermore, postoperative HbA1c values were correlated more closely with the risk of retears than preoperative HbA1c values.
Diabetes mellitus (DM), a chronic metabolic disease, is a common and debilitating medical condition as well as a risk factor for perioperative complications. 9 DM affects various musculoskeletal disorders, impairs connective tissue healing, and reduces tissue biomechanical properties because of less fibroblast proliferation and lymphocyte infiltration in healing tendons associated with tendon weakness. 1,2,8,24
Although arthroscopic rotator cuff repair (ARCR) is an effective treatment for painful rotator cuff tears (RCTs), complications, such as infection and healing failure at the tendon-bone interface, can occur. The risk of these complications is further increased in patients with DM. # Adverse effects of DM on the tendon-bone healing process after ARCR may increase the probability of retears. 6,14,15,18,29,30 Cho et al 6 suggested that preoperative hyperglycemia increases the possibility of anatomical failure at the repaired rotator cuff. Furthermore, the risk of infection after ARCR in patients with DM increases as the perioperative serum glycosylated hemoglobin A1c (HbA1c) level increases. 5
In patients with DM, serum glucose levels are dynamic and can fluctuate during the day. Patients with DM have varying degrees of disease severity that may include additional metabolic comorbidities and vascular disease. In the many studies focused on HbA1c levels in patients with DM with ARCR, HbA1c measurements were usually performed at a single preoperative time point. 6,19,29 These studies analyzed the outcome of this single preoperative HbA1c measurement to reflect the entire postoperative course. However, we postulated that a single preoperative HbA1c measurement may not sufficiently predict clinical outcomes after ARCR.
In this study, we aimed to investigate the surgical outcomes of ARCR in patients with and without type 2 DM and the association between the surgical outcomes of patients with type 2 DM and HbA1c levels measured during the preoperative versus the postoperative course. We hypothesized (1) that surgical outcomes after ARCR would be similar between patients with well-controlled DM and those without DM and (2) that postoperative hyperglycemia would better predict retears after ARCR than preoperative hyperglycemia.
Methods
Institutional review board approval was obtained for the study protocol, and all procedures were in compliance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was obtained from all patients.
Patient Selection
Between January 1, 2017, and December 31, 2019, 395 patients underwent ARCR for full-thickness RCTs. All surgical procedures were performed by a single shoulder surgeon (I-H.J.). The postoperative follow-up was performed at 1 month, 3 months, 6 months, 1 year, and once a year after the first year. Patients with DM were consulted periodically by the endocrinology department. According to the protocol, HbA1c levels were evaluated preoperatively as well as 6 months and 12 months postoperatively. All clinical data were collected by an assigned clinical nurse specialist (J.H.P.).
Inclusion and Exclusion Criteria
The inclusion criteria of this study were as follows: Diagnosis of medium to large (≥1 and ≤5 cm) RCT with complete tear of ≤2 tendons and medial retraction of Patte grade 1 or 2 on preoperative magnetic resonance imaging (MRI). Postoperative 1-year MRI. ARCR performed by a single surgeon (I.-H.J.). Patients with type 2 DM.
The exclusion criteria of the study were as follows: Isolated subscapularis tendon tears. Concomitant superior capsular reconstruction or augmentation procedures. Previous rotator cuff surgery. <1 year of follow-up. DM patients whose HbA1c level was not observed at least once.
Of the 395 patients, 183 were observed for at least 1 year and evaluated using MRI. The mean follow-up duration was 22 months (range, 12-50 months) (Figure 1).

Flowchart of the study. ARCR, arthroscopic rotator cuff repair; DM, diabetes mellitus; f/u, follow-up; HbA1c, serum glycosylated hemoglobin; MRI, magnetic resonance imaging.
