
Abstract
Background:
The teres minor is a critical component of the rotator cuff and serves as one of the few external rotators of the humerus. Information is lacking regarding the effect of teres minor atrophy in isolation and in the setting of concomitant full-thickness rotator cuff tears on outcomes in patients undergoing rotator cuff surgery.
Purpose:
To investigate the effect of preoperative teres minor fatty infiltration on postoperative clinical outcomes in patients with and without full-thickness rotator cuff pathology.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review of patients undergoing primary arthroscopic shoulder surgery between 2014 and 2016 was performed. Preoperative magnetic resonance imaging was used to determine fatty infiltration for each rotator cuff muscle using the modified Goutallier classification. American Shoulder and Elbow Surgeons (ASES) as well as the shortened version of Disabilities of the Arm, Shoulder and Hand (QuickDASH) scores were obtained preoperatively and during follow-up. Exclusion criteria included prior surgery on the ipsilateral shoulder or a diagnosis of inflammatory arthropathy. For analysis, patients were dichotomized to grade 0 or grade 1-4 atrophy of the teres minor as well as to full-thickness or partial-thickness rotator cuff pathology.
Results:
A total of 36 of 47 (76.6%) patients (mean age, 63 years; range, 45-76 years) were available for postoperative follow-up at a mean of 40 months (range, 30-48 months). Postoperative ASES score was significantly higher and QuickDASH score was significantly lower among all patients in the grade 0 group compared with the grade 1-4 group. Postoperative ASES and QuickDASH scores were not significantly different in patients with partial-thickness rotator cuff tears at any time point. However, the postoperative ASES score was significantly higher and QuickDASH score was significantly lower in the grade 0 versus grade 1-4 group for patients with full-thickness rotator cuff pathology.
Conclusion:
Preoperative teres minor atrophy in patients undergoing surgery for rotator cuff pathology may impair postoperative clinical outcomes, especially in patients with full-thickness tears.
Rotator cuff tears represent the most common injury affecting the upper extremity and are a major cause of disability. 9 The prevalence of rotator cuff pathology increases with advancing patient age, with >50% of patients older than 80 years having full-thickness tears. 33 Most rotator cuff tears result from chronic degeneration, from either intrinsic or extrinsic factors, which compromises the quality and integrity of the tendons and leads to progressive tearing and failure. 34 Surgical repair is effective at treating pain and disability associated with a rotator cuff tear, even though postoperative retearing is common. 2,16
The teres minor is a critical component of the rotator cuff and serves as one of the few external rotators of the humerus. Although isolated tears of the teres minor can occur, 19,20 most tears develop in association with massive rotator cuff pathology and can be associated with teres minor atrophy. 22 Atrophy may also result from either quadrilateral space syndrome 1,24 or compression of the primary motor nerve to the teres minor. 3,6 Isolated teres minor atrophy without full-thickness rotator cuff pathology has an incidence between 0.8% and 5.5% in persons with shoulder pain. 5,32,35
Although fatty infiltration of the rotator cuff musculature has been associated with increased retear rates after surgical repair, there is mixed evidence that this is associated with decreased functional outcomes. 18 It has been reported, however, that preoperative fatty infiltration of the teres minor does not affect functional outcomes after rotator cuff repair. 21 As such, it is still to be confirmed whether preoperative teres minor atrophy is associated with decreased postoperative functional outcome scores in not only patients with full-thickness rotator cuff tears but also in those with non–full thickness rotator cuff pathology.
The purpose of this study was to investigate the effect of preoperative teres minor fatty infiltration on postoperative clinical outcomes in patients with and without full-thickness rotator cuff pathology. We hypothesized that patients with preoperative fatty infiltration of teres minor would have inferior clinical outcomes compared with patients without evidence of teres minor changes.