Glucose Control and Measurement of HbA1c
The American Diabetes Association (ADA) has suggested that the HbA1c target for many nonpregnant adults with DM be <7% (53 mmol/mol) without significant hypoglycemia. 3 To classify the severity of sustained hyperglycemia in the DM group, patients with an HbA1c level of ≥7% were defined as patients with uncontrolled DM, and those with an HbA1c level of <7% were considered patients with controlled DM according to the ADA. 3
Data Collection
The visual analog scale for pain (pVAS), American Shoulder and Elbow Surgeons (ASES), and Single Assessment Numeric Evaluation (SANE) scores were assessed before and after surgery. The following data were collected from the patients: age, sex, body mass index (BMI), medical history, Charlson Comorbidity Index (CCI), smoking status, and DM morbidity period. Moreover, imaging and operative data, such as tear size according to preoperative MRI scan and operative findings (partial, small, medium, large, or massive), 25 Goutallier fatty infiltration, 11 and repair configuration (single or double row), were collected. Postoperative MRI was performed at 12 months. Retear was defined as Sugaya type 4 and 5 classifications. 28 All imaging studies were analyzed by a fellowship-trained shoulder surgeon (D.M.K.) who was not involved in the surgery and who was blinded to the identifying information of the patients and clinical outcomes
Statistical Analysis
Data distribution was assessed using the Kolmogorov-Smirnov test. An independent t test was used to evaluate the difference between the non-DM and DM groups according to age, follow-up period, BMI, tear size, pVAS score, and clinical score. The Pearson chi-square test and Fisher exact probability test were used to evaluate the difference between these 2 groups according to sex, CCI score, age-adjusted CCI score, smoking status, retear, tear size, Goutallier fatty infiltration, repair configuration, and dominant side. An independent t test was used to evaluate the difference in HbA1c between the healing and retear groups among patients with DM.
Univariate and multivariate logistic regression analyses were performed to determine factors for retears after ARCR. Univariate analysis was performed using the chi-square test or Fisher exact test for categorical variables and a t test for continuous variables. Multivariate logistic regression analysis was performed on variables with P values of >.20, which was followed by the calculation of odds ratios (ORs).
Many patients were included in duplicates in the uncontrolled DM group at 6 and 12 months, which could cause confounding if both groups were included in the multivariate analysis. Therefore, only the postoperative uncontrolled DM groups at 6 months were included in the multivariable analysis to ensure accurate results were obtained. Significance was set at a level of .05 with associated 95% CIs. SPSS Version 21.0 (IBM Corp) was the software program used for all statistical analyses.
Results
Demographic Data