Methods
A retrospective review of all patients undergoing shoulder surgery with the senior author (G.D.A.) between January 2014 and June 2016 was conducted after obtaining approval from our institutional review board. Inclusion criteria were patients 18 years of age and older who had rotator cuff repair or debridement. Patients were excluded from the study if they had acute rotator cuff pathology, any previous open or arthroscopic operation of the ipsilateral shoulder, a diagnosis of inflammatory arthropathy, deltoid atrophy on preoperative magnetic resonance imaging (MRI), or a space-occupying lesion in the quadrilateral space (Figure 1).

Flowchart demonstrating patient selection process for study inclusion. MRI, magnetic resonance imaging.
Before surgery, all patients received at least 3 months of formal physical therapy or a home exercise program as well as a subacromial corticosteroid injection. All patients also underwent an MRI prior to their surgical date. Patients with persistent symptoms were indicated for surgery. The treating surgeon rendered treatment based on the degree of rotator cuff pathology intraoperatively. Full-thickness tears were treated with rotator cuff repair, and partial-thickness tears were treated with rotator cuff debridement and subacromial decompression. Massive, irreparable rotator cuff tears were treated with debridement and either a long head of biceps tendon tenodesis or tenotomy, if the biceps tendon was present.
Preoperatively, the American Shoulder and Elbow Surgeons (ASES) score 26 as well as the shortened version of Disabilities of the Arm, Shoulder and Hand (QuickDASH) score 17 were obtained, as it was for all patients undergoing shoulder surgery. Descriptive data including sex, body mass index (BMI), history of diabetes, and smoking history were also recorded. Concomitant surgical procedures were determined based on operative report review. Postoperative follow-up scores using ASES and QuickDASH were calculated at a minimum of 2-year follow-up. Standard postoperative protocols were provided to patients and their physical therapists.
Preoperative MRI scans were used to determine fatty infiltration for each rotator cuff muscle based on the modification of the Goutallier classification 10 for use with MRI. 7,30 Measurements were made on sagittal cuts at the coracoid base. The amount of retraction in the mediolateral plane (if any) was determined by measuring the maximum retraction distance of the supraspinatus or infraspinatus tendon edge from the medial footprint on coronal oblique images. Tear size was determined by measuring the maximum anterior-posterior size on sagittal oblique images. Two independent observers (E.J.S., G.D.A.) recorded each measurement, and the mean was calculated.
Teres minor atrophy assessment within the overall cohort was dichotomized to patients with grade 0 atrophy of the teres minor on preoperative MRI scan versus those with grade 1-4 atrophy of the teres minor. Within each of these groups, the Goutallier grading was reported as mean ± SD. Subgroup analysis within each of these 2 teres minor cohorts was also separately performed among patients with partial-thickness rotator cuff pathology versus full-thickness tears. Shapiro-Wilks tests for normality were used, and comparisons of continuous variables were made with Student t tests and Mann-Whitney U tests, as dictated by normality testing. Dichotomous variables were analyzed with chi-square and Fisher exact tests. To adjust for confounding variables among the population, analysis of covariance was used, with adjusted means and confidence intervals reported. Correlation among the amount of atrophy of the various rotator cuff muscles was performed with the Spearman rank correlation coefficient.
An a priori power analysis with parametric means testing (Student t test) indicated the need for 34 patients to reach a power of 80% with a P value of .05 (and an effect size of 1) when using postoperative ASES as our primary outcome measure (Version 3.1.2; G*Power). We used R (Version 3.6.1; Foundation for Statistical Computing) for analysis, and an alpha level of .05 was set as significant.
Results
Of the 47 patients meeting inclusion and exclusion criteria, 36 patients (76.6%) were available for postoperative follow-up at a mean of 40 months (range, 30-48 months). The 11 excluded patients did not respond to requests for follow-up. A total of 18 patients had grade 0 teres minor changes whereas 18 patients had grade 1 or greater atrophy. For the overall cohort, mean age at the time of surgery was 63 years (range, 45-76 years), and all patients were male. No significant difference was found in maximum tear size between the 2 groups. Baseline descriptive, imaging, and surgical data for the 2 groups are presented in Table 1.