Demographic data are shown in Table 1. Demographic data were not statistically different, except for CCI and age-adjusted CCI, between the non-DM and DM groups. The DM group had preoperative HbA1c ranging from 6% to 8.4%.
Patient Demographics a
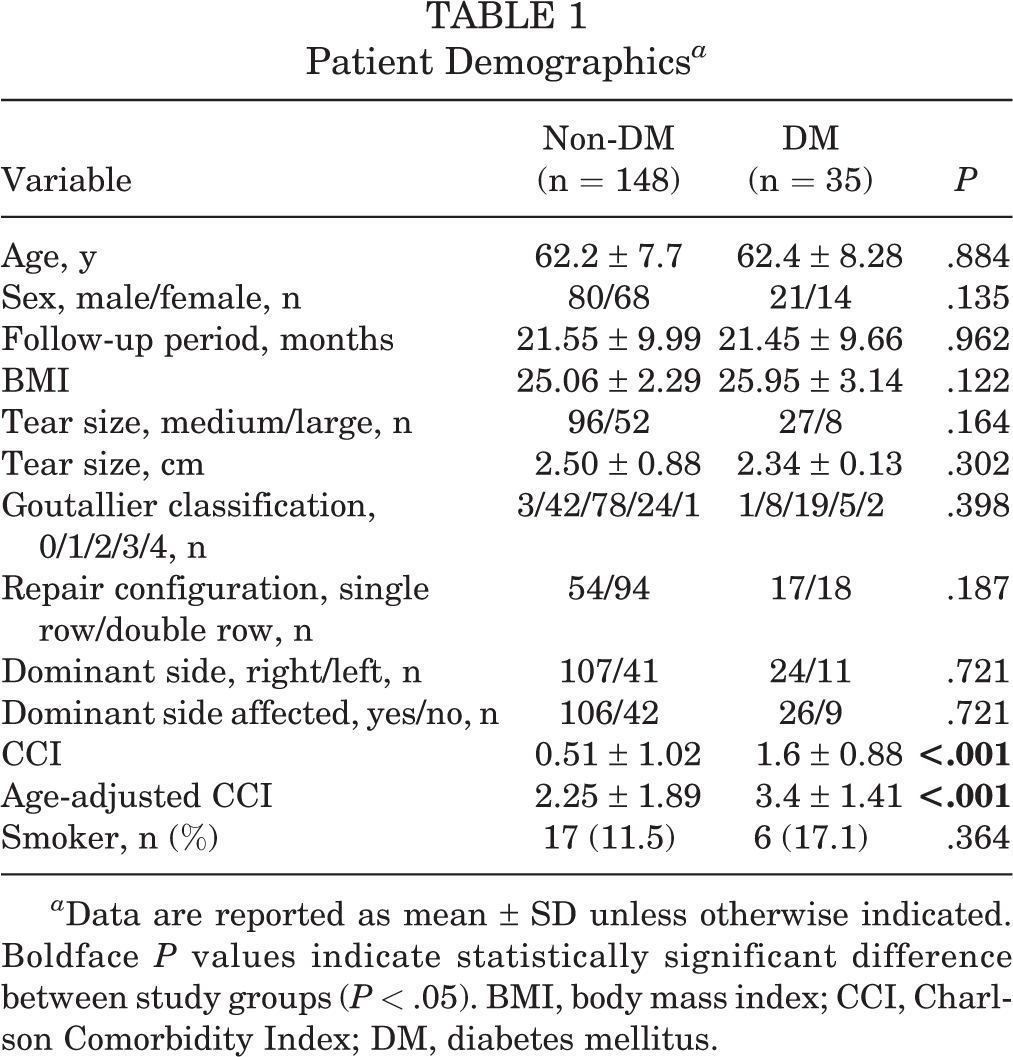
a Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant difference between study groups (P < .05). BMI, body mass index; CCI, Charlson Comorbidity Index; DM, diabetes mellitus.
Comparison of Clinical Outcomes Between Non-DM and DM Groups
The clinical score assessed using the pVAS, ASES, and SANE scores showed significant improvement in both the DM (P < .001) and the non-DM (P < .001) groups (Table 2). The preoperative ASES and SANE scores of the DM group were significantly lower than those of the non-DM group (P = .003 and P = .032, respectively); however, the scores at the final follow-up were not significantly different between the groups (Table 2). In this study, 183 patients satisfied the inclusion criteria. Among the 148 patients without DM, 25 (16.9%) had retears, and, of the 35 patients with DM, 8 (22.9%) had retears. No statistically significant difference was found between the 2 groups (Table 3).
Comparison of Preoperative and Postoperative Clinical Scores Between Groups a

a Data are reported as mean ± SD. Boldface P values indicate statistically significant difference between study groups (P < .05). ASES, American Shoulder and Elbow Surgeons; DM, diabetes mellitus; pVAS, visual analog scale for pain; SANE, Single Assessment Numeric Evaluation.
Comparison of Retear Rates Between Groups a

a Data are reported as n (%). DM, diabetes mellitus.
Comparison of Retear Rates According to Preoperative and Postoperative HbA1c Levels
Subgroup analyses were performed to analyze the retear rate based on the preoperative and postoperative HbA1c levels. Based on the preoperative HbA1c level, 5 of 24 patients in the controlled group had retears and 3 of 11 patients in the uncontrolled group had retears, which was not statistically significant (Table 4). In contrast, according to the 6-month and 12-month postoperative HbA1c levels, 2 of 23 patients and 2 of 21 patients in the controlled group had retears, and 6 of 12 patients and 6 of 14 patients in the uncontrolled group had retears (Table 4). The postoperative uncontrolled DM groups showed statistically significant higher retear rates compared with the controlled group and the non-DM group (Table 4). Moreover, when using HbA1c levels at 6 and 12 months postoperatively, the accuracy, positive predictive value, sensitivity, and specificity were higher than those for preoperative HbA1c levels (Table 5). 12
Comparison of Retear Rates According to Preoperative and Postoperative HbA1c Levels a

a DM, diabetes mellitus; HbA1c, serum glycosylated hemoglobin.
b Results of comparisons between the (1) non-DM and controlled DM groups, (2) non-DM and uncontrolled DM groups, and (3) controlled DM and uncontrolled DM groups. Boldface P values indicate statistically significant differences between groups compared (P < .05).
Diagnostic Values of Preoperative and Postoperative HbA1c Levels for Predicting Retear a
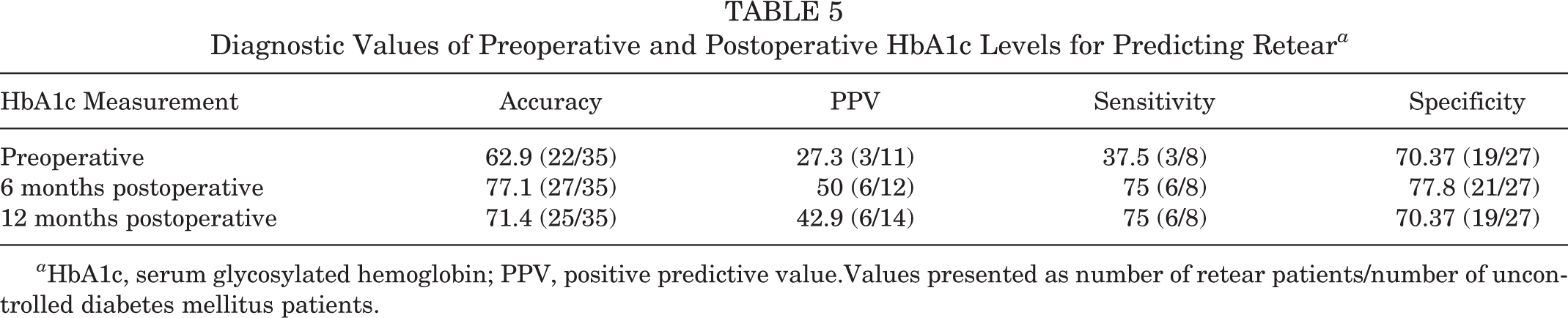
a HbA1c, serum glycosylated hemoglobin; PPV, positive predictive value.Values presented as number of retear patients/number of uncontrolled diabetes mellitus patients.
There were no differences in preoperative HbA1c levels between patients with DM with retears versus those with healed rotator cuffs; however, patients with retears presented with higher HbA1c levels than the healed group at 6 and 12 months postoperatively (P < .05) (Figure 2). Moreover, in the patients DM with retears, postoperative HbA1c levels increased compared to preoperative HbA1c levels in 7 of 8 patients (87.5% ).

Preoperative (Preop) and postoperative (Postop) HbA1c levels in the diabetes mellitus (DM) group. The dashed red line indicates the threshold HbA1c level for controlled DM according to the American Diabetes Association. 3 *Statistically significant difference between patients with DM with versus without retear (P < .05). HbA1c, serum glycosylated hemoglobin.
Factors Affecting Retear
In the univariate logistic regression analysis, age, BMI, uncontrolled DM according to 6-month postoperative HbA1c, Goutallier fatty infiltration, and age-adjusted CCI score met the criteria and were included in the multivariate logistic analysis. In the multivariate analysis, age and Goutallier fatty infiltration had significantly higher ORs for retears (1.062 [95% CI, 1.007-1.120], P = .028; and 1.866 [95% CI, 1.045-3.330], P = .035, respectively). Patients with uncontrolled DM at 6 months postoperatively showed higher OR for retears (5.555 [95% CI, 1.510-20.437]; P = .010) (Table 6).
Results of Binary Logistic Analysis of Retear After ARCR a

a Boldface P values indicate statistical significance (P < .05). ARCR, arthroscopic rotator cuff repair; BMI, body mass index; CCI, Charlson Comorbidity Index; DM, diabetes mellitus; HbA1c, serum glycosylated hemoglobin; NA, not applicable; OR, odds ratio.
Discussion
The postoperative HbA1c levels served as a reliable predictor of retears following ARCR in patients with DM compared with preoperative HbA1c levels. The 6-month postoperative HbA1c levels exhibited better accuracy, sensitivity, and specificity for predicting retears than preoperative HbA1c levels. Following ARCR, the retear group tended to have higher HbA1c levels than the healed group, and the difference in HbA1c levels between the retear and healed groups increased between 6 and 12 months postoperatively.