Descriptive, Imaging, and Surgical Data for All Patients Dichotomized Based on Teres Minor Atrophy Grade a

a Data are reported as mean ± SD or No. of participants. RTC, rotator cuff.
b Full-thickness tear group.
No significant difference was seen in preoperative ASES or QuickDASH scores between the 2 teres minor atrophy groups. Both 1-year and 2-year postoperative ASES and QuickDASH scores, however, were significantly better in the grade 0 group versus the grade 1-4 group. Additionally, the absolute value of the pre- to postoperative ASES change was significantly larger in the grade 0 group versus the grade 1-4 group (Table 2). After adjustment for BMI differences between the grade 0 and grade 1-4 groups, both postoperative QuickDASH (P = .026; adjusted mean, 15.0 [95% CI, 3.7-26.3] vs 33.9 [95% CI, 22.2-45.5]) and postoperative ASES (P = .011; adjusted mean, 83.4 [95% CI, 71.3-95.4] vs 60.0 [95% CI, 47.6-72.4]) maintained a significant improvement. Significant differences between the grade 0 group and grade 1-4 group also remained after adjustment for the presence of diabetes for postoperative ASES (P = .006; adjusted mean, 85.3 [95% CI, 72.9-97.6] vs 59.4 [95% CI, 47.1-71.9) as well as postoperative QuickDASH (P = .007; adjusted mean, 12.3 [95% CI, 0.9-23.8] vs 35.5 [95% CI, 24.1-46.9]).
Postoperative Outcome Scores Among All Patients Dichotomized Based on Teres Minor Atrophy Grade a