In patients with postacute coronary syndrome, a lower HbA1c level was independently associated with a lower risk of major adverse cardiac and cerebrovascular events, and maintaining a lower HbA1c level after discharge was strongly recommended. 21 Previous studies have found a relationship between HbA1c levels and clinical outcomes after ARCR. Despite efforts to correlate this preoperative parameter with the entire postoperative course of the disease, HbA1c levels were measured at a single preoperative time. 6,19 Few studies have focused on the correlation between postoperative HbA1c levels and surgical and clinical outcomes after orthopaedic surgery. After total joint arthroplasty surgery, postoperative glucose levels are related to infection; however, most studies only measured glucose levels after surgery. 16,27 In an animal study, poor glycemic control significantly affected soft tissue repair and reconstruction by creating a hyperglycemic environment before and after surgery. 4
HbA1c levels reflect glucose levels over the past 3 months, and the ADA recommends glycemic status assessment (HbA1c or other glycemic measurements) at least twice a year in patients with DM. 3,22 In addition, glucose levels can fluctuate daily in patients with DM. Therefore, preoperative evaluation of HbA1c may not sufficiently represent the overall state of DM. This study showed that a single preoperative HbA1c level was not a reliable predictor of repair integrity following ARCR surgery and that continuous HbA1c management is recommended postoperatively. Recently, Shohat et al 26 suggested that fructosamine, a measure of the average glucose levels over a time period of 2 to 3 weeks, is an excellent predictor of complications following total joint arthroplasty. However, they measured the fructosamine levels only once within 30 days before surgery.
In this study, among patients with DM, the retear group had higher postoperative HbA1c levels than preoperative HbA1c levels, whereas HbA1c levels were maintained steadily between the pre- and postoperative periods in the healed group. Postoperative HbA1c levels increased in 7 of 8 patients (87.5%) in the retear group. Uncontrolled postoperative glucose levels may adversely affect the healing process, resulting in healing failure after ARCR. Hence, we recommend the continuous management of blood glucose levels to improve outcomes after ARCR in patients with DM.
Patients with DM were informed before surgery that hyperglycemia could affect the surgical outcome and that they should avoid it by changing their lifestyle and seeking management from an endocrinologist. However, if hyperglycemia was not controlled before surgery, the patient was given intensive care by an endocrinologist, and surgery was sometimes postponed. The temporarily controlled preoperative HbA1c levels had no positive effects on surgical outcomes in this study. Lifestyle modification for maintaining euglycemia after surgery may be necessary to preserve the integrity of the repaired tendon. Similarly, in a recent study, perioperative hyperglycemia did not have an association with rates of revision rotator cuff surgery within 2 years of follow-up. 5
Ultimately, patients with DM should control their glucose levels to prevent vascular events, and vascular events occur more frequently in patients with poor glycemic control. 10 As numerous vascular complication–related DM studies are constantly evaluating and managing HbA1c, there is still scope for improvement when it comes to recognizing DM as a risk factor in orthopaedic surgery. 3 When considering DM as a risk factor for rotator cuff healing, serum HbA1c levels should be continuously monitored and managed. Continuous glucose level management both before and for a period of time after surgery needs to be recognized as an important measure that helps in preservation of rotator cuff integrity.
Limitations
This study has several limitations. First, the retrospective study had a relatively short follow-up period. Therefore, the long-term metabolic effects of uncontrolled glucose levels on tendon-bone healing after ARCR were not evaluated. Second, selection bias may have occurred, as patients with high morbidity or multiple systemic diseases associated with DM were excluded; in addition, surgery was postponed in patients with remarkably elevated HbA1c levels. Third, the generalization to a larger population is limited due to the small number of patients with DM enrolled in the study. Despite this limitation, the study demonstrated that high postoperative HbA1c levels are associated with healing failure after ARCR. Finally, the DM and non-DM groups had unequal numbers of patients and different preoperative clinical scores. As a result, the extrapolation of the data is limited due to the dissimilar clinical conditions between the 2 groups.
Conclusion
This study demonstrated the association between uncontrolled postoperative DM and an increased risk of retears compared with no DM or controlled DM. Furthermore, postoperative HbA1c values were correlated more closely with the risk of retears than preoperative HbA1c values. Therefore, maintaining glycemic control in the postoperative period may help preserve rotator cuff integrity following repair.
Footnotes
Notes
Final revision submitted September 12, 2022; accepted September 26, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Asan Medical Center (ref No. S2021-1507-0001).