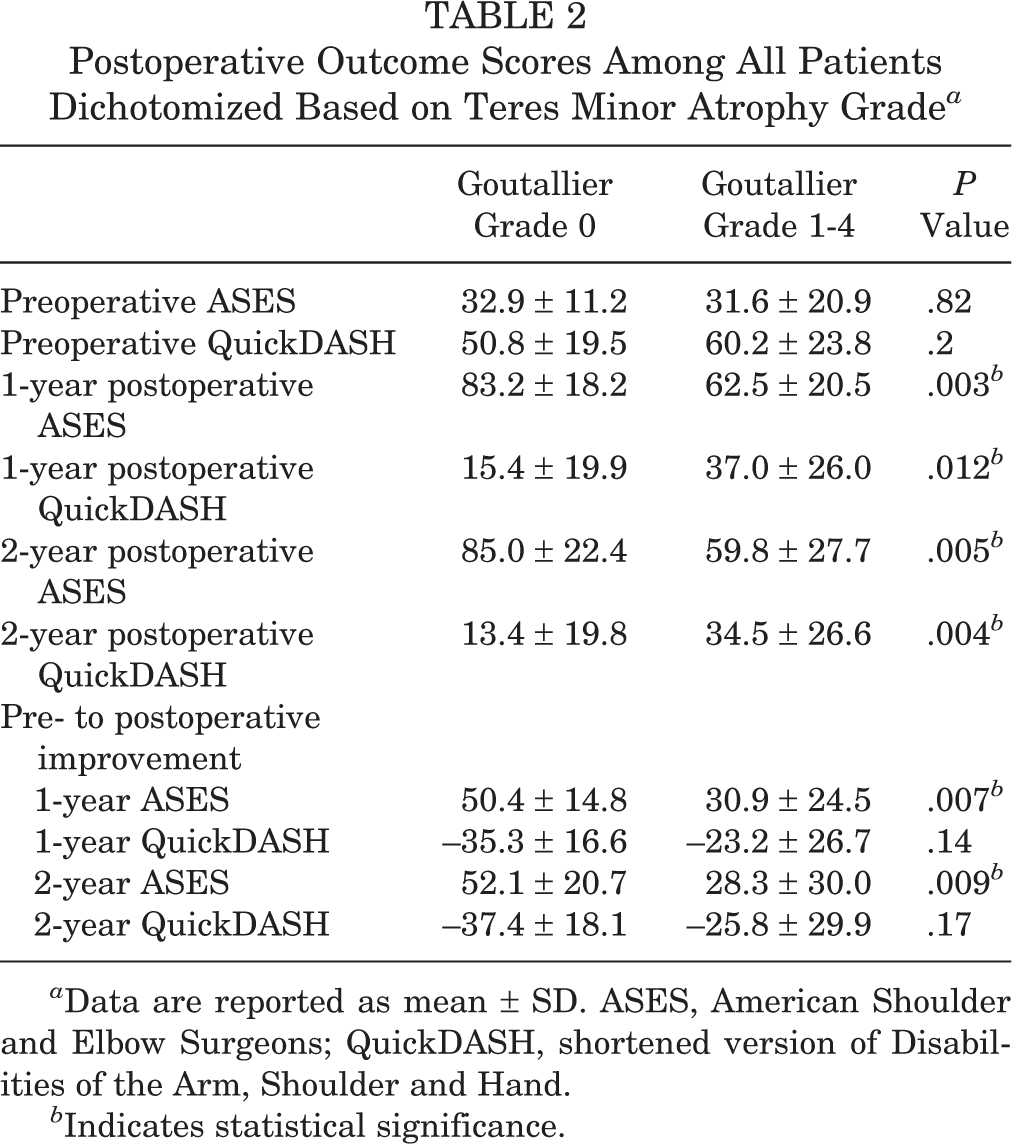
a Data are reported as mean ± SD. ASES, American Shoulder and Elbow Surgeons; QuickDASH, shortened version of Disabilities of the Arm, Shoulder and Hand.
b Indicates statistical significance.
When analyzing the subgroup of patients with partial-thickness tears, we found no significant difference in outcome scores between those with grade 0 and grade 1-4 atrophy of the teres minor (Table 3). However, when evaluating only patients with full-thickness rotator cuff pathology undergoing repair, we noted that postoperative ASES and QuickDASH scores were significantly better for the grade 0 group (Table 4).
Postoperative Outcome Scores for Patients With Partial-Thickness Rotator Cuff Tears Dichotomized Based on Teres Minor Atrophy Grade a

a Data are reported as mean ± SD. ASES, American Shoulder and Elbow Surgeons; QuickDASH, shortened version of Disabilities of the Arm, Shoulder and Hand.
Scores for Patients With Full-Thickness Rotator Cuff Tears (Including Massive Irreparable Tears) Dichotomized Based on Teres Minor Atrophy Grade a
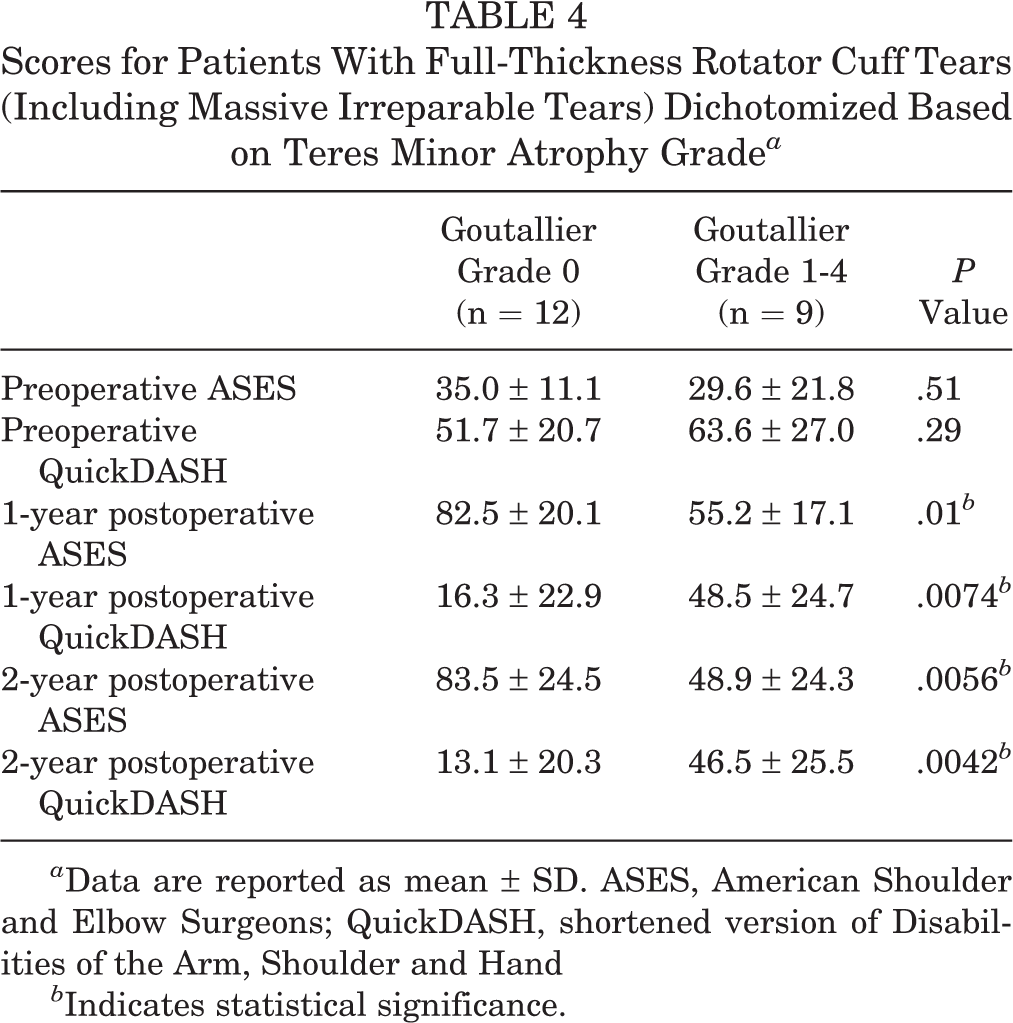
a Data are reported as mean ± SD. ASES, American Shoulder and Elbow Surgeons; QuickDASH, shortened version of Disabilities of the Arm, Shoulder and Hand
b Indicates statistical significance.
A significant correlation was found for the overall cohort between the severity (modified Goutallier score) of teres minor atrophy and atrophy of the infraspinatus (r = 0.499; P = .002) but not atrophy of the supraspinatus (r = –0.002; P = .99) or subscapularis (r = 0.320; P = .057). These findings were also found in the subgroup analysis, with the exception that patients undergoing rotator cuff repair demonstrated a significant correlation between subscapularis and teres minor atrophy (Table 5).
Correlations Between Rotator Cuff Atrophy Scoring for Those Undergoing Rotator Cuff Debridement and Repair

a Indicates statistical significance.
Discussion
The findings of our study support our hypothesis that surgical treatment of rotator cuff disease in patients with evidence of preoperative teres minor fatty infiltration leads to inferior clinical outcomes compared with similar patients without teres minor atrophy, particularly in those with full-thickness rotator cuff pathology. Postoperative ASES score was increased and QuickDASH score was decreased in all patients without teres minor atrophy compared with those who had teres minor atrophy. Within the subgroup analysis, the group with full-thickness pathology and grade 0 atrophy demonstrated significantly better postoperative outcomes scores versus those with full-thickness tears and grade 1-4 atrophy. Additionally, teres minor fatty infiltration correlated with atrophic changes of the infraspinatus and the subscapularis muscles but not the supraspinatus.
Fatty infiltration of rotator cuff musculature has been associated with an increased risk of rotator cuff retear after surgical repair, but its effect on functional outcomes after surgical intervention is less clear. 18 Kim et al 21 reported clinical and MRI outcomes after rotator cuff repair in patients with and without teres minor atrophy. In their matched cohort analysis, those investigators found no significant functional outcome score differences between the groups or any change in teres minor fatty infiltration 1 year after surgery. The findings of Kim et al contrast with those of our study, potentially owing to our inclusion of patients with massive, irreparable rotator cuff tears. Studies on other rotator cuff muscles have indicated a mixed correlation between degree of preoperative atrophy and postoperative shoulder function. 8,11 –14,25 One randomized controlled trial found no significant difference in functional outcome after surgical repair between patients with absent or scant supraspinatus fat infiltration and patients with advanced fat infiltration. 15 Alternatively, another prospective study observed a positive correlation between low preoperative supraspinatus fat infiltration and improved postoperative outcomes in a series of >100 shoulders after 2 years of follow-up. 27
Our results indicate that the teres minor muscle may be most important for functional outcomes in patients with already compromised rotator cuffs. Teres minor integrity has been shown to be important in latissimus dorsi tendon transfers for treating massive irreparable rotator cuff tears. 4,28,29 A normal teres minor or one with minimal atrophy is predictive of successful outcomes after latissimus dorsi tendon transfers, 4 whereas high-grade fatty infiltration leads to inferior clinical outcomes of reverse total shoulder arthroplasty compared with those without teres minor atrophy. 31 Although we identified a correlation between teres minor fatty infiltration with atrophic changes of the infraspinatus and subscapularis, hypertrophic changes to the teres minor have been noted in posterosuperior rotator cuff tears in the presence of infraspinatus atrophy. 19 In these studies, progression of infraspinatus atrophy appeared to induce development of compensatory teres minor hypertrophy and subsequently led to greater strength of external rotation in such patients compared with those who had a normal or atrophic teres minor. 20 An understanding of the effect of fatty infiltration on rotator cuff tears may allow clinicians to implement unique shoulder rehabilitation programs to improve functionality in those patients at increased risk for poor postoperative outcomes.
The clinical implication of isolated teres minor atrophy in the setting of an intact rotator cuff, such as in a younger patient, remains unclear. Isolated teres minor atrophy is a clinically distinct form of shoulder pathology. The clinical presentation of teres minor atrophy is variable but can be asymptomatic or may include posterior shoulder pain and weakness with abduction and external rotation (hornblower position) not associated with paresthesia or quadrilateral space point tenderness. 6,22,23 Anatomic sources proposed as a cause of isolated teres minor atrophy include fibrous bands in the quadrilateral space 1,24 or a stout fascial sling, 3 some of which may spare the axillary nerve and lead to isolated compression of the motor branch to the teres minor. Previous studies based on cadaveric dissection have also revealed considerable anatomic variation of axillary nerve length from both its origin at the posterior cord to its bifurcation into posterior and anterior branches, which may increase the risk of impingement and subsequent isolated teres minor atrophy. 6 A case series showed relief of symptoms and clinical improvement in patients undergoing open decompression of the axillary nerve for isolated teres minor atrophy. 22
The limitations of this study include the retrospective design and inherent biases of a relatively small number of patients. For simplicity, study participants were organized in such a manner as to compare functional outcomes after rotator cuff surgery of patients with absolutely no evidence of teres minor atrophy (Goutallier 0) versus patients with any evidence of teres minor atrophy (Goutallier 1-4). Including patients with irreparable tears was important to identify any association with teres minor fatty infiltration and function, but it introduced heterogeneity and may have limited generalizability, as did our exclusively male patient population. Although varying degrees of teres minor atrophy may produce differences in outcomes, this was not the objective of the current study. A future study may investigate this relationship further.
Outcome scores assessing clinical examination parameters were not used, which could have provided additional functional measures such as range of motion and strength. Additionally, postoperative MRI studies were not obtained to evaluate potential changes in degree of fatty infiltration of the rotator musculature. Last, we may have been underpowered to detect outcome differences in our subgroup without full-thickness rotator cuff pathology.
In conclusion, preoperative teres minor atrophy in patients undergoing surgery for rotator cuff pathology may impair postoperative clinical outcomes, especially for patients with full-thickness pathology.
Footnotes
Final revision submitted May 3, 2020; accepted May 18, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.D.A. has received educational support from Arthrex, Evolution Surgical, and Stryker and consulting fees from Cytonics, Fidia Pharma, RubiconMD, and Sideline Sports Doc and has stock/stock options in Cytonics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Stanford University (protocol ID 30479).